Hidden Identity: Unmasking Follicular Dendritic Cell Sarcoma Mimicking Squamous Cell Carcinoma
Hidden Identity: Unmasking Follicular Dendritic Cell Sarcoma Mimicking Squamous Cell Carcinoma
Fatima Shamsuddin *, George Smiley1, Dr. Nourah Alyouha2, Dr. Bader Alali3
1.Department of Histopathology, Jaber Al Ahmad Hospital, Kuwait.
2.Otolaryngology, Head and Neck surgery department, Jaber Al Ahmad hospital.
3.Otolaryngology, Head and Neck surgery department, Jaber Al Ahmad hospital
*Correspondence to: Fatima Shamsuddin, Department of Histopathology, Jaber Al Ahmad Hospital, Kuwait.
Copyright
© 2024 Fatima Shamsuddin. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 07 September 2024
Published: 20 September 2024
DOI: https://doi.org/10.5281/zenodo.13821579
Abstract
Background: We present the case of a 55-year-old male with progressive dysphagia and weight loss. CT neck revealed a large oropharyngeal lesion infiltrating the right tonsil, uvula, and soft palate. Initial biopsy and later excision specimens were examined.
Aims: To diagnose and understand the rare presentation of Follicular Dendritic Cell Sarcoma (FDCS) in the tonsils and emphasize the importance of considering FDCS in the differential diagnosis.
Materials and Methods: Biopsy and excision specimens were analysed for histopathological features. Immunohistochemistry was employed to confirm the diagnosis.
Results: Histopathology revealed ulcerated squamous epithelium overlaying a tumour with epithelioid and spindle-shaped cells, multinucleate forms, and extensive necrosis. Immunohistochemistry confirmed CD21 and CD23 positivity.
Conclusions: Our case underscores the need to consider rare entities like FDCS when encountering tonsillar neoplasms. Initial tests using epithelial markers were inconclusive, leading to the consideration of FDCS. Our findings contribute to the growing body of literature on extranodal FDCS and its diagnostic challenges.
Keywords: Follicular Dendritic Cell Sarcoma, Immunohistochemistry, Oropharyngeal lesion, Tonsillar neoplasm.
Hidden Identity: Unmasking Follicular Dendritic Cell Sarcoma Mimicking Squamous Cell Carcinoma
Introduction
Follicular dendritic cell sarcoma (FDCS) is an extremely rare and difficult-to-diagnose primary lymph node tumor that arises from follicular dendritic cells in lymph nodes. However, due to the presence of acquired lymphoid tissue, it can also be expressed in extranodal sites. The diagnosis of FDCS poses a major challenge for pathologists and hematopathologists, especially when it occurs outside the lymph nodes.
We draw on the results of few remarkable studies to shed light on this rare neoplasm.
In a report by Zhao et al., they presented two cases of extranodal FDCS, one involving the soft tissues of the chest wall and the other involving the right tonsil. Both patients underwent surgery with good postoperative results. A systematic review of the literature retrieved 102 cases of extranodal FDCS, with recurrence, metastasis, and mortality rates documented as 14.63%, 17.07%, and 8.29%, respectively.[1]
Another study by Duan et al reported pitfalls in the diagnosis of extranodal pharyngeal FDCS and highlighted that it is often misdiagnosed during initial evaluation, leading to suboptimal treatment. These challenges are further exacerbated by the striking similarity of FDCS to other neoplasms in histological and immunophenotypic features. [2]
Given the rarity and diagnostic difficulty of this tumor, it is essential to synthesize and critically evaluate the existing literature on FDCS to improve understanding and diagnosis. Furthermore, the results of related studies provide important information regarding the clinical behavior and prognostic factors of FDCS. [3,4]
Case Report
A 55-year-old male presented with a progressive onset of dysphagia and noticeable weight loss, prompting medical evaluation. A computed tomography (CT) scan of the neck was performed, revealing a substantial oropharyngeal lesion. On oral examination, the lesion demonstrated partial necrosis and displayed extensive infiltration, encompassing the right tonsil, uvula, soft palate, and abutting the dorsum of the tongue (Fig 1). Furthermore, the lesion extended below the epiglottis and posteriorly to involve the pre-vertebral muscle. Initial diagnostic procedures included a small biopsy, followed by the subsequent excision of the lesion. These specimens were submitted to the histopathology laboratory for comprehensive evaluation (Fig 2). Upon histopathological examination, the squamous epithelium covering the lesion appeared ulcerated and showed reactive changes (Fig 3). Beneath this epithelial layer, an underlying tumor was identified, arranged in nests and sheets.
