A Comparative Study of Outcomes of PFN (Proximal Femoral Nail) And PFN A2 (Proximal Femoral Nail Antirotation) in Elderly Patients with Trochanteric Fractures.
A Comparative Study of Outcomes of PFN (Proximal Femoral Nail) And PFN A2 (Proximal Femoral Nail Antirotation) in Elderly Patients with Trochanteric Fractures.
Dr. Dinesh Kumar *1, Dr Vikramjit Singh 2, Dr Raminder Singh 3, Dr Hrushikesh Sen 4,
Dr Roopam Preet Singh Sethi 5
1, 2. Senior Resident, Government Medical College, Amritsar.
3. Assistant Professor, Government Medical College, Amritsar.
4. Junior Resident, Government Medical College, Amritsar.
5. Junior Resident, Government Medical College, Amritsar.
*Correspondence to: Dr. Dinesh Kumar, Senior Resident, Government Medical College, Amritsar.
Copyright
© 2023 Dr. Dinesh Kumar. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 26 August 2023
Published: 01 September 2023
Abstract
Background: The management of intertrochanteric fractures in the elderly offers difficulties in terms of achieving stable fixation and favorable postoperative results. There is a dearth of clinical evidence comparing the widely used Proximal Femoral Nail (PFN) and Proximal Femoral Nail Antirotation (PFNA) implants, particularly in the context of osteoporosis.
Aim: To compare the clinical and radiological outcomes of PFN and PFNA in the elderly patient with intertrochanteric fracture.
Materials and Methods: Patients with unstable intertrochanteric fractures (AO 31.A2 and 31.A3) were enrolled in the study and were treated with either PFN or PFNA. Singh's index was used to grade osteoporosis in preoperative radiographs of the normal side. Significant was defined as a grade of 3 or less. Postoperative radiographs were evaluated for tip-apex distance, Cleveland index, and reduction quality. Patients were followed for at least nine months, and any problems were reported. At the final follow-up, the Harris Hip Score and Parker-Palmer Mobility Score were used to compare functional outcomes. The unpaired t-test/Mann-Whitney U test and the Chi-square test/Fisher's exact test were used for statistical analysis. A p-value of 0.05 was deemed significant.
Results: The study included 44 patients with intertrochanteric fractures, of which 20 were treated with PFN and 24 with PFNA. Average age of PFN group was 60.78 years and of PFNA group was 74.12 years. In PFN group 8 patients (38.09%) and in PFNA group 13 patients (54.1%) had Singh’s osteoporotic index of ≤ 3. The average Harris Hip Score was 75.37 and 78.85 in PFN and PFNA groups (p=0.54) respectively.
From PFN and PFNA groups, 35% and 32% patients respectively were able to return to pre-injury mobility status as assessed by the Parker-Palmer mobility score (p=0.83). Out of eight implant related complications; seven were in patients treated with PFN (p=0.02). Among patients with Singh’s grade ≤ 3, 3 (37.5%) in PFN group suffered from implant failure whereas all 13 patients in PFNA group had successful outcome (p=0.04).
The study comprised 44 patients with intertrochanteric fractures, 20 of whom were treated with PFN and 24 with PFNA. The average age of the PFN group was 60.78 years, whereas the PFNA group was 74.12 years. Singh's osteoporotic index was 3 in the PFN group (8 patients) and 13 patients (54.1%) in the PFNA group. In the PFN and PFNA groups, the average Harris Hip Score was 75.37 and 78.85, respectively (p=0.54). According to the Parker-Palmer mobility score, 35% and 32% of PFN and PFNA patients, respectively, were able to restore to pre-injury mobility status (p=0.83). Seven of the eight implant-related problems occurred in individuals who received PFN (p=0.02). Implant failure occurred in 3 (37.5%) of patients with Singh's grade 3 in the PFN group, while Three (37.5%) patients in the PFN group had implant failure, whereas all 13 patients in the PFNA group had a favorable outcome (p=0.04).
Conclusion: Although the functional outcomes of both implants were comparable (p=0.83), the number of implant-related problems was lower with PFNA (p=0.02), especially in the osteoporotic group (p=0.04). We urge that the PFNA be used in unstable fractures, particularly in the elderly osteoporotic population.
