Diagnosis of Heart Failure with Preserved Ejection Fraction by Machine Learning.
Diagnosis of Heart Failure with Preserved Ejection Fraction by Machine Learning.
Dr Aruna kurukundu1*, Dr Amit Munjal 2, Dr Prachi Arun 3, Dr Palvi Mahajan 4
1 Dr Aruna kurukundu, Cardiologist, KIMS, Kurnool(AP).
2 Dr Amit Munjal, Cardiologist, Munjal Multispeciality Hospital, Fatehabad, Haryana.
3. Dr Prachi Arun, Associate professor, Dept of pathology, MAMC, AGROHA (Haryana).
4. Dr Palvi Mahajan, BMC superspeciality Hospital, Barnala, punjab, India.
*Correspondence to: Dr Aruna kurukundu, Dr Aruna kurukundu, Cardiologist, KIMS, Kurnool(AP), India.
Copyright.
© 2025 Dr Aruna kurukundu This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 26 Mar 2025
Published: 03 Apr 2025
Diagnosis of Heart Failure with Preserved Ejection Fraction by Machine Learning.
Introduction
Heart failure (HF) is a significant public health issue globally, affecting approximately 1-3% of the Indian population [1]. Approximately half of all patients with heart failure have heart failure with preserved ejection fraction [2]. Heart failure with preserved ejection fraction (HFpEF) is a complex clinical syndrome identified by the presence of signs and symptoms of HF despite having a near-normal LV ejection fraction (LVEF; ≥50%) [3]. The clinical symptoms of HFpEF arise from intricate changes in the structure and function of cardiomyocytes, leading to hemodynamic disturbances [2].
An accurate diagnosis of HFpEF is difficult since it frequently manifests with nonspecific symptoms that can easily be mistaken for other conditions [4]. Echocardiography (echo), the most frequently employed diagnostic tool, has limitations when used solely to depend on left ventricular ejection fraction (LVEF) as an indicator of cardiac function. This measurement primarily assesses systolic function and may not adequately capture the complete range of myocardial dysfunction in HFpEF patients, particularly those experiencing both systolic and diastolic dysfunction [5, 6].
Machine learning (ML) is a discipline that originated from statistics and computer science, focusing on the capacity of computers to learn from data, comprehend it, and make predictions. One of the main challenges in the clinical environment is the difficulty of interpreting the vast amount of data from various sources. This is where ML could be particularly beneficial for clinicians and researchers, as it can help prevent the loss of potentially valuable information that could enhance clinical decision-making and patient care [7, 8]. Heart failure with preserved ejection fraction (HFpEF) exemplifies a cardiovascular condition that stands to gain from ML due to its inherent variability, the need for better classification, and the complexities involved in diagnosing and treating HFpEF [8]. The HFA-PEFF score is a diagnostic tool for identifying patients with heart failure with preserved ejection fraction (HFpEF). It combines clinical assessments, echocardiographic data, and natriuretic peptide levels to estimate the probability of HFpEF in individuals presenting with heart failure symptoms [9].
To enhance the diagnostic process, the current study focuses on evaluating the sensitivity and accuracy of machine learning (ML) models, specifically the Random Forest and CART models, compared to the HFA-PEFF scoring system. By analysing these ML approaches, the study aims to determine their effectiveness in diagnosing HFpEF relative to the established HFA-PEFF score.
Methodology
The current single-centre retrospective study was conducted among patients attending the outpatient and inpatient department of tertiary healthcare centres in India for a period of 24 months from March 2019-2021. Informed consent was obtained from all patients.
Inclusion and exclusion criteria:
- Patients with LV EF >45%
- Patients >18 yrs age
- Patients with Rheumatic heart disease
- Patients having NT Pro BNP report.
Ethical clearance:
Ethical clearance was obtained from the Institutional Ethics committee and Scientific Research Committee, Aster Prime hospital, Ameerpet, Hyderabad.
