Breastfeeding Versus Dextrose as Analgesic in Newborns: A Prospective Study
Breastfeeding Versus Dextrose as Analgesic in Newborns: A Prospective Study
Gurmeet Singh 1, Payal Mittal 2, Saim Ali 3, Rajender Singh *4, Shehraz Firoz 5, Sonia Bhatt 6
1,3,4. Assistant Professor, Department of pediatrics, F.H. Medical College, Etmadpur.
2. Associate Professor, Department of pediatrics, F.H. Medical College, Etmadpur.
5,6. Professor, Department of pediatrics, F.H. Medical College, Etmadpur.
*Correspondence to: Rajender Singh. Assistant Professor, Department of pediatrics, F.H. Medical College, Etmadpur.
Copyright
© 2024: Rajender Singh. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 20 July 2024
Published: 01 August 2024
DOI: https://doi.org/10.5281/zenodo.13267899
Abstract
Aim: To assess the level of pain in infants in the control group and the experimental group before and after routine procedure. Secondly, to determine the effect of peroral dextrose solution and breast feeding on procedural pain in infants in the experimental group.
Materials and Methods: This index study was conducted in Department of Pediatrics of F.H. Medical college, Etmadpur, India. The newborns enrolled were late pre-term and full term, having gestational age 34 weeks to 42 weeks. The enrolled newborns were either partial or complete breast-feeding and were assigned heel prick procedure. Newborns were randomized into 2 groups for analgesia, i.e. breast-feeding and 25% peroral dextrose solution. The independent variables were peroral 25% dextrose solution and breast feeding. The dependant variable were procedural pain (heel prick) in the study groups. Primary outcome variable were Premature Infant Pain Profile score. PIPP score consists of 2 physiologic indicators of pain (i.e. heart rate and oxygen saturation), two contextual factors (i.e. corrected gestational age and behavioral state) and three behavioral indicators (i.e. brow bulge, eye squeeze, and nasolabial furrow). Greater the PIPP score, higher the pain perception. PIPP score were assigned prior to stimulus and post 30 sec after the stimulus.
Results: The mean pain score of 9.7 and 4.7 in dextrose and breast-feeding groups respectively proves significant difference (p-value 0.000) were found in them. Lesser mean score in breast feeding group signifies the importance of breast feeding during painful procedures as compared to dextrose. The mean pain scores of both groups showed that pain were more prevalent in dextrose group than breast feeding group. Hence it is clear that the effect of breast feeding reduced the pain among newborns in comparison to dextrose.
Conclusion: Breast feeding and 25% peroral dextrose solution have analgesic effect during procedural pain. Breast feeding has significantly superior analgesic effect during procedural pain among newborns as compared to dextrose. Breast feeding should preferably being chosen as non-pharmacological intervention during infliction of procedural pain in newborns.
Keywords: Breast-Feeding; New-born; PIPP; Analgesia; Maternal Holding; Pacifier; Pain.
Breastfeeding Versus Dextrose as Analgesic in Newborns: A Prospective Study
Introduction
Noxious stimuli in newborns have deleterious effect on their health. Despite of being aware of this fact, newborns are still being subjected to repeated painful stimuli as a routine practice in neonatal intensive care units without proper analgesia International Association of the Study of Pain (1) states that pain as “noxious emotional and sensory perception due to either actual or potential tissue loss”.