Keywords: Cephalomedullary Nail, Proximal femoral Nail, Proximal Femoral Nail Anti rotation, Osteoporosis, Singh’s index, Harris hip Score.
A Comparative Study of Outcomes of PFN (Proximal Femoral Nail) And PFN A2 (Proximal Femoral Nail Antirotation) in Elderly Patients with Trochanteric Fractures.
Introduction
Intertrochanteric fractures of the femur are highly prevalent in older osteoporotic patients. Recumbency after a hip fracture has been linked to an increase in mortality in this patient population. In order to achieve satisfactory reduction and early mobilization in the older osteoporotic individual, surgical therapy is currently the acknowledged standard of care [1]. Because implant failure has disastrous complications and revision surgery is a highly morbid procedure due to these patients' poor general condition, obtaining a successful fixation is of paramount importance in this group of patients; thus, evidence regarding the ideal implant that would provide enduring fixation for such fractures has been a topic of ongoing research for several years.
The dynamic hip screw, which has become the gold standard treatment for stable fractures, has been proven to be ineffective in the treatment of the unstable class of intertrochanteric fractures [2]. The use of an intramedullary nail in conjunction with a dynamic femoral head/neck stabilization implant is the best option for fixing unstable fractures [3]. Various nail designs featuring a single compression screw or a compression screw coupled with an antirotation screw, such as the PFN, have gained popularity for treating unstable fractures over time. Although PFN proved to be superior to extramedullary implants for unstable intertrochanteric fractures, screw cut-out, back out, varus collapse, and rotational instability remained important postoperative problems, with literature reporting up to 31% complication rates [4].
The PFNA was created to improve femoral head and neck stability by using a single helical blade rather than a screw system for fixation. The helical blade is supposed to improve the bone-implant interface and cause cancellous bone compaction, resulting in high fixation stability [5]. The blade appears to give additional anchoring, particularly in osteoporotic bone, because it can be placed without reaming out bone from the head/neck fragment. Biomechanical investigations have shown that the helical blade has higher resistance to rotation and varus collapse due to the compaction of cancellous bone around it [6]. Clinical investigations are required to confirm whether this enhanced biomechanical performance affects functional outcomes and complication rates. However, research on helical blade fixation has revealed that, like other implant designs, it can be associated with cut-through into the hip joint, cut-out, and back-out [7].
The purpose of this prospective clinical trial was to examine the functional results and complications associated with the use of PFN and PFNA in the treatment of unstable intertrochanteric fractures, as well as to evaluate their comparative performance in the setting of osteoporosis.
Material and Methods
The study was an eighteen-month prospective comparative study undertaken at the Department of Orthopaedics, Government Medical College, Amritsar, Punjab, India, from December 1, 2020 to December 25, 2022. The study was approved by the Institutional Ethics Committee. After applying the exclusion criteria, all skeletally mature patients with unstable intertrochanteric AO 31.A2 and 31.A3 fractures who presented to the institution during this time period were included in this study. Those with stable 31.A1 intertrochanteric fractures, those who were immobile or bedridden prior to accident, and those who had previous implants in the broken hip or femur were also excluded.
The study comprised 48 patients with unstable intertrochanteric fractures who were treated with PFN or PFNA and were monitored for at least nine months. After obtaining radiographs - an anteroposterior view of the pelvis with both hips and a lateral view of the afflicted hip - the A.O. alphanumeric classification [8] was used to diagnose the fractures. Singh's index [9] was used to assess the degree of osteoporosis in the radiographs. Preoperative and postoperative hemoglobin levels, as well as blood transfusion units, were measured. The anesthetic record sheet was used to record the surgical time.The antero-posterior neck-shaft angle of the operated hip was compared to that of the normal hip to measure reduction quality. A 'excellent' reduction was defined as a deviation of fewer than 5 degrees from the normal side.Between 5 and 10 degrees of variation was considered ‘acceptable’ and more than 10 degrees variation was considered ‘poor’ [10].
