Ameloblastic Fibro-Odontoma: Case Report with Brief Review of Literature
Ameloblastic Fibro-Odontoma: Case Report with Brief Review of Literature
Dr. Ritika Kad 1*, Dr. Susmita Saxena 2, Nithya S 3, Jitin Kharbanda 4
1.Junior Resident, ESIC Dental College and Hospital, Rohini, Delhi.
2.Director Professor and Head of Department, Department of Oral Pathology and Microbiology, ESIC Dental College and Hospital, Rohini, Delhi
3. Assistant Professor, Department of Oral Pathology and Microbiology, ESIC Dental College and Hospital, Rohini, Delhi
4. Professor, Department of Oral Pathology and Microbiology, ESIC Dental College and Hospital, Rohini, Delhi.
*Correspondence to: Dr. Ritika Kad. Junior Resident, ESIC Dental College & Hospital, Rohini, Delhi.
Copyright.
© 2024 Dr. Ritika Kad. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 31 July 2024
Published: 06 August 2024
Abstract
Ameloblastic fibro-odontoma (AFO) is a rare, benign and non-aggressive tumour which has a prevalence of about 0.1-3.4% of all odontogenic tumors. The presentation of this tumor is in the form of asymptomatic swelling associated usually with buccolingual cortical expansion and impacted teeth. Young children of age group 8-12 years are generally affected.
It is a mixed tumour with proliferative odontogenic epithelium embedded in a cellular fibrous ectomesenchyme tissue resembling dental papilla and dental hard tissue. Radiographic features include expansile radiolucency containing radiopaque mass which represents the odontoma part. Histologically this tumour shows presence of ameloblastic follicles along with dentinoid material and enamel-like tissue.
Here we present a case of a 12-year-old girl who reported to ESIC Dental College and Hospital, Delhi with swelling on left mandibular posterior region. Panoramic radiograph and non-contrast computed tomography (NCCT) of face showed the presence of well circumscribed radiolucency with radiopaque mass extending into ramus along with impacted permanent second premolar and first molar of the same side. A provisional diagnosis of complex odontoma was given. Treatment was done by enucleation under general anaesthesia along with prophylactic bone plating. Histopathological examination of the received tissues exhibited the presence of ameloblastic follicles along with dentinoid and enamel-like structure leading to the final diagnosis of ameloblastic fibro-odontoma.
The histopathological features thus can facilitate differentiation of ameloblastic fibro-odontoma from other mixed odontogenic tumors. AFO though considered a hamartoma requires a long term follow up due to its chance of recurrence.
Keywords: Ameloblastic fibro-odontoma, odontogenic tumor, hamartoma, benign tumor.
Ameloblastic Fibro-Odontoma: Case Report with Brief Review of Literature
Introduction
Ameloblastic fibro-odontoma (AFO) is a rare, benign and slow growing odontogenic tumor. It is ‘a neoplasm composed of proliferative odontogenic epithelium embedded in a cellular ectomesenchymal tissue that resembles dental papilla with varying degree of inductive change and dental hard tissue formation’ as defined by WHO [1].
Among the odontogenic tumors, AFO is less common with a prevalence rate of 0.1-3.4% usually affecting individuals in their first and second decades of life [2]. A majority of ameloblastic fibro odontoma is intraosseous and associated with impacted teeth. Approximately 80% of lesions arise in the posterior regions of maxilla or mandible [3].
The common symptoms presented are asymptomatic swelling and delayed eruption of teeth. Radiographic features reveal an expansile radiolucency containing either a solitary radiopaque mass or multiple small opacities which represent the odontoma part of the tumor [1].
Microscopic features include presence of strands, cords, fingers and rosettes of odontogenic epithelial cells resembling dental lamina mostly embedded in a fibrous mesenchyme resembling dental papilla along with the presence of typical odontoma.
AFO being a non-aggressive lesion can be treated by surgical curettage without removal of teeth [4].
Case Report
A female patient of age 12 years reported to ESIC Dental college and hospital, Rohini, Delhi with complaint of swelling with respect to her mandibular left posterior region. The patient had no significant medical or family history.