Study population:
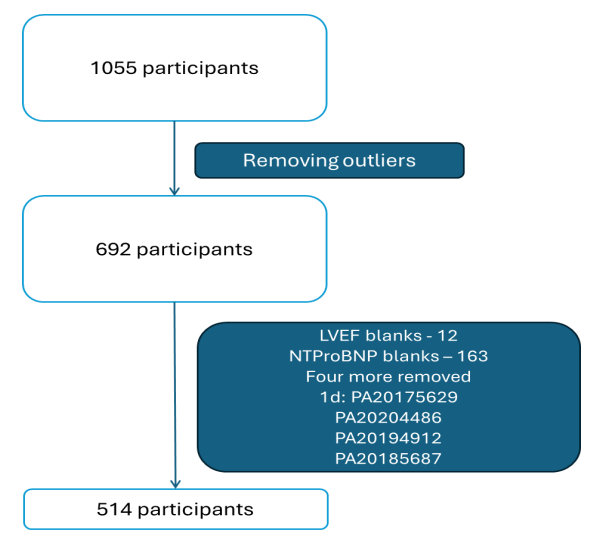
The data pertaining to 1068 consecutive patients with suspected HF were analyzed. After removal of outliers based on a box-and-whisker plot, data was selected based on LVEF values of above 45%, a sample size of 693 patients was initially considered for the study. After removing patients with missing BNP and LVEF values, a final data set of 514 patients was considered for the study. This data has been calculated as appropriate based on the prevalence of our hospital's statistical analysis over the last two years [Figure 1]. Demographic data including age and gender), vital signs (such as heart rate, systolic blood pressure and diastolic blood pressure), medical and personal history, co-morbidities, medication history, diagnostic parameters, chest radiography and focussed echocardiography evaluation to assess the presence of HFpEF was recorded. The diagnosis of HF and categorization into HFrEF and HFpEF was made by two independent physicians based on clinical, biochemical and echocardiography data.
HFpEF diagnosis: HFpEF diagnosis was based on signs or symptoms of heart failure with LVEF >45% along with structural and diastolic physiological parameters supporting the diagnosis of HFpEF that included left atrial size (left atrial volume index), left ventricular hypertrophy (Left ventricular mass index), diastolic filling, E/e’ value and global longitudinal strain (GLS) value. The level of N-terminal pro brain natriuretic peptide (NT-pro BNP) was assessed in all patients. Those patients with NT-pro BNP level less than 125 pg/ml were excluded from the study despite a clinical suspicion of HF diagnosis. Using these parameters, HFA-PEFF score was calculated for all the patients [ref].
A total of 50 attributes were recorded for each patient, with each attribute assigned an integer value of 0 or 1 to indicate its presence or absence. In the preliminary investigation, significant variables were identified through trial and error using Orange Data Mining software v3.31. Previous studies have highlighted the importance of variables such as NT-proBNP and echocardiographic measures in predicting heart failure, so these were included in our model. Additionally, we incorporated common comorbidities associated with HFpEF, such as Chronic Kidney Disease (CKD), Chronic Obstructive Pulmonary Disease (COPD), and Anemia. This resulted in a baseline set of variables that could be further refined using XLSTAT (Addinsoft 2019).
After extensive preprocessing, we ultimately selected 23 attributes for machine learning model generation. The selected attributes include:
Age
Gender
Presence of heart failure
Blood pressure
Atrial fibrillation
Diabetes mellitus
Hypertension
Coronary artery disease (CAD)
Body Mass Index (BMI)
Asthma/COPD
Estimated Glomerular Filtration Rate (eGFR)
Hemoglobin levels
NT-proBNP
Pulmonary edema
Left Atrial Volume Index (LAVI)
Left Ventricular Mass Index (LVMI)
Tricuspid Regurgitant Jet Velocity (TRJV)
Left Ventricular Ejection Fraction (LVEF)
Lateral e’
Septal e’
E/e’
Global Longitudinal Strain (GLS)
HFA-PEFF score
For this study, two ML models (Random Forest and CART models) were generated and then compared to both expert opinion and the HFA-PEFF score. For each machine learning technique, we have recursively varied internal parameters in order to obtain a good compromise between learning ability and generalization capability.
