A Deadly Connection: Recognizing and Preventing Tracheo-Brachiocephalic Artery Fistula
A Deadly Connection: Recognizing and Preventing Tracheo-Brachiocephalic Artery Fistula
Dr. Sayed Said Rabie Mohamed1*, Dr. Syed Tayyab Hussain1, Dr. Raya Sakhar Alsayyid2, Dr. Abdelgalil Ali Abdelgalil Othman Ragab1, Dr. Mouhannad Mahmoud Abdulber Fakoury1.
1. Otolaryngology Head & Neck Surgery Department, Dubai Hospital, Dubai Health, Dubai, UAE.
2. Nad Alsheba Primary Health Center, Dubai Health, Dubai, UAE.
*Correspondence to: Dr. Sayed Said Rabie Mohamed, Specialist Registrar, Otolaryngology Head & Neck surgeon.
Copyright
© 2025 Dr. Sayed Said Rabie Mohamed. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 21 March 2025
Published: 26 March 2025
DOI: https://doi.org/10.5281/zenodo.15117726
ABSTRACT:
Tracheo-Brachiocephalic Artery Fistula is a rare but fatal complication of tracheostomy, with a very high mortality rate. In this paper, we present a case that was diagnosed early and successfully treated with optimal surgical intervention.
The patient was a 57-year-old male admitted to the hospital under the care of the neurosurgery team for urgent, life-saving surgery—an evacuation of a left chronic and subacute subdural hematoma. He was intubated in the emergency room upon admission and subsequently transferred to the operating theater for surgery. Later, a tracheostomy was performed due to the need for prolonged intubation.
Three months after the tracheostomy, the patient developed massive bleeding from the tracheostomy site. An otolaryngologist was consulted and ordered an emergency CT carotid angiography with IV contrast, which revealed an abnormal fistulous communication between the brachiocephalic artery and the upper anterior tracheal wall, approximately 3 cm below the cricoid cartilage. The fistula measured about 5 mm in length.
The otolaryngologist advised increasing the tracheostomy tube cuff pressure to 50 mmHg and urgently consulted vascular surgery, interventional radiology, and the cardiothoracic surgery team for appropriate intervention to control the bleeding. The vascular surgery team reported that they could not control the bleeding, as the fistula was located in the chest rather than the neck, necessitating an emergency intervention either by an interventional radiologist for stent placement or a cardiothoracic surgeon for surgical closure.
The interventional radiologist assessed the patient and concluded that the tracheostomy site was infected, significantly increasing the risk of stent infection; therefore, stent placement was not recommended. The cardiothoracic surgery team then evaluated the patient, immediately transferred him to the operating theater, and successfully closed the fistula, controlling the massive bleeding under general anesthesia.
This case highlights the critical importance of rapid multidisciplinary collaboration and prompt intervention in the successful management of tracheo-brachiocephalic artery fistula.
Key Words: Tracheo-Brachiocephalic Artery Fistula, tracheostomy, complications, tracheo-innominate artery fistula, diagnosis, surgery, fistula, hemorrhage, TIF.
A Deadly Connection: Recognizing and Preventing Tracheo-Brachiocephalic Artery Fistula
Introduction
Tracheo-Brachiocephalic Artery Fistula, also known as Tracheo-Innominate Artery Fistula (TIF), is a life- threatening complication of both open surgical tracheostomy and percutaneous dilatational tracheostomy (McCormick and Manara, 2005). Its incidence varies from 0.3% to 0.79% (Iodice et al., 2007). Patients with TIF are at risk of sudden massive tracheal hemorrhage and asphyxiation due to blood aspiration. The survival rate is only 7.3% (Jones et al., 1976), and emergency surgery is often the only chance for survival. The etiology of this complication includes pressure necrosis from high cuff pressure, mucosal trauma from a malpositioned cannula tip, a low tracheal incision, excessive neck movement, radiotherapy, and prolonged intubation, all of which have been implicated in TIF formation. The use of a high-volume, low-pressure cuff may reduce the risk of subsequent fistula formation.