On extraoral examination patient presented with facial asymmetry (figure 1). A globular swelling of approximate size 2x1.5 cm extending from posterior body of mandible to ramus on the left side was seen on inspection and was bony hard and non-tender on palpation. Intraorally expansion of buccal and lingual cortical plates with vestibular obliteration was present along with tenderness. Tooth 75 was retained with missing 35, 36 and 37.
Panoramic radiograph (figure 2) showed large well demarcated radiolucency containing tooth like radiopaque mass extending from mandibular left primary second molar till the ramus close to the inferior border of mandible along with impacted second premolar and permanent first molar. NCCT face (figure 3) revealed well defined calcified lesion of size 31.5x18 mm in the left ramus region with surrounding hypodense rim causing cortical bone expansion and focal mass effect onthe premolar tooth just anterior to it.
Considering the clinical and radiological findings the provisional diagnosis was given as complex odontoma.
Patient was treated by enucleation of lesion under general anesthesia along with prophylactic bone plating with 2 mm titanium plates and the tissue was sent for histopathological examination (figure 4).
Figure 1 Showing a 12-year-old patient with swelling on mandibular left posterior region A) Frontal profile B) Left profile with swelling C) Right profile
Figure 2 OPG (Orthopantomogram) showing large well demarcated radiolucency containing tooth like radiopaque mass extending from mandibular left primary second molar till the ramus close to the inferior border of mandible along with impacted second premolar and permanent first molar
Figure 3 NCCT face revealed well defined calcified lesion of size 31.5x18 mm in ramus of mandibular left region with surrounding hypodense rim causing cortical bone expansion and focal mass effect on premolar tooth just anterior to it
Figure 4 Post operative OPG of patient showing titanium plate with respect to inferior border of mandible (left side).
Histopathology
On gross examination, the specimen consisted of multiple hard tissue masses with the largest piece measuring 4x3x2 cm attached with multiple soft tissue bits of varying size and shape with one cystic lesion of size about 2 cm in diameter (figure 5). The cystic lesion was kept for routine histological processing and the hard tissue was decalcified along with staining. Two specimens of hard tissue were kept for ground sectioning.
The histopathological examination of soft tissue revealed presence of 2-3 cells layered lining epithelium with absence of rete ridges. Interlacing strands of epithelial cells seen surrounded by fibrous mesenchymal tissue (figure 6). Ameloblastic follicles consisting of peripheral columnar cells and central polygonal cells were present . Few spicules of calcifications along with dentinoid material were also evident. Decalcified hard tissue section revealed mineralised tissue with resting lines and osteocytes indicative of compact bone. The ground section of hard tissue illustrated appearance of enamel in addition to unorganised dentinal tubules and cellular cementum(figure 7).
Thus, the presence of ameloblastic follicles and strands of epithelial cells in fibrous ectomesenchyme accompanied by dental hard tissue formation was suggestive of ameloblastic fibro odontoma.
Figure 5 Gross features of tissue received included: A) Multiple blackish irregular soft tissues of varying size and shape with one cystic lesion of size 2 cm was kept for routine processing. B) Multiple hard tissue specimens with its largest tissue measuring 4x3x2 cm appeared black in colour was kept for decalcification and ground section.
Figure 6 Histopathological examination of soft tissue showing A) interlacing strands of epithelial cells surrounded by fibrous mesenchymal tissue, B) & C) Ameloblastic follicles consisting of peripheral columnar cells and central polygonal cells.
Figure 7 D) Decalcified section of hard tissue showing presence of compact bone along with cementoid tissue; E) & F) Ground section exhibiting presence of enamel and unorganised dentinal tubules with cellular cementum
Discussion
The present case meets the clinicopathological criteria for the diagnosis of ameloblastic fibro- odontoma, which is a rare mixed odontogenic tumor.
The two most common complaints of patient are of painless swelling and delayed eruption of teeth in the affected region. Radiographic features show well circumscribed radiolucency enclosing varying amount of radiopaque mass of different shape and size. Size of lesions may vary from a relatively small one of approximately 1-2 cm in diameter to extremely large lesion involving a considerable portion of body of mandible and even ramus [5] similar to our patient.
Histologically, AFO is considered controversial because of the similarities it shows with ameloblastic fibroma (AF), ameloblastic fibrodentinoma (AFD) and complex odontoma. These are regarded as separate lesions by some pathologists but others consider them as a spectrum starting from AF at one end, complex odontoma at other with AFD, AFO in intermediate stages[3]. When there is formation of dentin or dentinoid like material it is called AFD. The difference between these two lies in the presence of enamel-like structure in AFO. In the present case, enamel-like and dentinoid material with cementum could be appreciated in disorganised pattern unlike composite odontoma which has more of an organised tooth like appearance.