CART algorithm: It is a supervised machine learning method that can be applied to both classification and regression problems. In our study, we utilized the classification model to identify patients with and without heart failure with preserved ejection fraction (HFpEF). The decision tree structure of CART systematically splits attributes into various branches until specific end criteria are met, employing mathematical equations to guide these decisions.
Random Forest algorithm: It is also a supervised machine learning technique capable of handling both classification and regression tasks. However, it distinguishes itself by creating an ensemble of multiple decision trees rather than relying on a single tree. This ensemble approach enhances performance and robustness. By utilizing techniques such as bootstrap aggregation and feature randomness, Random Forest generates multiple trees, leading to improved diagnostic accuracy.
Training and testing of the ML program:
In the preliminary model, 75% of the dataset was used to train the model, and 25% was used to test it. So in this study we are training the model with 385 datasets and testing the remaining 129 datasets for ML diagnosis of HFpEF. We will study different ML algorithms and come to a conclusion regarding diagnosis of HFpEF by ML.
Figure 1: CONSORT Flow diagram
Statistical analysis:
All the data was entered in a Microsoft Excel sheet and analysed using Orange data mining v3.31 software. Categorical variables were expressed as N (%) and continuous variables were expressed as mean ± SD or Median [IQR]. For evaluating the applicability of ML models in diagnosing HFpEF, confusion matrix, sensitivity, specificity, accuracy, precision, recall, and F1 score were estimated. The secondary endpoints compared the accuracy of ML models with HFA-PEFF scoring system in the diagnosis of HFpEF. P<0.05 was considered to be statistically significant.
Results
The current study was conducted in 513 patients, with 186 patients (36%) diagnosed with HFpEF. Demographic and clinical characteristics of the total population is provided in table 1. Individuals diagnosed with HFpEF had an average age of 67.1 ± 11.8 years with an M:F ration of 0.898. History of T2DM and hypertension was present in 61.3% and 84.9%, respectively. History of atrial fibrillation and COPD/asthma were present in 18.3% and 12.9%, respectively. CKD was present in 17.7% and eGFR <45% was observed in 46.4%. Pulmonary edema was present in 80.6% of the population. The ECHO parameters are listed in Table 1.
Table 1: Demographics and clinical characteristics
|
|
Total population (N = 513) |
HFpEF (N = 186) |
|
Age |
64.8 ± 13.0 |
67.1 ± 11.8 |
|
Gender Male Female |
276 (53.8%) 237 (46.2%) |
88 (47.3%) 98 (52.7%) |
|
Smoking |
33 (6.4%) |
13 (7%) |
|
Alcohol consumption |
3 (0.6%) |
2 (1.1%) |
|
Heart rate |
93.8 ± 18.2 |
96.1 ± 21.4 |
|
Diabetes |
288 (56.1%) |
114 (61.3%) |
|
History of hypertension |
392 (76.4%) |
158 (84.9%) |
|
SBP |
129.1 ± 26.0 |
130.4 ± 28.5 |
|
DBP |
79.2 ± 13.7 |
79.8 ± 15.0 |
|
Uncontrolled hypertension (SBP≥140/DBP≥90) |
223 (43.5%)
|
87 (46.8%) |
|
BMI (in kg/m2) |
21.3 ± 1.7 |
21.2 ± 1.7 |
|
Overweight/ Obese status |
87 (17%) |
28 (15.1%) |
|
Hypercholesterolemia |
16 (3.1%) |
4 (2.2%) |
|
Atrial fibrillation |
44 (8.6%) |
34 (18.3%) |
|
Asthma/ COPD |
65 (12.7%) |
24 (12.9%) |
|
eGFR |
60.4 ± 39.5 |
54.3 ± 33.3 |
|
eGFR distribution ≥90 60-89 45-59 30-44 <30 |