In terms of management, median sternotomy for ligation of the artery remains the most common approach for TIF repair. However, even after successful surgical intervention, postoperative local or mediastinal infections can lead to recurrent bleeding, which is often fatal and distressing for both healthcare providers and the patient’s family (Praveen et al., 2007). Preventing rebleeding is crucial for the successful management of TIF.
Without surgical intervention, the mortality rate approaches 100% due to acute massive tracheal hemorrhage (Tomoyasu et al., 2007). The median sternotomy provides excellent exposure and can be performed rapidly, while a cuffed endotracheal or tracheostomy tube helps tamponade the bleeding site. Before addressing the injured area, proximal and distal control of the innominate artery must be established. Various surgical techniques have been reported, including direct suture, resection, and ligation of the innominate artery.
Although a few cases of TIF have been successfully treated with graft interposition (Jamal-Eddine et al., 2008), endovascular stent grafting (Cohen et al., 2008), or endovascular embolization (Takasaki et al., 2005), fatalities have been reported due to rebleeding when attempts were made to preserve innominate artery flow using direct sutures or prosthetic materials in an infected area (Gelman et al., 1994).
Ligation of the innominate artery is considered the first-line treatment, as previous studies have shown that interruption of its flow does not result in significant neurological or vascular complications due to collateral circulation via the external carotid artery, thyrocervical trunk, and vertebral vessels (Allan and Wright, 2003; Gelman et al., 1994; Silen and Spieker, 1965). Various surgical techniques have been employed for tracheal repair, including primary closure to allow for natural granulation, patch closure with heterologous tissue, and patch closure with autologous tissue (Tomoyasu et al., 2007). To protect the blood vessel, it should be covered with viable adjacent tissue, such as the sternocleidomastoid or strap muscles. Some authors have also recommended using an autologous pericardium flap (Hsiao et al., 2012) or a pectoralis major myocutaneous flap (Roh et al., 2006). Suction drains should be placed in the mediastinum, as rebleeding can occur due to mediastinal infection caused by residual necrotic tissue and granulation.
Preventing this complication should be a priority in all tracheostomy procedures, as treatment is extremely challenging once TIF occurs. Tracheostomy indications should be carefully evaluated to avoid unnecessary procedures, and whenever possible, it should be performed in an optimal surgical environment, such as the operating room. The incision should be made at the second or third tracheal ring, avoiding prolonged or excessive neck hyperextension. Anatomic variations, such as an aberrant high-riding innominate artery, should be considered during the procedure. For patients undergoing percutaneous tracheostomy in the intensive care unit, bedside ultrasound screening can help identify pretracheal vascular structures, thereby minimizing the risk of hemorrhage. If a cuffed tracheostomy tube is used, the cuff pressure should be maintained below 20 mmHg (Hsiao et al., 2012) to prevent excessive pressure on the tracheal mucosa.
Case Report
A 57-year-old male patient was admitted to the hospital under the care of the neurosurgery team for an urgent life-saving surgery, which was performed for the evacuation of a left chronic and subacute subdural hematoma. The patient was intubated in the Emergency Room and received ventilator support. His past medical history included a previous cerebrovascular accident (CVA), type 2 diabetes mellitus without complications, and hyperlipidemia.
During his hospital stay, he developed nosocomial pneumonia, septic shock, and respiratory failure. Due to prolonged intubation, the patient underwent a tracheostomy.
Three months later, oozing from the tracheostomy stoma was noted five days after a routine tracheostomy tube change. The bleeding progressed dramatically, leading to massive hemorrhage from the tracheostomy site and throat, which was associated with hypotension and a drop in hemoglobin (Hb) from 8.6 g/dL to 6 g/dL. Emergency Management;
• Intravenous fluids were administered.