The tumor cells exhibited distinctive characteristics, being oval to spindled in shape, with dispersed chromatin, small nucleoli, and moderate to abundant eosinophilic and fibrillar cytoplasm. Notably, many of these cells displayed multinucleate forms, and occasional nuclear pseudo inclusions were observed. The tumor nests were surrounded by an admixed population of lymphocytes, eosinophils, plasma cells, and neutrophils. Additionally, extensive areas of necrosis were evident. To further characterize the tumor and establish a precise diagnosis, immunohistochemistry (IHC) was performed. The results of the IHC analysis demonstrated that the tumor cells were positive for CD21 and CD23. Conversely, the tumor cells exhibited negative staining for pan CK, EMA, p63, Desmin, Myogenin, and S100. The IHC stain for P16 displayed a patchy positive pattern. Based on the comprehensive histopathological evaluation and the immunohistochemical profile, the tumor was conclusively diagnosed as Follicular Dendritic Cell Sarcoma (FDCS).
Fig 1. Oral examination revealed a large oropharyngeal lesion infiltrating the right tonsil,
uvula, and soft palate.
Fig 2. Macroscopy of tonsillar mass showing nodular tumor and serial slicing showed an ill-defined pale white lesion
Fig 3. Microscopy reveals A. Ulcerated squamous epithelium overlaying a tumor with syncytial sheets of cells (H&E, 4x) B. Epithelioid and spindle-shaped cells, multinucleate forms (H&E, 10x) C. CD21 positivity (H&E, 10x) D. CD23 positivity (H&E, 10x)
Discussion
The diagnosis and management of Follicular Dendritic Cell Sarcoma (FDCS) present significant challenges, particularly when it arises from extranodal sites. Extranodal FDCS can manifest in various locations, including the soft tissue of the chest wall, tonsils, nasopharynx, and gastrointestinal tract. Patients typically undergo surgical resection, and the post-operative outcomes appear favorable in many cases.[1]
The diagnostic journey for FDCS is complicated by its histological resemblance to other neoplasms. Duan et al. noted that FDCS of the pharyngeal region is often misdiagnosed upon initial evaluation, with cases resembling undifferentiated carcinoma or meningioma.[2] This diagnostic pitfall underscores the importance of accurate identification and the need for specialized expertise in distinguishing FDCS. Immunohistochemistry plays a crucial role in confirming the diagnosis, with specific markers like CD21, CD23, and CD35 proving essential for distinguishing FDCS from other tumors.[5]
Understanding prognostic factors is crucial for appropriate management. The prognosis of FDCS appears to vary based on location and subtype. A study by Gui et al. suggests two distinct subtypes of FDCS in the gastrointestinal tract, with differing clinical outcomes.[6] While some FDCS subtypes are low-grade and have relatively better survival rates, others may exhibit more aggressive behavior.
Although FDCS typically lacks distinctive genetic and molecular anomalies, some studies suggest the presence of clonal karyotype and chromosomal structural alterations. Exploring the molecular drivers of this neoplasm may hold promise for potential new therapeutic strategies.
FDCS often lacks mutations in genes related to the MAPK pathway, making it distinct from other histiocytic and dendritic cell tumors. Specialized immunohistochemical markers, such as clusterin, CXCL13, and podoplanin prove valuable in confirming the diagnosis.[7]
Complete surgical excision remains the gold standard for FDCS treatment. However, data on targeted therapies and immune checkpoint inhibitors are limited, with variable responses.[8] As research advances and molecular drivers are better understood, potential therapeutic strategies may emerge.