AF matures over a period of time into AFO/AFD and finally results in formation of complex odontoma which suggests that AF occurs at younger age followed by AFO/AFD in older children and finally with odontoma occurring in later age. Hence, age has been declared as a critical feature in the diagnosis of AFO [6].
|
Features of AFO [2] |
|
|
Prevalence rate worldwide |
Rare (0.1-3.4% among odontogenic tumors) |
|
Age group of patients |
8-12 years |
|
Gender predilection (male: female ratio) |
1.85:1 |
|
Site usually affected |
Posterior mandibular region |
|
Radiographic feature |
Mostly unilocular; mixed lesions |
The mixed odontogenic tumors can be either neoplastic or hamartomatous. AFO earlier classified [7] as benign mixed odontogenic tumor has not been included as a separate entity according to WHO 2017 and latest 2022 classification. It has been concluded that ameloblastic fibro-odontoma represents an immature complex odontoma and so is considered a hamartoma rather than a neoplastic odontogenic lesion [1]. AF and AFD can be considered as neoplasm but AFO is a hamartoma representing a stage preceding a developing complex odontoma [2].
AFO is well encapsulated and has less chances of local invasion so the treatment advised is conservative surgery that is by enucleation or through curettage. The affected teeth can be removed or even preservation can be done as in this case. Recurrence might occur in conservative approach, hence long follow up is required [4]. Despite being regarded as a hamartoma some cases of AFO have shown true neoplastic behaviour with potential of malignant transformation [5]. In the present case no recurrence was observed within one year of enucleation of lesion alongside preservation of premolar and molar. Tissue healing was adequate even without placement of bone graft.
Conclusion
The histopathological features of ameloblastic fibro-odontoma distinguish it from other mixed odontogenic tumors. AFO though considered a hamartoma requires a long term follow up for chances of recurrence.
Reference
1. Shafer WG, Hine MK, Levy BM. A Textbook of Oral Pathology. 8th Indian ed. Philadelphia, PA: Saunders. 2016: 116.
2. Tine SD et al. Report of a rare case of ameloblastic fibro-odontoma of the mandible with >400 odontomas and a related literature review. J of Oral Med and Oral Surgery. 2017. Volume 23, No.2: 99-102.
3. Lin YC, Hsu HM, Liu CS, Yuan K. A peripheral Ameloblastic Fibro-Odontoma in a 3-Year-Old Girl: Case Report, Immunohistochemical analysis, and Literature Review. Case Reports in Dentistry. 2014.
4. Silva GC Carvalho et al. Ameloblastic fibro-odontoma. Oral oncology extra. 2006; 42: 217-220.
5. Beena VT, Josh J, Paul S, Mathunny MS, Kottarathil SK, Shalu. Ameloblastic Fibro-odontoma. Oral Maxillofac Pathol J. 2017; 8(2): 94-97.
6. Philipsen HP, Reichart PA, Praetorius F. Mixed odontogenic tumors and odontomas. Considerations on interrelationship. Review of the literature and presentation of 134 new cases of odontomas. Oral Oncol. 1997; 33: 86-99.
7. Tekkesin M, Vered. Ameloblastic Fibro-Odontoma: At the Crossroad Between “Developing Odontoma” and True Odontogenic Tumour. Head Neck Pathol. 2021; 15(4): 1202-1211.