The tip-apex distance reported by Baumgaertner MR [11] and the Cleveland index [12] were used to measure fixation quality. A tip-to-apex distance of 25 mm protects the screw from cutting out of the femoral head and was deemed adequate for both types of implants. On the immediate postoperative radiographs, the tip apex distance was measured using the Picture Archiving and Communication System (PACS) tool. The Cleveland index [12] was used to evaluate the compression screw position in PFN and the helical blade position in PFNA. A compression screw or helical blade centered or inferiorly centered was deemed optimum.
The Parker and Palmer mobility score [13] was used to assess functional results. As a measure of mobility return, the pre-injury mobility score was recorded and compared to the score at the final follow up. At the last follow-up, the Harris Hip score [14] was generated to assess hip function following surgery. Deep infection, acetabular penetration, blade/screw migration, nail breakage, non-union, rotation failure, or screw/blade loosening were all documented for both groups of patients during the follow-up period. Complications in both groups of patients with Singh's grade 3 were also compared.
Statistical Analysis
The unpaired t-test/Mann-Whitney test was used to compare quantitative variables, and the Chi-square test/Fisher's exact test was used to correlate qualitative variables. A p-value less than 0.05 was regarded as significant. The data was entered into an MS Excel spreadsheet before being statistically analysed with the Statistical Package for Social Sciences (SPSS) version 16.0.
Results
PFN was used on 23 of the 48 patients with AO type 31.A2 and 31.A3 fractures, while PFNA was used on the other 25. The PFN group had an average age of 60.78 years (30-90 years), while the PFNA group had an average age of 74.12 years (37-96 years). The age distribution of the two groups differed significantly (p=0.05), with the PFNA group being older. [Table/Figure 1] displays demographic statistics.
Table/ Figure 1: Demographic data and patient distribution of the two groups.
Degree of Osteoporosis
The Singh's index could not be calculated for two patients in the PFN group and one in the PFNA group due to previous implants in the opposite hip. A Singh's index of 3 or below indicated severe osteoporosis in 8 of 21 patients (38.09%) in the PFN group and 13 of 24 patients (54.16%) in the PFNA group. The distribution of osteoporotic individuals in the two groups did not differ substantially (p = 0.15). However, the PFNA group had a higher proportion of patients with radiological osteoporosis, which coincided with the average age of the two groups, with the PFN group being more than ten years younger.
A detailed description of the results has been summarized in [Table/Figure 2]
Table/Figure 2: Comparison of PFN and PFNA groups in terms of quality of fixation, functional outcomes and complications.
The average decline in haemoglobin after surgery was comparable between the two groups (p=0.61). The PFNA group's operating time was determined to be 40 minutes shorter; however, this metric was not based solely on procedural time, but also on anaesthetic record sheets.
Comparison of reduction and Fixation
Quality of Reduction:
Reduction could not be accurately assessed in two PFN patients and one PFNA patient (due to previous implants in the opposite hip, which prevented examination of neck shaft angle). 71% (15/21) of patients in the PFN group and 83% (20/24) of patients in the PFNA group achieved a good decrease [Table 3]. Only one patient (from the PFNA group) had a poor decrease according to our criteria, but no complications occurred. Implant failure occurred in four cases with high reduction, three of which were in the PFN group.
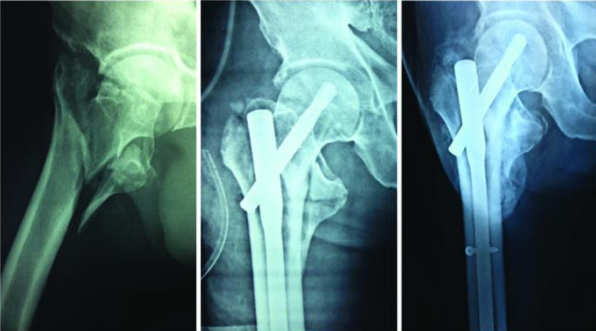
Table/Figure 3: - A 31.A3 fracture treated with PFN, with good union at one year follow up.