• Femoral central line and brachial artery line were inserted.
• Two units of packed red blood cells (RBCs) were transfused.
• An urgent ENT consultation was requested.
Upon ENT evaluation, clots were removed from around the tracheostomy tube, and no active bleeding was noted at that time. A throat pack was applied, and an emergency CT carotid angiogram was recommended to rule out Tracheo-Brachiocephalic Artery Fistula (TIF).
Fig 1
Fig 2
Fig 3
Imaging Findings
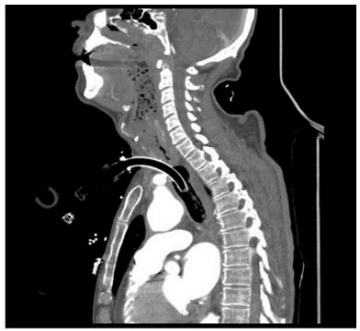
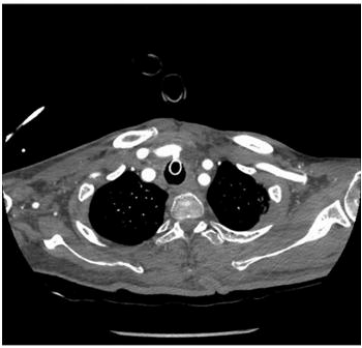
Emergency multiphasic CT carotid angiography using IV contrast was performed, including axial thin cuts with multiplanar and maximum intensity projection (MIP) reformatted images.
The study revealed:
• Abnormal fistulous communication between the brachiocephalic artery and the upper anterior tracheal wall, approximately 3 cm below the cricoid cartilage.
• The fistula measured approximately 5 mm in length.
• Dense secretions were noted in the trachea and main bronchi.
• Diffuse marked atherosclerotic changes were observed in the visualized portion of the thoracic aorta, characterized by mural irregularities, thickening, and intimal calcifications.
• Mild atherosclerotic changes were noted in the bilateral common carotid arteries and the extracranial segments of the internal carotid arteries, with no evidence of significant stenosis.
Multidisciplinary Management
The ENT surgeon reviewed the CT angiogram and recommended:
• Increasing the tracheostomy tube cuff pressure to 50 mmHg.
• Considering an urgent change from a tracheostomy tube to an endotracheal tube in case of airway collapse or severe uncontrolled bleeding.
• Requesting urgent consultations from the vascular surgery, interventional radiology, and cardiothoracic surgery teams for definitive management.
Specialist Evaluations
• The vascular surgery team reviewed the patient and confirmed the diagnosis of Tracheo- Brachiocephalic Artery Fistula, stating that emergency intervention was required. They suggested possible endovascular stenting by interventional radiology or surgical repair by cardiothoracic surgery, as the fistula was located in the chest rather than the neck.
• The interventional radiology team assessed the patient but advised against stenting, as the tracheostoma was infected, increasing the risk of stent infection.
• The cardiothoracic surgery team decided to proceed with immediate surgical intervention in the operating theater to close the fistula and control the massive bleeding under general anesthesia.
Surgical Procedure
In the operating theater, the following steps were performed:
1. Median sternotomy incision was made.
2. Dissection of the ascending aorta and arch vessels was carried out.
3. Right brachiocephalic trunk was identified and controlled using a vessel loop.
4. Dissection of the right subclavian artery was performed.
5. Clamping of the brachiocephalic trunk and right subclavian artery was achieved.
6. Dissection of the fistulous tract between the brachiocephalic artery at its bifurcation and the anterior tracheal wall was performed.
7. The fistula was closed using 4/0 Prolene continuous sutures.
8. Meticulous hemostasis was ensured.
9. The sternotomy wound was closed in layers, and two chest drains were placed: one retrosternal and one in the left pleural cavity.
The patient tolerated the procedure well and was transferred to the Surgical Intensive Care Unit (SICU) for postoperative management.