Conclusion
In conclusion, FDCS is an exceedingly rare and diagnostically challenging tumour that can affect various anatomical sites. Accurate diagnosis, aided by immunohistochemical markers, is crucial for effective management. Prognosis varies based on subtype and location. The field of FDCS research is evolving, and further exploration of its molecular drivers may open avenues for novel therapeutic approaches. As the literature on FDCS continues to expand, multidisciplinary collaboration among pathologists, hematopathologists, and oncologists is essential for improving the understanding and management of this unique neoplasm.
References
1. Zhao X, Sun D, Zhang G. Clinicopathological characteristics of extranodal follicular dendritic cell sarcoma: A report of two cases. Oncol Lett. 2021 Mar;21(3):182. doi: 10.3892/ol.2021.12443. Epub 2021 Jan 6. PMID: 33574921; PMCID: PMC7816366.
2. Duan GJ, Wu F, Zhu J, Guo DY, Zhang R, Shen LL, Wang SH, Li Q, Xiao HL, Mou JH, Yan XC. Extranodal follicular dendritic cell sarcoma of the pharyngeal region: a potential diagnostic pitfall, with literature review. Am J Clin Pathol. 2010 Jan;133(1):49-58. doi: 10.1309/AJCP7U8YISBUAVNW. PMID: 20023258.
3. Wu A, Pullarkat S. Follicular Dendritic Cell Sarcoma. Arch Pathol Lab Med. 2016 Feb;140(2):186-90. doi: 10.5858/arpa.2014-0374-RS. PMID: 26910224.
4. Bao L, Wang T, Liu M, Xing F. Follicular dendritic cell sarcoma of the tonsil: case report and review of literature. Int J Clin Exp Pathol. 2021 Apr 15;14(4):493-500. PMID: 33936372; PMCID: PMC8085827.
5. Facchetti F, Simbeni M, Lorenzi L. Follicular dendritic cell sarcoma. Pathologica. 2021 Oct;113(5):316-329. doi: 10.32074/1591-951X-331. PMID: 34837090; PMCID: PMC8720404.
6. Gui H, Chaudhari J, Mannan R. Follicular dendritic cell sarcoma of gastrointestinal tract with two emerging distinct subtypes: a case report and systemic review. Diagn Pathol. 2022 Aug 8;17(1):64. doi: 10.1186/s13000-022-01246-z. PMID: 35941667; PMCID: PMC9358870.
7. Idrees MT, Brandwein-Gensler M, Strauchen JA, Gil J, Wang BY. Extranodal follicular dendritic cell tumor of the tonsil: report of a diagnostic pitfall and literature review. Arch Otolaryngol Head Neck Surg. 2004 Sep;130(9):1109-13. doi: 10.1001/archotol.130.9.1109. PMID: 15381600.
8. Satoh K, Hibi G, Yamamoto Y, Urano M, Kuroda M, Nakamura S. Follicular dendritic cell tumor in the oro-pharyngeal region: report of a case and a review of the literature. Oral Oncol. 2003 Jun;39(4):415-9. doi: 10.1016/s1368-8375(02)00138-0. PMID: 12676264.

Figure 1

Figure 2
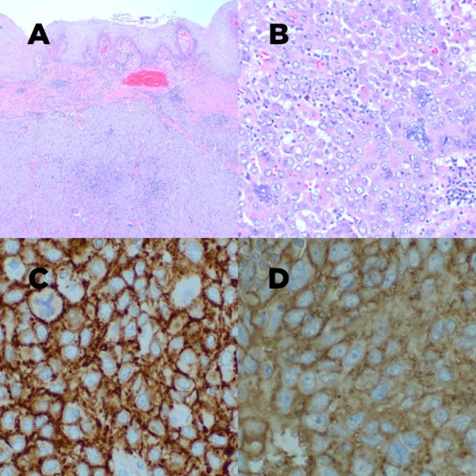
Figure 3