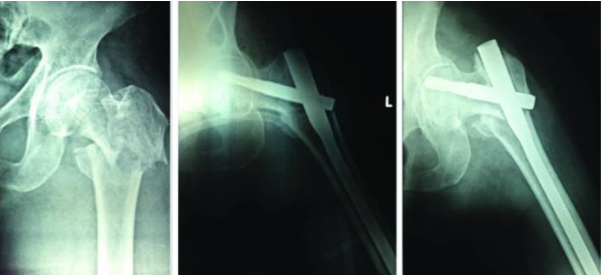
Table/Figure 4: A 31.A2 fracture treated with PFNA with good union at eight months follow up.
Tip-apex Distance: Both groups' average Tip Apex Distance (TAD) was substantially below the indicated safe range of 25 mm. The PFN group measured 19.08 mm (range 8.42-27.37 mm) and the PFNA group measured 21.13 mm (range 11.08-36.1 mm). The average TAD for cases of implant failure in the PFN group was 22.21 mm, but the TAD for the one patient with PFNA implant failure was 32.32 mm. There was no implant failure in seven other cases of TAD > 25 mm treated with the PFNA.
Implant Position as per Cleveland Index: In the PFN group, 19 of 23 patients (83%) had an optimal implant location in the femoral head, whereas in the PFNA group, 17 of 25 patients (68%) had an optimal implant position in the femoral head, i.e., either centre-centre or inferior-centre. Only two PFN failures had a suboptimal implant position, while the lone PFNA failure had a suboptimal position (superior-centre).
Comparison of Functional Outcomes
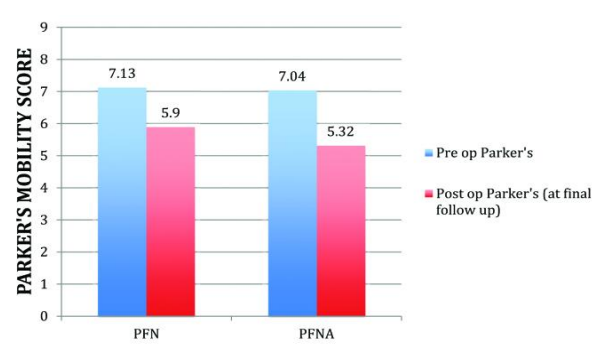
Parker’s Mobility Score and Return of Mobility [Table/Fig-5]: The average postoperative Parker's mobility score at final follow-up was identical in both patient groups (5.9 for PFN vs 5.32 for PFNA), and the difference was not statistically significant. A similar percentage of patients in both groups were able to return to their pre-injury Parker's score - 8/23 (35%) in the PFN group and 8/25 (32%).
Table/Figure 5- The preoperative and postoperative Parker’s mobility score at final follow up.
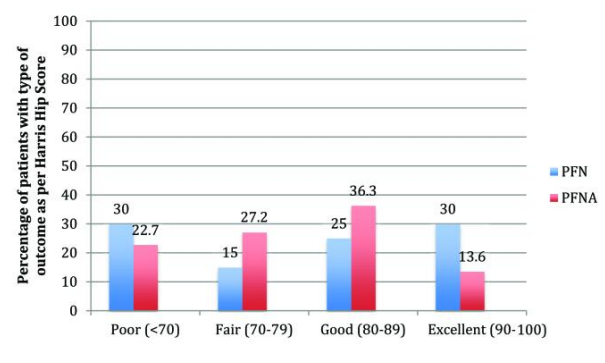
Harris Hip Score [ Table/Figure 6]: The average Harris Hip Score achieved at final follow-up was 75.37 for the PFN group and 78.85 for the PFNA group. In the PFN group, the average Harris Hip Score for implant failure cases was 41.3. The example of medial migration with the PFNA helical blade demonstrated radiological varus collapse but maintained good hip function with an 86 score.
Table/Figure 6: A comparison of Harris hip scores obtained at final follow up with the two implants
Comparison of Complications [Table/Fig-7]: Seven patients (30.4%) in the PFN group had an implant-related problem, whereas only one patient (4%) in the PFNA group had one [Table/Fig-8]. The difference in the rates of implant-related complications was found to be statistically significant (p=0.02). Both groups had one episode of deep infection, which was not deemed an implant-related consequence. One helical blade patient died from an unrelated medical cause.
Table/Fig-7: The number and type of implant related complications encountered with both devices.