Postoperative Course
The patient remained in the SICU for three weeks following surgery without any complications and continued to receive medical management.
Discussion and Conclusion
Tracheo-Brachiocephalic Artery Fistula (TIF) is a rare but fatal complication of tracheostomy, with a high mortality rate if not diagnosed and treated promptly. In this report, we present a case that was diagnosed early and successfully managed with optimal surgical intervention.
The successful outcome in this case highlights the critical importance of early recognition, rapid intervention, and a multidisciplinary approach. Effective management requires full cooperation and immediate response from all involved teams, including:
• Intensive Care Unit (ICU) team
• Otolaryngology team
• Radiology team
• Cardiothoracic surgery team
• Vascular surgery team
• Interventional radiology team
A high index of suspicion is essential in patients with sudden, unexplained bleeding from a tracheostomy site, and urgent imaging should be performed to confirm the diagnosis. In this case, early ENT consultation, rapid imaging, and coordinated surgical intervention led to a successful outcome, demonstrating the importance of timely and collaborative management in life-threatening complications of tracheostomy.
References
1. Allan JS, Wright CD. 2003. Tracheoinnominate fistula: diagnosis and management. Chest Surg Clin N Am., 13:331–341.
2. Cohen JE, Klimov A, Rajz G, Paldor I, Spektor S. 2008. Exsanguinating tracheoinnominate artery fistula repaired with endovascular stent-graft. Surg Neurol., 69:306–309.
3. Flint AC, Midde R, Rao VA, Lasman TE, Ho PT. 2009. Bedside ultrasound screening for pretracheal vascular structures may minimize the risks of percutaneous dilatational tracheostomy. Neurocrit Care, 11:372–376.
4. Gelman JJ, Aro M, Weiss SM. 1994. Tracheo-innominate artery fistula. J Am Coll Surg., 179:626–634.
5. Hsiao CW, Lee SC, Lee KC, Cheng YL, Tzao C. 2002. Tracheoinnominate artery fistula: successful surgical management of one case. Thorac Cardiovasc Surg., 50:249–250.
6. Iodice F, Brancaccio G, Lauri A, Di Donato R. 2007. Preventive ligation of the innominate artery in patients with neuromuscular disorders. Eur J Cardiothorac Surg., 31:747–749.
7. Jamal–Eddine H, Ayed AK, Al–Moosa A, Al–Sarraf N. 2008. Graft repair of tracheo-innominate artery fistula following percutaneous tracheostomy. Interact Cardiovasc Thorac Surg., 7:654–655.
8. Jones JW, Reynolds M, Hewitt RL, Drapanas T. 1976. Tracheo-innominate artery erosion: successful surgical management of a devastating complication. Ann Surg., 184:194–204.
9. McCormick B, Manara AR. 2005. Mortality from percutaneous dilatational tracheostomy. A report of three cases. Anaesthesia, 60:490–495.
10. Praveen CV, Martin A. 2007. A rare case of fatal haemorrhage after tracheostomy. Ann R Coll Surg Engl., 89:W6–8.
11. Roh JL, Na MH, Kim KH. 2006. Treating tracheo-innominate artery fistula with interposition of a pectoralis major myocutaneous flap. Eur Arch Otorhinolaryngol., 263:180–182.
12. Silen W, Spieker D. 1965. Fatal hemorrhage from the innominate artery after tracheostomy. Ann Surg., 162:1005–1012.
13. Takasaki K, Enatsu K, Nakayama M, Uchida T, Takahashi H. 2005. A case with tracheo-innominate artery fistula. Successful management of endovascular embolization of innominate artery. Auris Nasus Larynx., 32:195–198.
14. Tomoyasu M, Tanita T, Nakajima T, et al. 2007. Successful repair using innominate vein flap, pericardial flap and thymus pedicle flap for tracheo-innominate artery fistula. Ann Thorac Cardiovasc Surg., 13:143–146.