Fielder Fc to Navigate Acute Angle Bifurcations.
Fielder Fc to Navigate Acute Angle Bifurcations.
Dr Anand R Shenoy *1, Dr Kishan Raj K 2, Dr Suraj Sudhish Palavilayil 3
1. Dr Anand R Shenoy, MBBS, MD, DM, FICC, FSCAI, MEAPCI, FESC, FACC, and FRCP (ED), Dept Of Cardiology, Consultant Intervventional Cardiology, Manipal Hospitals, Old Airport Road, Bengaluru, Karnataka, India- 560017.
2. Dr Kishan Raj K, MBBS, MD, DrNB Cardiology Resident, Manipal Hospitals, Old Airport Road, Bengaluru, Karnataka, India- 560017.
3. Dr Suraj Sudhish Palavilayil, MBBS, Manipal Hospitals, Old Airport Road, Bengaluru, Karnataka, India- 560017.
*Correspondence to: Dr Anand R Shenoy, MBBS, MD, DM, FICC, FSCAI, MEAPCI, FESC, FACC, and FRCP (ED), Dept Of Cardiology, Consultant Intervventional Cardiology, Manipal Hospitals, Old Airport Road, Bengaluru, Karnataka, India- 560017.
Copyright
© 2024 Dr Anand R Shenoy. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 18 June 2024
Published: 01 July 2024
Abstract
Guidewire manipulation to negotiate branches originating at an acute angle from the parent artery is a frequently encountered challenge by the interventional cardiologist in clinical practice. To date, several methods have been developed, but none of them have a definitive success rate.
We hereby present 2 cases; one with acute angled early bifurcating RCA with lesion near bifurcation and another case with acute angled and tortuous LAD, which were stented successfully with the help of Fielder FC wire to help in manoeuvring the arteries without which crossing the lesion would have been a rather difficult task.
With this we would like to emphasise on the need for proper wiring technique in acute angled as well as tortuous arteries to prevent complications as well as to help ease the procedure itself.
KEY WORDS: Fielder FC wire, vascular bifurcations, Tortuous vessels
Fielder Fc to Navigate Acute Angle Bifurcations.
Introduction
Percutaneous coronary intervention (PCI) provides a significant challenge in negotiating acute-angle bifurcations even for the considerably skilled interventionist, and significant angulations are a predictor of procedural failures and complications. To date, several methods have been developed, but none of them have a definitive success rate. Fielder FC guidewire is associated with a relatively shorter procedure time and lower contrast amount, as Fielder FC guidewire could cross these lesions with ease compared to other guidewires. The quantum of contrast media is closely related to the incidence of CIN, and several studies have shown that the volume of contrast media is an independent risk factor for the development of contrast-induced acute kidney injury
Case Report
Case 1
60 year old male known diabetic, hypertensive and dyslipidaemic presented with unstable angina, Coronary angiogram revealed Mid RCA pre crux lesion of 80-90% stenosis and PDA and PLV arising from Mid RCA (Fig 1). It was an angulated bend post bifurcation and hence Fielder FC wire support was taken to easily manipulate the vascular bifurcation (Fig 2) and successful PTCA+ stent to Mid RCA was done with 3x24mm Yukon choice flex stent (Fig 3& 4). TIMI III flow was achieved and post procedure period was uneventful.
FIG 1: Early bifurcating dominant RCA, Pre crux 90% stenotic lesion, with acute angled bifurcation
FIG 2: Successful manoeuvring of Fielder FC through the bifurcation to PLV
FIG 3: Stent deployment
FIG 4: Final Shot
Case 2
77 year old male presented with Effort angina, TMT positive for inducible ischemia, Old AWMI (2014) with EF 44%- Details of the same not known, Coronary angiogram revealed Double Vessel Disease with proximal LAD 90% stenosis and RCA 50-60% stenosis. LAD had a tortuous course with an acute angled bifurcation from Left Main artery (Fig 5 & 6). He underwent successful PTCA+ Stent to LAD with 3x18mm Yukon choice flex stent done with the help of 0.014x180cm Fielder FC wire and guide plus II (Fig 8). LCx was also stented with 2.75x16mm Yukon choice flex stent without any difficulty.
FIG 5 & 6: Tortuous and acute angled LAD
FIG 7: Navigating Fielder FC
FIG 8: Stent Placement Using Guideliner Support
Discussion
Coronary bifurcation lesions are found in approximately 15% to 20% of PCIs, and they have been shown to be associated with lower procedural success rates compared with non-bifurcation lesions.1
Successful wiring to approach branches is essential for a successful percutaneous coronary intervention (PCI) of bifurcation lesions.2,3 However, wiring of side branches with an extremely angulated take-off can be challenging, as the wire is prone to prolapse into non-targeted branches if a conventional wiring technique is used. For such lesions, the double-lumen Crusade catheter (Kaneka, Osaka, Japan) is commonly used.
Similarity between both of our cases were that both were tortuous and acute bifurcation vessels which required special hardware to manoeuvre. Case 1 had lesion pre bifurcation where as Case 2 had lesion post bifurcation. Post bifurcation lesion could be stented only with the help of microcatheter to manoeuvre through the acute angle.
Fielder guidewires come with a tip load of 0.8 gf with Hydrophilic coating over polymer jacket of about 16cm. It has excellent torquability and is easy to manoeuvre across difficult lesions and tortuous arteries.
The use of plastic-jacket hydrophilic wires is reasonable for this procedure, because they offer both good controllability for engaging the ostium of extremely angulated branches and better trackability for advancement deep into the vessel because of lower resistance, even under conditions of poor pushability. Kawasaki et al succeeded in treating an ostial LAD, which bifurcated at an acute angle from the LMT, using a bare wire.4
Conventional wiring is almost impossible for some extremely angulated lesions, even with the support of a Crusade catheter. According to in vitro bench tests, when the bifurcation angle is larger than 150°, the wire cannot approach the branch using a conventional antegrade wiring technique even under the support of a Crusade catheter.5
We have presented here two cases with almost 150 degree angulation which we had wired in conventional antegrade wiring technique, this is very difficult and needs certain expertise to manoeuvre the same.
In conclusion, the right hardware in the hands of a skilful operator is the recipe for success in interventional cardiology.
Reference
1. Louvard Y, Lefevre T, Morice MC. Percutaneous coronary intervention for bifurcation coronary disease. Heart. 2004;90:713–722
2. Su MI, Chen CY, Yeh HI, Wang KT. Concise review of optical coherence tomography in clinical practice. Acta Cardiol Sin. 2016;32:381–386
3. Zhang L, Zhong W, Luo Y, Chen L. A pilot study on culottes versus crossover single stenting for true coronary bifurcation lesions. Acta Cardiol Sin. 2016;32:450–459
4. Kawasaki T, Koga H, Serikawa T. New bifurcation guidewire technique: a reversed guidewire technique for extremely angulated bifurcation — a case report. Catheter Cardiovasc Interv. 2008;71(1):73-76.
5. Watanabe S, Saito N, Bao B, et al. Microcatheter-facilitated reverse wire technique for side branch wiring in bifurcated vessels: an in vitro evaluation. EuroIntervention. 2013;9:870–877.