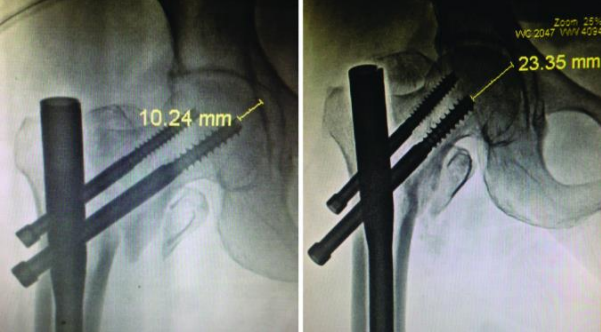
Table/Figure 8: A 31.A3 fracture treated with a helical blade showing varus collapse of the fracture and medial migration of the blade at six weeks.
Complications in patients with Singh’s index ≤ 3: Three of the eight patients with considerable osteoporosis in the PFN group had implant failure, whereas none of the 13 patients with significant osteoporosis in the PFNA group had implant failure. This difference in complication rates was found to be significant (p=0.04) in the context of osteoporosis. Implant fracture, screw back out [Table/Fig-9], and Z effect were the problems encountered in these osteoporotic instances. The TAD and implant site were both optimal in the first two cases, and the Singh's grade was 3. The TAD for the Z-effect was 26.47 mm, and the Singh's grade was 2. Four patients with Singh's grade 3 had TAD > 25 mm in the PFNA group, but none of them suffered blade migration or failure.
Table/Figure 9: A case of back-out of the compression screw of a dual screw design over six weeks after initial fixation.
Discussion
The management of unstable intertrochanteric fractures remains a problem for orthopaedic surgeons, which is exacerbated by the effect of osteoporosis on the outcome of these injuries [15]. Osteoporosis has been shown in biomechanical investigations to be a major predictor of screw migration in the proximal femur, leading to implant failure [16]. Clinical studies have also demonstrated that osteoporosis is related with poor intertrochanteric fracture outcomes [17]. As a result, several treatments, such as cement augmentation [18] and advances in implant design, are being used to try to improve fixation in osteoporotic intertrochanteric fractures. The variety of nail shapes available today reflects the ongoing search for an optimal implant for these osteoporotic fractures.
A helical blade device was a crucial advance in enhancing fixation in these fractures. The motivation behind the helical blade innovation was its biomechanical advantage in the setting of osteoporosis [6]. Without reaming, the blade can be inserted, maintaining critical bone stock in the femoral head. It compacts cancellous bone surrounding it after insertion, providing a greater purchase and enhanced resistance to varus collapse and rotational stress [19]. The current study shows that, as compared to standard PFN, this resulted in less problems in a clinical context in an osteoporotic patient group.
The use of PFNA in older patients was frequently recommended in the current investigation, owing to its theoretical advantage of improved purchase in osteoporotic bone. This is why the PFNA group was substantially older than the PFN group, although being comparable on other criteria. Our findings demonstrate no statistically significant differences in functional outcomes between the two implants, as measured by the Harris Hip Score and Parker's mobility score, but a much decreased total complication rate.
Our findings are similar with those of other research that have compared these implant designs. Mora A et al. compared the PFNA (helical blade) to the PFN and discovered that the PFNA had a lower rate of cut-out [20]. Choo SK et al. discovered reduced postoperative sliding of the PFNA compared to the PFN, but no difference in the walking abilities of patients with either implant [21]. In contrast, Park JH et al. discovered that helical blade nails dramatically improved social function, mobility, and complication rates [22]. Gardenbroek et al. discovered that the risk of a secondary late complication and re-surgery is substantially higher with a PFN than with a helical blade device in their study [23].
Other reported advantages of the helical blade device over a two-screw design include ease of insertion, shorter operative time [24-26], and less fluoroscopic exposure [25,26]. We discovered that when a helical blade was employed, the average time of surgery (from the start of anaesthesia induction to the conclusion of anaesthetic monitoring) was 40 minutes shorter. Because our measurement was not only of procedural time, this is only a preliminary estimate. We found no significant difference in blood loss or the requirement for transfusion following surgery with either implant, but this benefit has been highlighted in the literature [24]. Stern R et al. investigated whether using a single helical blade enhances device location in the femoral head and discovered no difference in implant positioning between nails using blades and screws [27]. In our study, the number of patients with appropriate implant site was lower in the helical blade group (17 of 25 versus 19 of 23 in the PFN group), corroborating their findings.