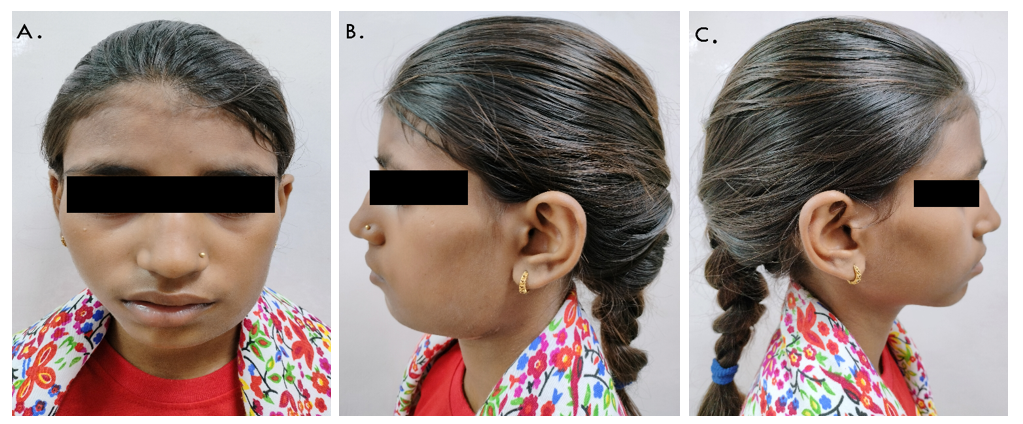
Figure 1
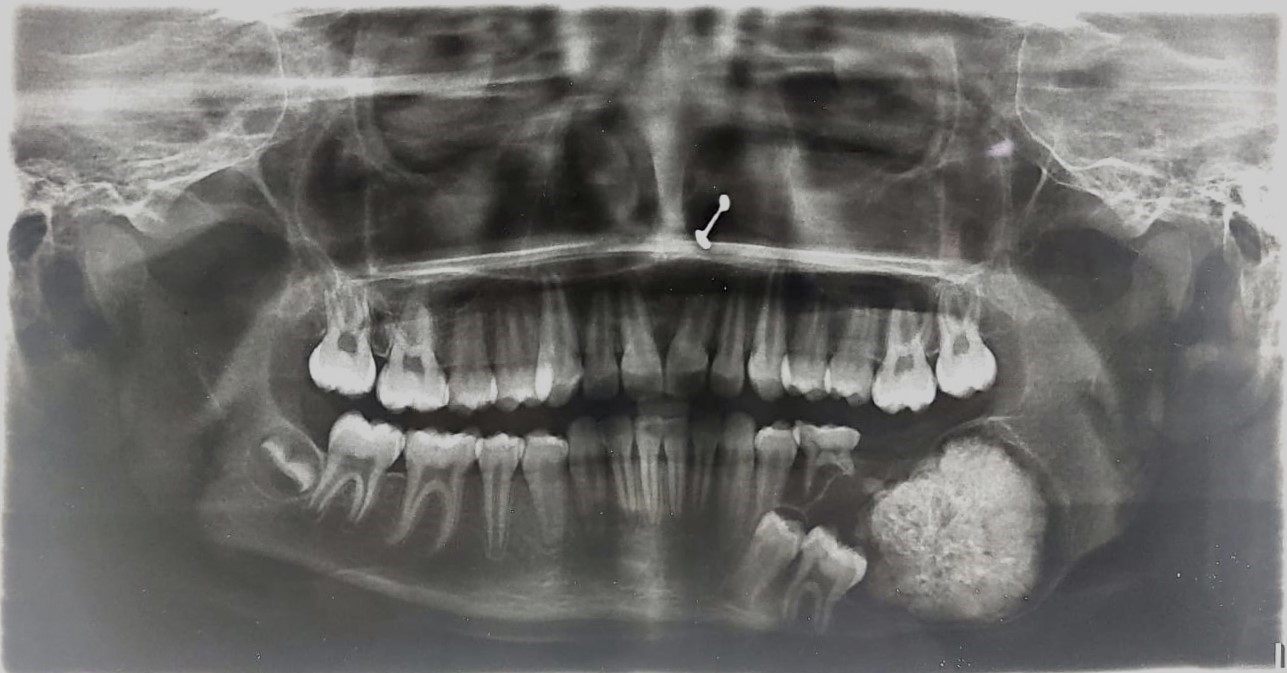
Figure 2