Extended pain procedures stimulate oxidative stress & inflammatory reactions and halts development of pre-myelinating cells. (3)
Premature babies have extended activation of hypothalamic-pituitary axis which leads to prolonged alteration in beinghavioural, hormonal, and physiological mechanisms. (2)
Amongst the routinely performed procedures in NICU, heel prick is commonly beinging practiced for capillary sampling. (4)
Ranger, et al (5) found that repetitive skin prick procedures in newborns eventually leads to thinner cortical gray matter during their childhood period. Extended research in this matter concludes that repetitive painful procedures in newborns lead to poor cognitive and motor function during their forth coming development & also sub-optimal behaviors during their later life. (6)
Short term painful procedures in newborns (heel prick), non-pharmacological pain-relieving interventions are effective, economical and safe as compared to pharmacological pain-relieving interventions. Non-pharmacological procedures likewise, swaddling, peroral dextrose solution, breast feeding, non-nutritive sucking (NNS), facilitated tucking and skin- to-skin contact had been effectively used for reduction of minor painful procedures in newborns. (7) Pain perception during routine painful procedures in newborns can being effectively demonstrated by pain judgmental tools such as PIPP scale (Premature Infant Pain Profile) devised by Stevens and colleagues (8).
Any pain-relieving measure in newborns which is cost effective, natural, & safe can being ideal for use in NICU receiving heel prick. Ongoing research has proved that both breast feeding & perperoral dextrose solution are effective measures to alleviate pain in newborns during painful procedures such as heel prick.
Aim and Objective
- To measure the effect of peroral dextrose solution or breast feeding on procedural pain in newborns of experimental group.
- To quantify the association of level of pain with sample characteristics of the newborns enrolled in this study.
Materials and Methods
Study were conducted in neonatal unit of F.H. Medical College, Department of Pediatrics, Etmadpur. This study includes 104 newborns. Sample size is estimated based on previous studies 6. Where in experimental group only 30% subjects had severe pain in post vaccination whereas in control group it were in 62.9% subjects. Our sample size came out to being 47 subjects per group at a power of 90% & confidence interval of 95 %. For possible dropouts, it were decided to include 10% extra subjects so finally it were decided to include 104 subjects in total for both the groups.
The criteria to being met during the study were as follows: Inclusion criteria: Newborns 0 to 28 days of age (with gestational age 34 weeks to 42 weeks) who are undergoing heel prick for blood sampling and who are on exclusive or partial breast feeding. Gestational age were estimated by New Ballard’s Score. Exclusion criteria: Those excluded were sick babies with unstable vitals or on oxygen or with history of severe birth asphyxia, with neurological abnormalities, facial palsy, or glucose intolerance. Infants at high risk for necrotizing enterocolitis, infants with severe birth asphyxia (i.e. Apgar score of 3 or less than 3 at 1 minute), infants with congenital heart disease that are not on established feeds, infants with feeding intolerance, infants with absent bowel sounds. Newborns with major congenital defects such as cleft lip, cleft palate, esophageal atresia or tracheal esophageal fistula. Infants who are sedated or on other pain medications.
Independent research variables were peroral 25% dextrose solution and breast feeding and dependant variable were procedural pain (heel prick) in newborns.
The subjects were randomized into 2 groups of 52 babies each through computer generated random numbers and these numberings were being put in serially ordered opaque sealed envelopes. The person generating random numberings and placing them serially in sealed envelope were not being involved in the study.
Breast feed group: Babies in breastfeed group were being breastfed throughout the intervention, starting 2 minutes before, during and 2 minutes after the procedure. During breast feeding, only one half of the face were to being visible; thus, all facial parameters were based on the facial side which observer can see. However if for some reason a parameter cannot be seen on both sides, a zero score were being given to that parameter.
25% dextrose group: 2 ml of 25% dextrose was given per orally by a sterile syringe 2 minutes prior to heel prick. Heel prick were being given while the baby is in the mother’s lap. All the events were being recorded on a video camera by a female investigator to ensure mother’s compliance. The principal investigator recorded the vital parameters for a total duration of four minutes after the prick and analyzes the outcome variables from the video recording in all the subjects. All enrolled babies were being fed at least 1 hour before the procedure. All the babies were being held in the mother’s lap during the procedure. The mothers were being allowed to hold, talk to, or rock the baby during the procedure in both the groups. Written informed consent was taken from the parents
Judgement of neonatal pain was being done by using Premature Infant Pain Profile (Appendix-3). The minimum score is 0 and maximum score is 21. PIPP score includes two physiologic indicators of pain (i.e., heart rate and oxygen saturation), three behavioural indicators (i.e., brow bulge, eye squeeze, and nasolabial furrow); and two contextual factors (i.e., corrected gestational age and behavioral state). A 4-point scale (0–3) were being used. Scores on the seven indicators are added for a total pain score. Higher is the score greater the pain. PIPP score were being assessed before giving the stimulus and again at 30 sec, 1 min, 2 min and 4 min after the stimulus.