102 (19.9%) 125 (24.4%) 62 (12.1%) 77 (15%) 128 (25%) |
24 (12.9%) 50 (26.9%) 26 (14%) 33 (17.7%) 50 (26.9%) |
|
CKD |
97 (18.9%) |
33 (17.7%) |
|
CAD |
138 (26.9%) |
49 (26.3%) |
|
Hypothyroidism |
83 (16.2%) |
31 (16.7%) |
|
Haemoglobin (%) |
11.2 ± 2.5 |
10.9 ± 2.4 |
|
Anaemia |
357 (69.6%) |
140 (75.3%) |
|
Pulmonary edema |
341 (66.5%) |
150 (80.6%) |
|
LAVI |
24.6 ± 5.0 |
25.9 ± 6.7 |
|
LVEDD |
4.7 ± 0.3 |
4.7 ± 0.4 |
|
LVESD |
3.0 ± 0.3 |
3.0 ± 0.4 |
|
LVMI |
109.7 ± 12.2 |
110.2 ± 12.7 |
|
TRJV |
2.8 ± 0.6 |
3.0 ± 0.7 |
|
TAPSE |
2.0 ± 0.8 |
1.9 ± 0.2 |
|
Lateral e’ Median [IQR] |
0.1000 [0.0900, 0.1300] |
0.1000 [0.0900, 0.1300] |
|
Septal e’ Median [IQR] |
0.0800 [0.0600, 0.0900] |
0.0700 [0.0600, 0.0900] |
|
E (m/sec) |
0.8 ± 0.6 |
0.8 ± 0.8 |
|
E/e’ |
8.5 ± 4.2 |
9.0 ± 6.4 |
|
GLS (%) |
-11.5 ± 3.2 |
-11.3 ± 3.0 |
|
NT-ProBNP Median [IQR] |
2710 [703.4, 10788] |
4282 [1466, 12576] |
In the study, it was found that 67.2% of patients with heart failure with preserved ejection fraction (HFpEF) had an HFA-PEFF score greater than 4, indicating a definitive diagnosis of HFpEF (Table 2).
The diagnostic capabilities of the CART model and the RANDOM FOREST model were evaluated. For the CART model, the confusion matrix analysis demonstrated a sensitivity of 70% and a specificity of 51.7% in diagnosing HFpEF (Table 3). On the other hand, the RANDOM FOREST model exhibited improved performance, achieving a sensitivity of 78.3% and a specificity of 68.1% for HFpEF diagnosis (Table 4).
Table 5 shows the overall diagnostic accuracy of both models. The analysis highlighted that both the CART and RANDOM FOREST models displayed higher sensitivity and specificity when it came to diagnosing HFpEF than HFA-PEFF score (Table 6).
Table 2: HFpEF diagnosis by HFA-PEFF score
|
|
Number of subjects (n = 186) |
Percentage |
|
HFpEF unlikely (<1) |
1 |
0.5% |
|
HFpEF Intermediate (2-4) |
60 |
32.3% |
|
HFpEF Definite (>4) |
125 |
67.2% |
Analysis of ML program
Table 3: Confusion matrix of CART model
|
|
ML predicted HF |
ML did not predict HF |
|
HF diagnosed |
70 (TP) |
28 (FP) |
|
HF not diagnosed |
30 (FN) |
25 (TN) |
|
Sensitivity = TP / (TP+FN) = 70/100 = 70% Specificity = TN/ (TN + FP) = 30/58 = 51.7% |
||
Table 4: Confusion matrix of RANDOM FOREST model
|
|
ML predicted HF |
ML did not predict HF |
|
HF diagnosed |
83 (TP) |
15 (FP) |
|
HF not diagnosed |
32 (FN) |
23 (TN) |
|
Sensitivity = TP / (TP+FN) = 83/106 = 78.3% Specificity = TN/ (TN + FP) = 32/47 = 68.1% |
||
Table 5: Diagnostic accuracy of both the ML models
|
|
AUC |
CA |
F1 |
Precision |
Recall |
p-value |
|
RANDOM FOREST |
0.709 |
0.707 |
0.692 |
0.698 |
0.707 |
0.00027 |
|
CART |
0.590 |
0.626 |
0.622 |
0.619 |
0.626 |
0.035 |
Table 6: Comparison of diagnostic accuracy of ML with HFA- PEFF score
|
|
Sensitivity |
Specificity |
Accuracy |
NPV |
P-value |
|
RANDOM FOREST |
0.84 |
0.41 |
0.69 |
0.60 |
0.00027 |
|
CART |
0.71 |
0.45 |
0.62 |
0.47 |
0.035 |
|
HFA-PEFF |
0.67 |
0.40 |
0.70 |
0.53 |
0.004 |
Discussion
The role of CART and RANDOM FOREST ML models were investigated in HFpEF diagnosis. The CART model demonstrated a sensitivity of 70% and a specificity of 51.7%, while the RANDOM FOREST model showed enhanced performance with a sensitivity of 78.3% and a specificity of 68.1%. Overall, both models outperformed the HFA-PEFF score in terms of sensitivity and specificity in diagnosing HFpEF.