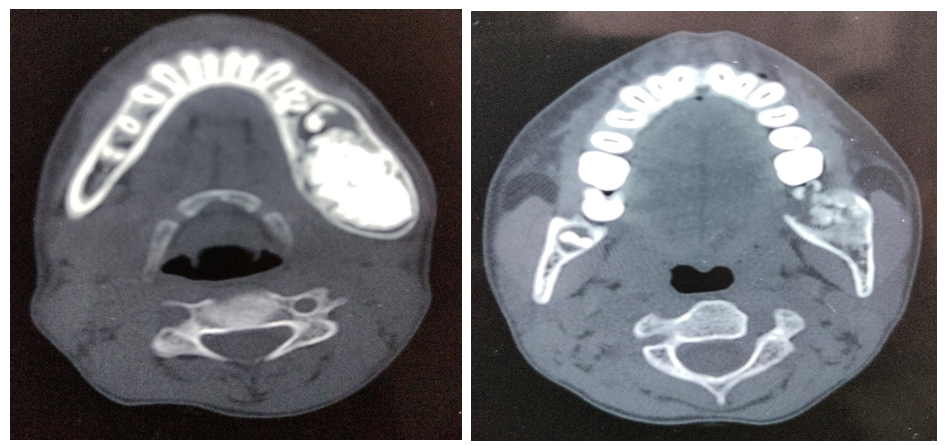
Figure 3
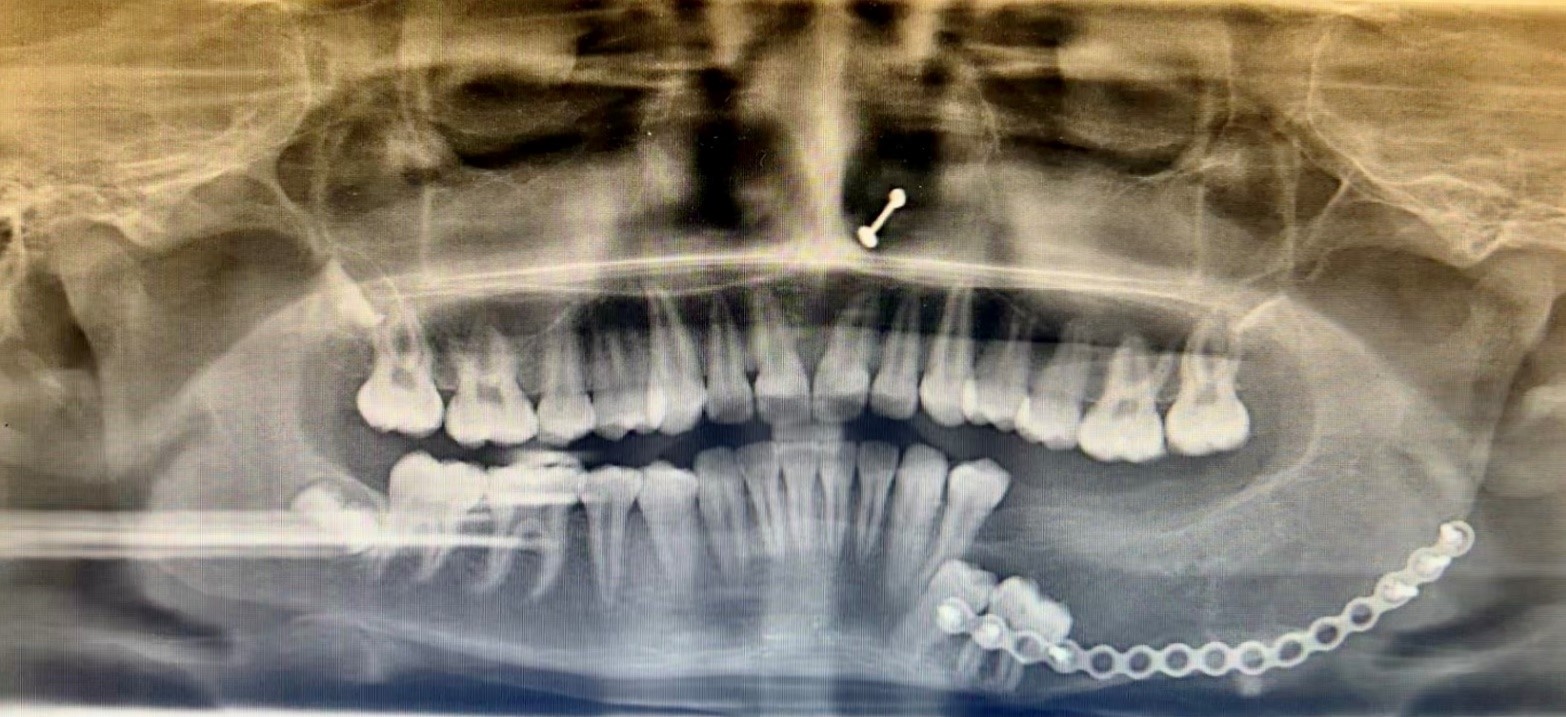
Figure 4
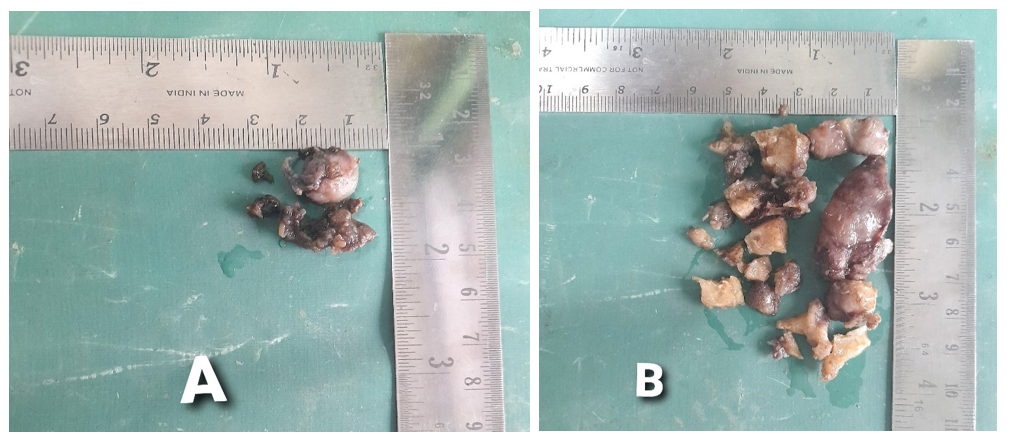