Results were being analyzed by using appropriate statistical tests by a statistician who were not being a part of the study.
Results
The current study “Breast Feeding Versus Dextrose as analgesic in newborns” was conducted in F.H. Medical College on 104 newborns attending the hospital. Random seed were generated and newborns were divided into two groups on the basis of identification number assigned to them randomly. Dextrose were used for newborns of one group(n-57), simultaneously breast feeding were used for another group(n-49) during heel Prick and the comparison were done on the basis of various parameters according to PIPP criteria. The profile of the newborns were as described in the tables below: newborn aged 1 to 10 days were included in the study with mean age 1.2 days. The male (65) and females (41) were in the gestation age of 32 to 41.1 weeks with men gestation age of 37.7 weeks. The average birth weight was 2648.1 ± 412.2 with range 1563-3632. The overall pain score among 106 newborn ranged from 3 to 13 with 7.4 ± 3.3 mean score.
Age distribution of children in both groups. The distribution in both groups was almost same and thus homogenous. The non-significant p-value (0.842) shows that both the groups had almost equal age distribution with highest number of 1 day newborn 24(42.1%) and 23(46.9%) in dextrose and breast feeding groups respectively.
Although the number of males was more among the total newborn but the above tables shows that the distribution in both groups was not statistically significant (p-value 0.075). The dextrose group had 30(52.6%) males as well as 27(47.4%) females. On the other hand 35(71.4%) males and 14(28.6%) females were in the breast feeding group.
Although 4(7%) children with extremely low birth weight were in dextrose group compared to none in breast feeding group, yet the difference was not significant (p-value 0.090).
|
S. No. |
Parameter |
0 |
1 |
2 |
3 |
Mean ± SD |
|
1. |
What is gestation of infant? |
89(84.0) |
17(16.0) |
0(0.0) |
0(0.0) |
0.2 ± 0.3 |
|
2. |
Behaviperoral state before the procedure (15 sec.). |
42(39.6) |
38(35.8) |
13(12.3) |
13(12.3) |
1.0 ± 1.0 |
|
3. |
Difference between Baseline HR and maximum HR during the procedure. |
26(24.5) |
37(34.9) |
43(40.6) |
0(0.0) |
1.2 ± 0.8 |
|
4. |
Difference between baseline SO2 % and minimum SO2 % during the procedure. |
64(60.4) |
22(20.8) |
20(18.9) |
0(0.0) |
0.6 ± 0.8 |
|
5. |
Observe the infant for 30 sec immediately after the procedure for brow bulge. |
27(25.5) |
36(34.0) |
23(21.7) |
20(18.9) |
1.3 ± 1.0 |
|
6. |
Observe the infant for 30 sec immediately after the procedure for eye squeeze. |
14(13.2) |
13(12.3) |
57(53.8) |
22(20.8) |
1.8 ± 0.9 |
|
7. |
Observe the infant for 30 sec immediately after the procedure for nasolabial furrow. |
26(24.5) |
38(35.8) |
22(20.8) |
20(18.9) |
1.3 ± 1.0 |
|
|
Total PIPP score |
|
|
|
|
7.4 ± 3.3 |
The gestation age according to PIPP criteria of both groups has been shown Figure 5 above. The percentage distribution was almost same in both groups with mostly infants in more than 36 weeks age group 84.2% and 83.7% respectively.