In 2019, the Heart Failure Association (HFA) of the European Society of Cardiology (ESC) introduced the Heart Failure Association Pre-test Assessment, Echocardiography & Natriuretic Peptide, Functional Testing, Final Etiology (HFA-PEFF) algorithm for diagnosing heart failure with preserved ejection fraction (HFpEF) [10]. A meta-analysis indicated that the sensitivity and specificity of the HFA-PEFF score for confirming HFpEF were 59% and 86%, respectively [11]. However, the current study found a higher sensitivity of 69% with HFA-PEFF in diagnosing HFpEF.
As Artificial Intelligence rapidly advances in medicine, our study focused on diagnosing the complex HFpEF condition. Given that HFpEF diagnosis often requires intricate scoring systems and invasive procedures, we aimed to develop a machine learning model that enables early diagnosis by physicians, even in remote areas [12]. In this study we used the methodology of feature selection and outliers’ detection by Isolation Forest method which improved the dataset and in turn the accuracy of the ML model. In a study by Bharti et al., similar methodology was used for the prediction of heart disease by ML and deep learning techniques which helped in improving the accuracy of the ML models [5]. Dong-Ju Choi et al. demonstrated that the AI-CDSS with the CART algorithm achieved superior diagnostic accuracy (78% ) for diagnosing heart failure, surpassing the accuracy of non-HF specialists (50%) [12]. Guidi et al., utilized the CART and RANDOM FOREST model to determine the diagnosis and severity of HF. RANDOM FOREST AND CART ML models observed an accuracy of 83.3% and 81.2% respectively with RF model having comparatively better accuracy than CART [13]. Our study also observed diagnostic accuracies of 62% and 70% with CART and Random Forest, respectively, which are comparable to the HFA-PEFF score's 70%.
In a March 2021 study by Woolley et al., researchers used machine learning to subgroup HFpEF based on NT Pro BNP values, identifying four clusters: CKD/Diabetes, elderly, young and obese, and COPD. They found that the CKD/Diabetes and COPD groups had the highest adverse outcomes and NT Pro BNP levels [14]. Similarly, in our study, COPD, CKD and Diabetes was present in 13%,18% and 62% respectively. Since NT Pro BNP has limitations and can be elevated even in patients who do not have HFpEF, we did not go on this one variable only and taken other clinical and echo parameters also to predict a ML model.
In a study by Tabassian and his colleagues, machine learning models were developed for diagnosing HFpEF using velocity, strain, and strain rates from echo at rest and during exercise. They applied KNN as an unsupervised model and a supervised classifier, achieving about 80% accuracy with strain rate [15]. However, measuring strain rates in all patients during exercise is often impractical due to varying patient conditions. Therefore, we focused on more feasible variables for our study.
Hedman et al. employed unsupervised machine learning models, such as neural networks and Naïve Bayes, to classify 528 HFpEF patients into six distinct phenogroups for improved managemen [16]. In our study, we had a smaller dataset of 186 HFpEF patients, with only 8 echocardiographic features and 7 comorbidities, which limited our ability to phenotype. With a larger HFpEF dataset, we could effectively use the Random Forest model for patient grouping into phenotypes.