In the literature, however, there is scant reporting of clinical investigations comparing the helical blade to other cephalo-medullary nails in the setting of osteoporosis. In the current study, implant failure occurred in three of eight instances with evident osteoporosis in the PFN group but not in any of the 13 patients in the PFNA group, demonstrating that the helical blade performs better in osteoporotic bone. Osteoporosis is known to predispose to implant failure in intertrochanteric fractures, especially if the device is misplaced [28].
In the current investigation, despite a TAD of more than 25 mm, the helical blade held in four cases of grade 3 osteoporosis. This may be due to the benefits of the helical blade in terms of preserving critical bone stock and compacting the available bone stock surrounding it during insertion. Siwach RC et al. employed a helical blade extramedullary device in 51 patients with a Singh's score of 3 or less and reported a 4% complication rate, which is comparable to our PFNA results [29]. However, the Singh's index is, at best, a subjective indicator of osteoporosis [30], and this must be considered when taking conclusions from our findings and those of others who use this index to evaluate osteoporosis.
Conclusion
To summarize, we conclude that after fracture union occurs, functional outcomes are identical regardless of implant type. However, the number of implant-related issues is lower when a helical blade device is employed, showing that it is biomechanically superior than a dual screw design. In the setting of osteoporosis, PFNA outperforms PFN, which is due to helical blade compaction of cancellous bone. However, it should be noted that no implant design can compensate for poor reduction or implant placement in these fractures.
Reference
1. Babhulkar S. Management of trochanteric fractures. Indian J Orthop. 2006;40(4):210–18.
2. Zhang K, Zhang S, Yang J, Dong W, Wang S, Cheng Y, et al. Proximal femoral nail vs. dynamic hip screw in treatment of intertrochanteric fractures: a meta-analysis. Med Sci Monit. 2014;20:1628–33.
3. Kulkarni GS, Limaye R, Kulkarni M, Kulkarni S. Intertrochanteric fractures. Indian J Orthop. 2006;40:16–23.
4. Hohendorff B, Meyer P, Menezes D, Meier L, Elke R. [Treatment results and complications after PFN osteosynthesis] Unfallchirurg. 2005;108(11):938. 940, 941-46 passim.
5. Raviraj A, Anand A, Chakravarthy M, Pai S. Proximal femoral nail antirotation (PFNA) for treatment of osteoporotic proximal femoral fractures. Eur J Orthop Surg Traumatol. 2012;22:301–05.
6. Strauss E, Frank J, lee J, Kummer FJ, Tejwani N. Helical blade versus sliding hip screw for treatment of unstable intertrochanteric hip fractures. Biomech Eval Injury. 2006;37:984–89.
7. Nikoloski AN, Osbrough AL, Yates PJ. Should the tip-apex distance (TAD) rule be modified for the proximal femoral nail antirotation (PFNA)?A retrospective study. J Orthop Surg Res. 2013;8:35.
8. Marsh JL, Slongo TF, Agel J, Broderick JS, Creevey W, DeCoster TA, et al. Fracture and dislocation classification compendium - 2007:Orthopaedic Trauma Association classification, database and outcomes committee. J Orthop Trauma. 2007;21(10 Suppl):S01–133.
9. Singh M, Nagrath AR, Maini PS. Changes in trabecular pattern in the upper end of the femur as an index of osteoporosis. J Bone Joint Surg Am. 1970;52(1):457–67.
10. Karapinar L, Kumbaraci M, Kaya A, Imerci A, Incesu M. Proximal femoral nail antirotation (PFNA) to treat peritrochanteric fractures in elderly patients. Eur J Orthop Surg Traumatol. 2012;22:237–43.
11. Baumgaertner MR, Curtin SL, Lindskog DM, Keggi JM. The value of the tip-apex distance in predicting failure of fixation of peritrochanteric fractures of the hip. J Bone Joint Surg Am. 1995;77:1058–64.