In our study , 89 out of 106, newborn having 36 weeks or more gestational age at birth were well distributed between both groups 48(84.2%) in Dextrose and 41(83.7%) in breast feeding group. The remaining 17 children were also showing the same trend and thus statistically non-significant (p-value 0.940) according to chi square test.
Figure 1: Behavioral state of newborn in both groups
The above figure shows the behavioral state of newborn in both groups before procedure. Most of the children 98.2% in dextrose group were in active and quite active state whereas 51% children in breast feeding group were in sleeping state.
The mean increase in heart rate was more 1.7 in dextrose group as compared to 0.5 in breast feeding group. The mean comparison was statistically significant.
SPO2 fall during procedure was different in both dextrose and breast-feeding groups. More fall 5.0- 7.4% was recorded in dextrose group 20(35.1%) compared to breast feeding group 48(98.0%) with 0 – 2.4%.
Maximum brow bulging ≥ 70% of time was recorded in 35.1% newborn of dextrose group. On the contrary 53.1% newborn of breast-feeding group showed none (0-9% of time).
The significant difference (p-value 0.000) while eye squeezing by newborn of both groups proves that 21(36.8%) children in dextrose groups bear more pain as compared to breast feeding group 1(2.0%).
With higher mean score 2.3 newborn of dextrose group shows more pain as compared to 1.2 mean in breast feeding group. The significant p-value (0.000) gives a clear opinion that breast feeding decreases the effect of pain during procedures.
Figure 2: Pain level among newborn of both groups
Overall pain level of newborn in both groups has been depicted in Figure 2. In breast feeding group 89.8% children had no or minimal pain. In dextrose group maximum children 73.7% had reported mild to moderate pain.
Discussion
In our study, overall average revised- PIPP score were7.4±3.3rangingfrom 0-21. The mean PIPP score of 9.7and 4.7 in dextrose and breast-feeding groups respectively. Similarly, Stevens et al, (11) in their study on initial development and validation of PIPP scale during heel prick found mean PIPP score to being 8.8 ± 2.4. Heish et al, (12) found in their study, PIPP score to being 8.6 (mean= 7-12) among breast feeding group and 9.5 (6.75-11.25) among peroral dextrose group. Codi Pietro et al, (13) in their study of breastfeeding or peroral sucrose solution in term newborns receiving heel prick reported that the median difference of PIPP score were 5.0 among the two groups. But Gradin et al, (14) during their comparison of analgesic effect of breastfeeding versus glucose alone, and in combination, with controls receiving no interventions, on full term infant’s pain response during heel prick, found that although breastfeeding alone decreased duration of crying time compared to control, PIPP scores and crying duration were lowest in the group receiving both interventions.
Gradin et al (14), in their study found that the PIPP score (median) were 7, which is lower in breastfed/dextrose group than during breastfeeding alone with mean PIPP score of 10. There were a similar difference between the PIPP scores in the dextrose fed group were 9 in comparison to the control groups where PIPP score were 11.
In this index study, in dextrose group 94.8%babies had minimal to moderate pain, with 3(5.3%) having severe pain. But 44(89.8%) babies having no or minimal pain were spotted in breast feeding group, 10.2% suffered from mild to moderate pain. None of the babies in breast feeding group showed symptoms of severe pain. The mean pain score of 9.7 and 4.7 in dextrose and breast-feeding groups respectively proves significant difference (p-value 0.000) were found in them.
Similarly, Heish et al,(12) found in their study, PIPP score to being 8.5 (mean= 6-11) among breastfeeding group and 9.5 (mean= 6.75-11.25) among peroral glucose group. Their study showed significant statistical difference(p<0.05) among breastfeeding and peroral dextrose groups.
Codipietro et al, (13) studied that median PIPP scores were 3.0, in the breastfeeding group which were lesser than those babies receiving 1 ml sucrose solution, with PIPP score of 8.5. The median group difference were 5.0.