Choi et al. demonstrated that a hybrid approach combining machine learning (ML) techniques with clinical diagnosis significantly enhances the accuracy of diagnosing heart failure with preserved ejection fraction (HFpEF). Their findings indicated an accuracy of 55% when assessed by non-HF experts, 78.9% using ML, 82% by HF experts, and an impressive 95% with the hybrid method [12]. In our study, we also observed an accuracy of 68% with ML and 70% with HF experts. These results suggest that ML techniques can effectively assist physicians, particularly those who are not specialized in heart failure, in making early diagnoses and implementing targeted interventions for patients. Future studies in larger sample sizes can explore various subgroups or phenotypes of HFpEF in enhancing our understanding of the condition and inform more effective treatment strategies for patients affected by HFpEF.
Limitations: This study has several limitations, primarily due to the small dataset. Increasing the number of participants could enhance the accuracy of our machine learning (ML) models. With only about 34% of the population being HFpEF patients, we were unable to effectively phenotype these groups. Additionally, we relied solely on retrospective data; incorporating prospective data could improve our ML model's accuracy, as demonstrated by Dong-Ju Choi et al., who reported a 95.5% accuracy with prospective cohorts. Moreover, our study population did not include any obese patients with a BMI over 30 kg/m², limiting our ability to explore this specific HFpEF phenotype. Addressing these limitations in future research could yield more comprehensive insights into HFpEF subtypes.
Conclusion
In conclusion, our study demonstrates that machine learning models, particularly Random Forest, outperform traditional diagnostic methods for HFpEF. With an accuracy of 0.69 and sensitivity of 0.84, the Random Forest model shows significant promise compared to the HFA-PEFF score, which has an accuracy of 0.70 and sensitivity of 0.67. These findings suggest that ML models could enhance early diagnosis and management strategies for HFpEF patients.
References
1.
[1] G. Savarese, P. M. Becher, L. H. Lund, P. Seferovic, G. M. C. Rosano and A. J. S. Coats, “Global burden of heart failure: a comprehensive and updated review of epidemiology,” Cardiovascular Research, vol. 118, p. 3272–3287, February 2022.
[2] A. B. Gevaert, R. Kataria, F. Zannad, A. J. Sauer, K. Damman, K. Sharma, S. J. Shah and H. G. C. Van Spall, “Heart failure with preserved ejection fraction: recent concepts in diagnosis, mechanisms and management,” Heart, vol. 108, p. 1342–1350, January 2022.
[3] P. Garg, H. Assadi, R. Jones, W. B. Chan, P. Metherall, R. Thomas, R. van der Geest, A. J. Swift and A. Al-Mohammad, “Left ventricular fibrosis and hypertrophy are associated with mortality in heart failure with preserved ejection fraction,” Scientific Reports, vol. 11, January 2021.
[4] F. Formiga, J. Nuñez, M. J. Castillo Moraga, M. Cobo Marcos, M. I. Egocheaga, C. F. García-Prieto, A. Trueba-Sáiz, A. Matalí Gilarranz and J. M. Fernández Rodriguez, “Diagnosis of heart failure with preserved ejection fraction: a systematic narrative review of the evidence,” Heart Failure Reviews, vol. 29, p. 179–189, October 2023.
[5] H. A. H. Bshiebish, A. H. Al-Musawi and S. A. Khudeir, “Role of global longitudinal strain in assessment of left ventricular systolic function in patients with heart failure with preserved ejection fraction,” Journal of the Saudi Heart Association, vol. 31, p. 100–105, April 2019.
[6] S. Romano, I. N. Mansour, M. Kansal, H. Gheith, Z. Dowdy, C. A. Dickens, C. Buto-Colletti, J. M. Chae, H. H. Saleh and T. D. Stamos, “Left Ventricular global longitudinal strain predicts heart failure readmission in acute decompensated heart failure,” Cardiovascular Ultrasound, vol. 15, March 2017.