12. Cleveland M, Bosworth DM, Thompson FR, Wilson HJ Jr, Ishizuka T. A ten-year analysis of intertrochanteric fractures of the femur. J Bone Joint Surg Am. 1959;41(A):1399–408.
13. Parker M, Palmer C. A new mobility score for predicting mortality after hip fracture. J Bone Joint Surg Br. 1993;75:797–98.
14. Harris WH. Traumatic arthritis of the hip after dislocation and acetabular fractures: treatment by mold arthroplasty. An end-result study using a new method of result evaluation. J Bone Joint Surg Am. 1969;51(4):737–55.
15. Broderick JM, Bruce-Brand R, Stanley E, Mulhall KJ. Osteoporotic hip fractures: the burden of fixation failure. Scientific World J. 2013;2013:515197.
16. Cheema G, Rastogi A, Singh V, Goel S. Comparison of cut out resistance of dynamic condylar screw and proximal femoral nail in reverse oblique trochanteric fractures:-a biomechanical study. Indian J Orthop. 2012;46(3):259–65.
17. Akan K, Cift H, Ozkan K, Eceviz E, Tasyikan L, Eren A. Effect of osteoporosis on clinical outcomes in intertrochanteric hip fractures treated with a proximal femoral nail. J Int Med Res. 2011;39(3):857–65.
18. Gupta RK, Gupta V, Gupta N. Outcomes of osteoporotic trochanteric fractures treated with cement-augmented dynamic hip screw. Indian J Orthop. 2012;46(6):640–45.
19. Gavaskar A, Subramanian M, Tummala N. Results of proximal femoral nail antirotation for low velocity trochanteric fractures in the elderly. Indian J Orthop. 2012;46(5):556, 60.
20. Mora A, Marimon I, Rius M, Brill W, Corral A, Gaya S. PFN versus PFNA in treatment of trochanteric femoral fractures: A prospective study. Bone and Joint Journal Orthopaedic proceedings. 2011;93(2):136.
21. Choo SK, Oh HK, Choi JY. PFNA and PFN in intertrochanteric fractures - comparison study of sliding. J Korean Hip Soc. 2010 Mar;22(1):79–85.
22. Park JH, Lee YS, Park JW, Wang JH, Kim JG. A comparative study of screw and helical proximal femoral nails for the treatment of intertrochanteric fractures. Orthopaedics. 2010;33(2):81–85.
23. Gardenbroek T, Segers M, Simmermacher R, Hammacher E. The proximal femoral nail antirotation: an identifiable improvement in the treatment of unstable pertrochanteric fractures? J Trauma. 2011;71(1):169–74.
24. D’Arrigo C, Carcangiu A, Perugia D, Scapellato S, Alonzo R, Frontini S, et al. Intertrochanteric fractures: Comparison between two different locking nails. Int Orthop. 2012;36:2545–51.
25. Xu Y, Geng D, Yang H, Wang X, Zhu G. Treatment of unstable proximal femoral fractures: comparison of the proximal femoral nail antirotation and gamma nail 3. Orthopedics. 2010;33(7):473.
26. Garg B, Marimuthu K, Kumar V, Malhotra R, Kotwal PP. Outcome of short proximal femoral nail antirotation and dynamic hip screw for fixation of unstable trochanteric fractures. A randomised prospective comparative trial. Hip Int. 2011;21:536.
27. Stern R, Lubbeke A, Suva D, Miozzari H, Hoffmeyer P. Prospective randomized study comparing screw versus helical in the treatment of low energy trochanteric fractures. Int Orthop. 2011;35:1855–61.
28. Barrios C, Brostrom LA, Stark A, Walheim G. Healing complications after internal fixation of trochanteric hip fractures: the prognostic value of osteoporosis. J Orthop Trauma. 1993;7:438–42.
29. Siwach RC, Rohilla R, Singh R, Gogna P. Radiological and functional outcome in unstable, osteoporotic trochanteric fractures stabilized with dynamic helical hip system. Strat Traum Limb Recon. 2013;8:117–22.
30. Koot VC, Kesselaer SM, Clevers GJ, Hooge P, Weits T, Werken C. Evaluation of the Singh index for measuring osteoporsis. J Bone Joint Surg Br. 1996;78(5):831.