Figure 1

Figure 2
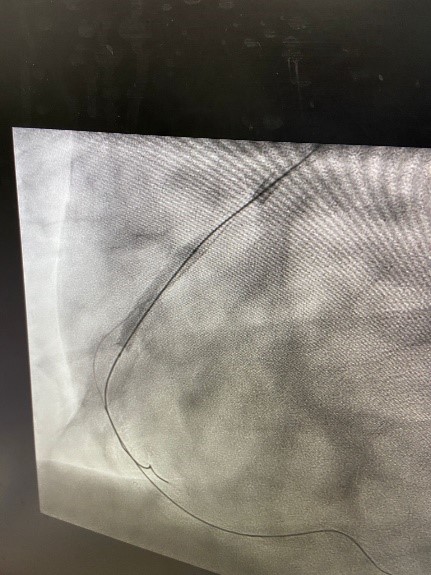
Figure 3

Figure 4
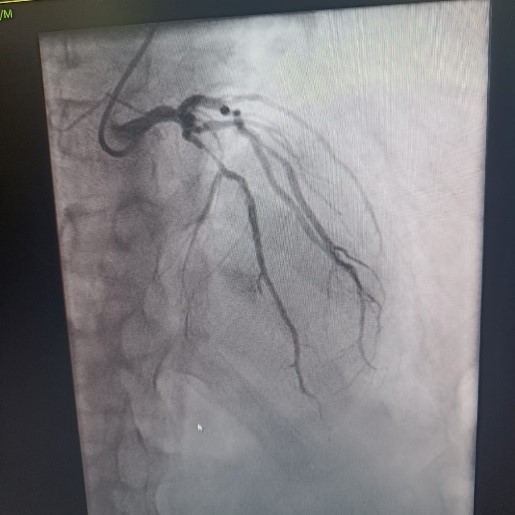
Figure 5

Figure 6

Figure 7
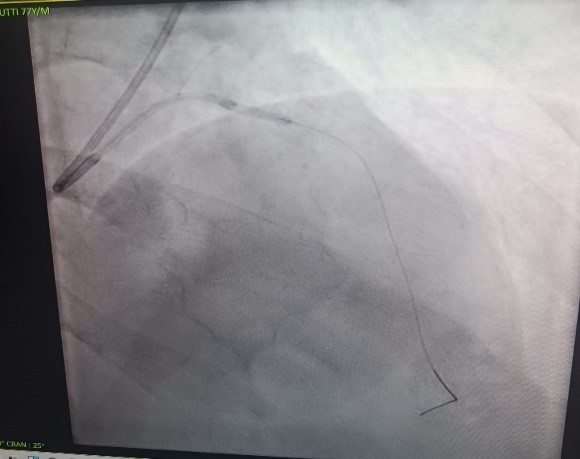
Figure 8