From the current discussion, inference can being drawn that lesser mean score (PIPP score) in breast feeding group signifies the importance of breastfeeding during painful procedures as compared to dextrose. Hence it is clear in our study that the effect of breast feeding reduced the pain among newborns in comparison to dextrose during heel prick.
Conclusion
In this index study, 104 newborns aged 1 to 10 days were included with mean age 1.2 days. The overall pain score among106 newborns ranged from 3 to13 with7.4 ± 3.3 mean score. In breast feeding group 89.8% children had no or minimal pain. In dextrose group maximum children 73.7% had mild to moderate pain. In dextrose group 94.8% children had minimal to moderate pain, with 3 (5.3%) having severe pain. None of the children in breast feeding group showed features of severe pain. Lesser mean score in breast feeding group signifies the importance of breast feeding during painful procedures as compared to dextrose.
The mean pain scores of both groups showed in the above figure 13 that pain was more prevalent in dextrose group than breast feeding group. Hence it is clear that the effect of breast feeding reduced the pain among newborn in comparison to dextrose.
References
1.International Association for the Study of Pain. (2005). Core curriculum for professional education in pain (online). Retrieved August 31, 2007, from www.iasp-pain.orgl
2. Uga E, Candriella M, Perino A, Alloni V, Angilella G, Trada M, et al. Heel prick in newborn during breastfeeding: an evaluation of analgesic effect of this procedure. Ital J Pediatr.2008;34:3.
3. Grunau RVE, Graig KD. Pain expression in newborns; facial action and cry. Pain.1987;28:395-410.
4. Carbajal R, Chauvet X, Couderc S, Olivier-Martin M. Randomized trial of analgesic effects of sucrose, glucose and pacifiers in term newborns. BMJ. 1999;319:1393-7.
5. Bildner, J., & Krechel, S. (1996). Increasing staff nurse awareness of postoperative pain management in the NICU. Neonatal Network,15(1),11-16.
6. Lawrence, J., Alcock, D., McGrath, P., Kay, J., MacMurray, S., & Dulbeingrg, C. (1993). The development of a tool to assess neonatal pain. Neonatal Network,12(6),59-66.
7. Fitzgerald, M., Millard, C., & McIntosh, N. (1989). Cutaneous hypersensitivity following peripheral tissue damage in newborn infants and its reversal with topical anaesthesia. Pain,39,31-36.
8. Craig, K., Whitfield, M., Gronau, R., Linton, J., & Hadjistavropoulos, H. (1993). Pain in the pretennneonate: Beinghaviperperoral and physiological indices. Pain, 52,287-299.
9. Slater L, Asmerom Y, Boskovic DS, Bahjri K, Plank MS, Angeles KR, et al. Procedural pain and oxidative stress in premature newborns. J Pain 2012;13:590–7.
10. Stevens BJ, Gibbins S, Yamada J, et al. The premature infant pain profile-revised (PIPP-R): initial validation and feasibility. Clin J Pain. 2014;30(3):238–243
11. Stevens BJ, Gibbins S, Yamada J, et al. The premature infant pain profile-revised (PIPP-R): initial validation and feasibility. Clin J Pain. 2014;30(3):238–243
13. Codipietro L, Ceccarelli M, Ponzone A. Breastfeeding or per peroral sucrose solution in term newborns receiving heel prick: a randomized, controlled trial. Pediatrics(Evanston IL) 2008;122:e716–21.
14. Gradin M, Finnstrom O, Schollin J. Feeding and per peroral glucose – additive effects on pain reduction in newborns. Early Hum Dev 2004;77:57–65.
15. Harrison D, Loughnan P, Manias E, Gordon I, Johnston L. Repeated doses of sucrose in infants continue to reduce procedural pain during prolonged hospitalizations. Nurs Res 2009;58:427–34.
