Gastric Tuberculosis-The Truth Beneath the Surface!!!!!
Gastric Tuberculosis-The Truth Beneath the Surface!!!!!
Madhulika Harkare 1, Parikshit Thakare 2*, Kamlesh Patil 3, Gaurav Dubey 4, Anil Rohankar 5
1. Madhulika Harkare-Junior resident Dr.PDMMC Amravati
2. Parikshit Thakare –Senior resident Dr PDMMC Amravati
3. Kamlesh Patil-Assistant Professor Dr.PDMMC Amravati
4. Gaurav Dubey-Associate Professor Dr PDMMC Amravati
5. Anil Rohankar- Senior resident Dr PDMMC Amravati
Correspondence to: Parikshit Thakare Senior Resident, Dr.Punjabrao Deshmukh Memorial Medical College, Amravati.
Copyright
© 2024 Parikshit Thakare. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 06 June 2024
Published: 01 July 2024
Abstract
Tuberculosis is major health concern in India. Pulmonary Tuberculosis is the most common tuberculosis while lymph node tuberculosis is most common extra pulmonary tuberculosis. We encounter one such case of gastric tuberculosis which is very rare.
A 28-year-old female presented with abdominal pain, fever, and loss of weight and loss of appetite since 4 months. The symptoms were not completely relieved after taking symptomatic treatment. On subsequent evaluation patient was found to be anemic and presence of subpyloric lymphadenopathy. The upper gastro-intestinal endoscopy was suggestive of fundal gastric ulcer with circumferential soft lesion and on taking biopsy of it found to be tuberculosis. Subsequently, she was diagnosed with military involvement too.
Gastric Tuberculosis-The Truth Beneath the Surface!!!!!
Introduction
Gastrointestinal tuberculosis is an uncommon entity, in which clinical presentation can be widely variable, from mild and nonspecific symptoms to an acute abdomen and gastrointestinal bleeding. The gastrointestinal tuberculosis is sixth most common cause of extrapulmonary tuberculosis and ileocaecal region is the most common site 1gastrointestinal (GI) tuberculosis (TB) accounts for 1%–3% of all TB cases worldwide, TB of the stomach is extremely rare and accounts for 1%–2% of all GI TB. Little is known about this entity.
Case report
A 28 year old female, non addict, immunocompetent female presented with complaints of abdominal pain, fever along with anorexia and loss of weight since 4 months. For these complaints she received symptomatic treatment which was not associated with any relief. Her past medical and family histories were irrelevant. Patient denied any other clinical symptoms and her physical examination showed palor.
All her routine blood investigations were normal except hemoglobin level of 10 grams per deciliter. Subsequently USG abdomen was done which was suggestive of subpyloric lymphadenopathy and presence of small areas of thickened bowel loop.Patient was posted for upper gastro-intestinal endoscopy for further assessment.
Figure 1-Endoscopic image showing gastric ulcer in fundic region
Figure 2- Chest X-ray & Computed tomography of thorax showing miliary nodules in lungs
Figure 2 (a), Figure 2 (b)
The endoscopy findings were consistent with presence of ulcer in fundic region (Figure 1) along with presence of well circumscribed circumferential soft,friable and fleshy lesion of approxiametely 1 cm. The bite on bite biopsies were taken from that area and send for analysis. The biopsy report was consistent with caseating granulomas with numerous acid-fast bacilli detected with Ziehl-Neelsen stain and immunohistochemical analyis for Helicobacter pylori was negative. On subsequent evaluation patient was found to have multiple military nodules on chest X-ray (Figure 2a) and which was confirmed with computed tomography of thorax (Figure 2b).
The patient was started on anti-tubercular therapy according to her weight as per National Tuberculosis Elimination Programme with isoniazid, rifampin, pyrazinamide, and ethambutol for 2 months, followed by 4 months of isoniazid, rifampin and ethambutol.
The patient came for follow up after 1 month of therapy which was associated with clinical improvement in the form of weight gain, no abdominal pain and no history of fever along with radiological improvement on her chest X-ray. Endoscopic reassessment after 2 months later was unremarkable.
Discussion
Tuberculosis is endemic in India. Pulmonary tuberculosis accounts for 85% cases and extrapulmonary cases accounts for 15% of cases. Abdominal tuberculosis is the sixth most common site of extrapulmonary tuberculosis. Ileocaecal region is the most common site of gastrointestinal tuberculosis followed by ascending colon, jejunum, appendix, duodenum and stomach.2
Gastric tuberculosis is a rare entity, accounting for 0.5–3% of GI tuberculosis cases 3.
Several factors have been described that seem to be responsible for the rare gastric involvement, namely,
(1) Low pH in the gastric lumen, which has a bactericidal role;
(2) The absence of lymphatic follicles;
(3) The local immunity induced by the integrity of gastric mucosa; and
(4) fast gastric emptying 4,5.
Most cases of gastric tuberculosis occur in patients with active pulmonary tuberculosis 6,7due to swallowing infected sputum, but it may also be secondary to hematogenous or lymphatic spread and contiguous spread from the adjacent organ.
When no other tuberculosis foci are identified after an extensive workup, it is called primary gastric tuberculosis. The clinical presentation of gastric tuberculosis is entirely non-specific with complaints of epigastric pain,vomiting and weight loss 8,9. Our patient presented with complaints of abdominal pain and other constitutional symptoms.
Gastric outlet obstruction is the most common presentation of tuberculosis10Other presentations reported in literature are haematemesis 11,perforation12,13, non healing ulcer14, and dysphagia15.Our patient reported sub-pyloric small lymphadenopathy on ultrasonography.