Figure 5
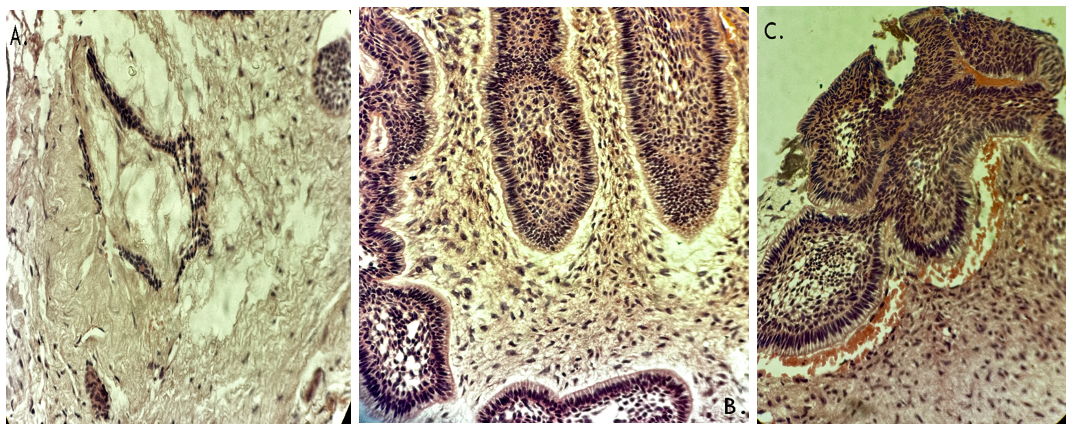
Figure 6
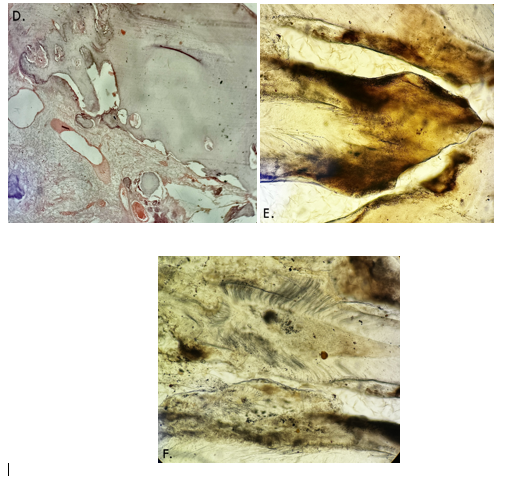
Figure 7