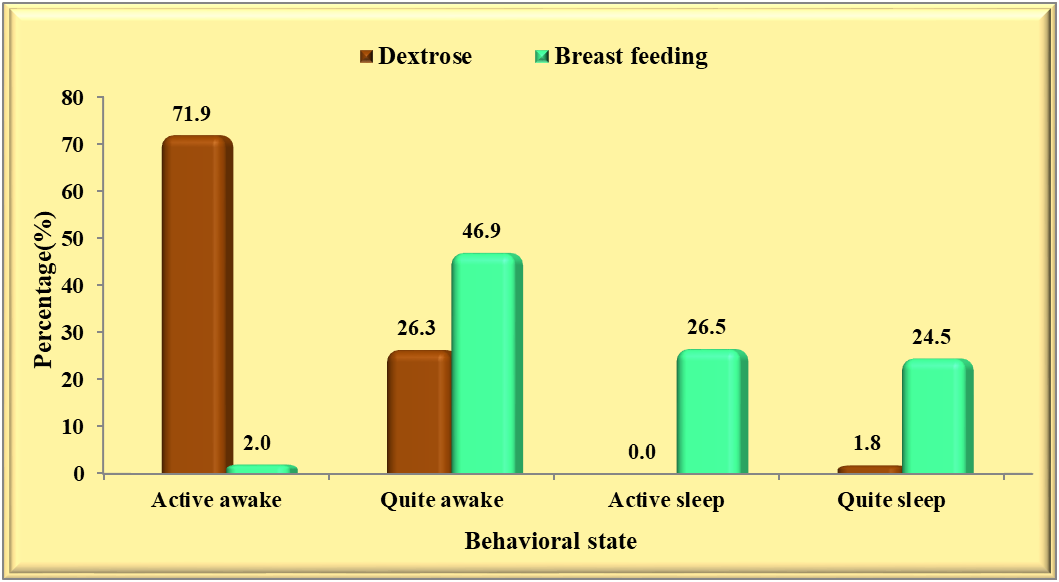
Figure 1
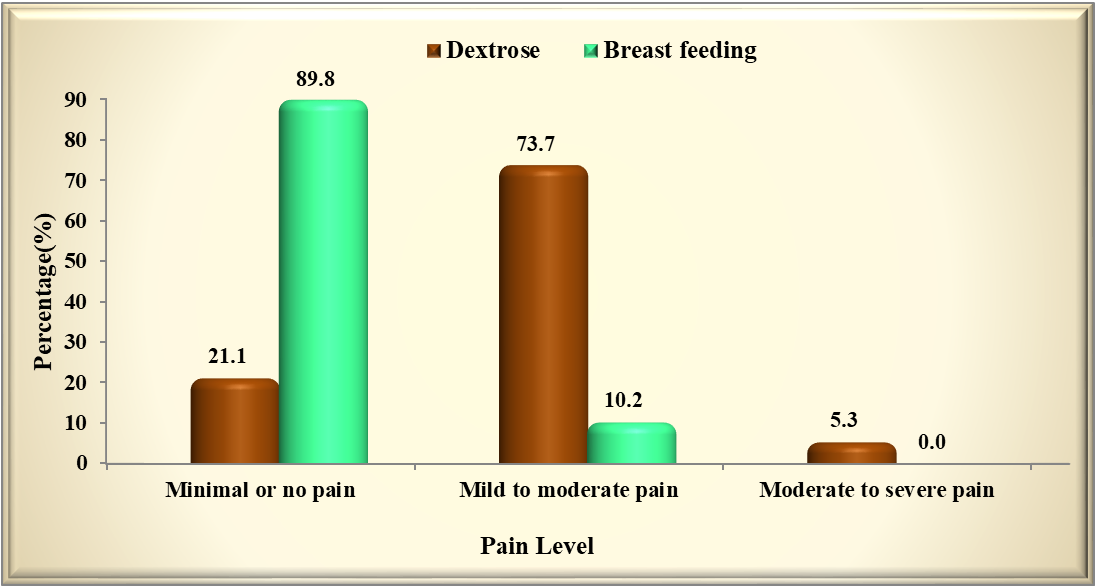
Figure 2