The diagnosis of tuberculosis requires demonstration of caseating epithelioid granuloma or presence of acid fast bacilli in tissue 15.For our case it was evident on the upper gastrointestinal endoscopy with presence of acid fast bacilli.
Antitubercular chemotherapy forms the mainstay of treatment when diagnosis of gastric tuberculosis is made. When diagnosis of TB is established, most lesions regress with appropriate antitubercular treatment and do not require excision.16 Our patient showed marked clinical improvement after inititation of anti-tubercular therapy along with radiological improvement too.
Conclusion
In patients with vague abdominal symptoms and those not responding to symptomatic treatment or antiulcer therapy should always keep differential in mind like gastric tuberculosis. Gastric tuberculosis produces a diagnostic challenge as it can mimic peptic ulcer disease and malignancy.
In conclusion a high level of suspicion is required for the diagnosis of gastric TB, especially in endemic countries such as India. Diagnosis of gastric tuberculosis is of utmost importance and once diagnosed properly, these patients can have good outcome with timely administration of antitubercular therapy and only few require endoscopic or surgical interventions.
References
1. Manoria P, Gulwani HV. Gastric tuberculosis presenting as non healing ulcer: a case report. Indian J Tuberc. 2019 Oct 1;66(4):502-4.
2. Marshall JB. Tuberculosis of the gastrointestinal tract and peritoneum. American Journal of Gastroenterology (Springer Nature). 1993 Jul 1;88(7).
3. Chaudhary P, Khan AQ, Lal R, Bhadana U. Gastric tuberculosis. Indian Journal of Tuberculosis. 2019 Jul 1;66(3):411-7.
4. Choi EH, Coyle WJ. Gastrointestinal tuberculosis. Microbiol Spectr. 2016; 4 (6).
5. Debi U, Ravisankar V, Prasad KK, Sinha SK, Sharma AK. Abdominal tuberculosis of the gastrointestinal tract: revisited. World Journal of Gastroenterology: WJG. 2014 Oct 10;20(40):14831.
6. Seth AK, Nijhawan VS, Bhandari MK, Dhaka RS, Kochar SK. Gastric tuberculosis: a case report. Medical Journal Armed Forces India. 1998 Jul 1;54(3):278-9.
7. Shah J, Maity P, Kumar-M P, Jena A, Gupta P, Sharma V. Gastroduodenal tuberculosis: a case series and a management focused systematic review. Expert Review of Gastroenterology & Hepatology. 2021 Jan 2;15(1):81-90
8. Subei I, Attar B, Schmitt G, Levendoglu H. Primary gastric tuberculosis: a case report and literature review. American Journal of Gastroenterology (Springer Nature). 1987 Aug 1;82(8).
9. Sharma BC, Prasad H, Bhasin DK, Singh K. Gastroduodenal tuberculosis presenting with massive hematemesis in a pregnant woman. Journal of Clinical Gastroenterology. 2000 Apr 1;30(3):336.
10 Tromba JL, Inglese R, Rieders B, Todaro R. Primary gastric tuberculosis presenting as pyloric outlet obstruction. American Journal of Gastroenterology (Springer Nature). 1991 Dec 1;86(12).
11. Wig JD, Vaiphei K, Tashi M, Kochhar R. Isolated gastric tuberculosis presenting as massive hematemesis: report of a case. Surgery Today. 2000 Oct;30:921-2.
12. ED P. Tuberculosis of the stomach and the stomach in tuberculosis; a review with particular reference to gross pathology and gastroscopic diagnosis. Am Rev Tubere. 1950;61:116-30.
13. CLAGETT OT, WALTERS W. Tuberculosis of the stomach. Archives of Surgery. 1938 Sep 1;37(3):505-20.
14.Chetri K, Prasad KK, Jain M, Choudhuri G. Gastric tuberculosis presenting as non-healing ulcer: case report. Tropical gastroenterology: official journal of the Digestive Diseases Foundation. 2000 Oct 1;21(4):180-1.
15. Amarapurkar DN, Patel ND, Amarapurkar AD. Primary gastric tuberculosis–report of 5 cases. BMC gastroenterology. 2003 Dec;3:1-4.
16. Anand BS, Nanda R, Sachdev GK. Response of tuberculous stricture to antituberculous treatment. Gut. 1988 Jan 1;29(1):62-9.
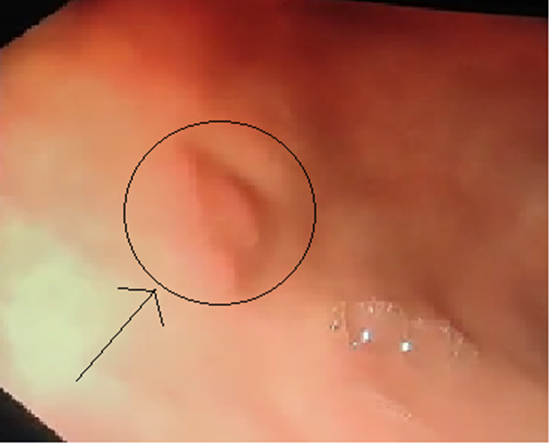
Figure 1

Figure 2
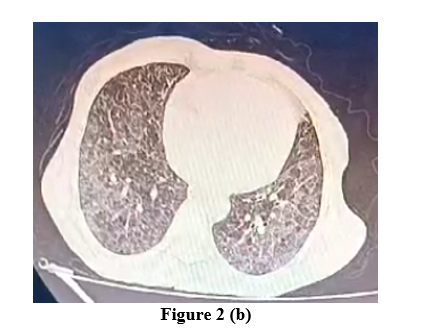
Figure 3