[7] F. S. Ahmad, Y. Luo, R. M. Wehbe, J. D. Thomas and S. J. Shah, “Advances in Machine Learning Approaches to Heart Failure with Preserved Ejection Fraction,” Heart Failure Clinics, vol. 18, p. 287–300, April 2022.
[8] S. J. Shah, “Precision Medicine for Heart Failure with Preserved Ejection Fraction: An Overview,” Journal of Cardiovascular Translational Research, vol. 10, p. 233–244, June 2017.
[9] K. Egashira, D. Sueta, T. Komorita, E. Yamamoto, H. Usuku, T. Tokitsu, K. Fujisue, T. Nishihara, F. Oike, M. Takae, S. Hanatani, S. Takashio, M. Ito, K. Yamanaga, S. Araki, H. Soejima, K. Kaikita, K. Matsushita and K. Tsujita, “HFA-PEFF scores: prognostic value in heart failure with preserved left ventricular ejection fraction,” The Korean Journal of Internal Medicine, vol. 37, p. 96–108, January 2022.
[10] B. Pieske, C. Tschöpe, R. A. de Boer, A. G. Fraser, S. D. Anker, E. Donal, F. Edelmann, M. Fu, M. Guazzi, C. S. P. Lam, P. Lancellotti, V. Melenovsky, D. A. Morris, E. Nagel, E. Pieske-Kraigher, P. Ponikowski, S. D. Solomon, R. S. Vasan, F. H. Rutten, A. A. Voors, F. Ruschitzka, W. J. Paulus, P. Seferovic and G. Filippatos, “How to diagnose heart failure with preserved ejection fraction: the HFA–PEFF diagnostic algorithm: a consensus recommendation from the Heart Failure Association (HFA) of the European Society of Cardiology (ESC),” European Heart Journal, vol. 40, p. 3297–3317, August 2019.
[11] X. Li, Y. Liang and X. Lin, “Diagnostic and prognostic value of the HFA-PEFF score for heart failure with preserved ejection fraction: a systematic review and meta-analysis,” Frontiers in Cardiovascular Medicine, vol. 11, July 2024.
[12] D.-J. Choi, J. J. Park, T. Ali and S. Lee, “Artificial intelligence for the diagnosis of heart failure,” npj Digital Medicine, vol. 3, April 2020.
[13] G. Guidi, M. C. Pettenati, P. Melillo and E. Iadanza, “A Machine Learning System to Improve Heart Failure Patient Assistance,” IEEE Journal of Biomedical and Health Informatics, vol. 18, p. 1750–1756, November 2014.
[14] R. J. Woolley, D. Ceelen, W. Ouwerkerk, J. Tromp, S. M. Figarska, S. D. Anker, K. Dickstein, G. Filippatos, F. Zannad, M. Metra, L. Ng, N. Samani, D. J. van Veldhuisen, C. Lang, C. S. Lam and A. A. Voors, “Machine learning based on biomarker profiles identifies distinct subgroups of heart failure with preserved ejection fraction,” European Journal of Heart Failure, vol. 23, p. 983–991, March 2021.
[15] M. Tabassian, I. Sunderji, T. Erdei, S. Sanchez-Martinez, A. Degiovanni, P. Marino, A. G. Fraser and J. D’hooge, “Diagnosis of Heart Failure With Preserved Ejection Fraction: Machine Learning of Spatiotemporal Variations in Left Ventricular Deformation,” Journal of the American Society of Echocardiography, vol. 31, p. 1272–1284.e9, December 2018.
[16] Å. K. Hedman, C. Hage, A. Sharma, M. J. Brosnan, L. Buckbinder, L.-M. Gan, S. J. Shah, C. M. Linde, E. Donal, J.-C. Daubert, A. Mälarstig, D. Ziemek and L. Lund, “Identification of novel pheno-groups in heart failure with preserved ejection fraction using machine learning,” Heart, vol. 106, p. 342–349, January 2020.