Unilateral Fetal Hydroceles in Utero
Unilateral Fetal Hydroceles in Utero
Chebil Aicha1, Montacer Hafsi*2. Marzouk Khouloud3, Nouiji Sabrine4, Baccouche Fedia5, Bouchahda Haifa6
1,2,3,4,5,6. Université de Monastir, Service de gynécologie obstétrique, CHU Taher Sfar Mahdia.
*Correspondence to: Montacer Hafsi, Université de Monastir, Service de gynécologie obstétrique, CHU Taher Sfar Mahdia.
Copyright
© 2024 Montacer Hafsi. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 09 October 2024
Published: 23 October 2024
Abstract
Fetal hydrocele is a condition in which fluid accumulates in the scrotum of male fetuses. It is often identified through ultrasound during pregnancy and is relatively common, especially in the third trimester.Through a clinical case, we illustrate the characteristic ultrasound imaging of fetal hydroceles and their intrascrotal content.
Keywords: fetal hydrocele, ultrasound imaging.
Unilateral Fetal Hydroceles in Utero
Introduction
The prevalence of fetal hydrocele is relatively common. In the majority of cases, this condition is benign and tends to disappear spontaneously in the months following birth. Fetal ultrasound is a key examination for prenatal diagnosis.
Materials and Methods
We report the case of a 34-year-old female patient, G2P2, admitted for term delivery at 39 weeks of gestation. Ultrasound revealed an unusual cystic structure at the lower end of the fetal trunk (Fig. 1), suggesting an enlarged scrotal sac consistent with a unilateral hydrocele. The presence of intrascrotal testes and an epididymis surrounded by hydrocele fluid was noted. The fetal hydrocele was confirmed at birth (Fig. 2).
Fig1, Fig2
Discussion
Ultrasonography is an effective tool for diagnosing fetal anomalies, including reported cases of prenatal urologic abnormalities. Advances in gray-scale imaging have greatly enhanced the accuracy of identifying normal fetal anatomy and genitalia(1).
Fetal hydroceles are often unilateral, meaning they typically occur on one side, although bilateral cases can also be observed(2).The presence of a hydrocele is generally considered a normal physiological phenomenon, particularly in the absence of other abnormalities(2).
A hydrocele is the abnormal accumulation of serous fluid between the two layers of the tunica vaginalis surrounding the testis. It can be either congenital or acquired. Congenital hydrocele occurs when the processus vaginalis fails to close. During development, the testes form retroperitoneally in the abdomen and descend into the scrotum through the inguinal canal by the third gestational week. This descent is accompanied by a fold of the peritoneum, the processus vaginalis. Normally, the upper part of the processus vaginalis closes, while the lower part persists as the tunica vaginalis, covering the anterior, lateral, and medial sides of the testes. If the upper part remains open, fluid from the peritoneal cavity can accumulate in the tunica vaginalis, leading to congenital hydrocele.
Hydroceles are classified into two types: primary and secondary(3).Primary hydrocele occurs when, during normal development, the processus vaginalis closes at birth or within the first 1-2 years of life, severing the connection between the abdomen and the scrotum. However, the distal portion persists as the tunica vaginalis, leaving a potential space where fluid can accumulate, leading to the formation of a hydrocele. The condition is categorized into four types, depending on the location of the failure in the closure of the processus vaginalis.
Secondary hydrocele develops as a result of underlying conditions such as infections (e.g., filariasis, tuberculosis of the epididymis, syphilis), injury (e.g., trauma or post-surgical complications), or malignancy. These hydroceles are generally small, except in cases of filariasis, where the hydrocele can become considerably larger.
Fetal hydrocele is typically diagnosed by prenatal ultrasound. The main ultrasound findings are: Anechoic fluid effusion around the testicle, often unilateral, Normal testicle in size and echostructure, pushed to the bottom of the scrotum, Absence of intra-fluid vascularization on Doppler(1).In some cases, fetal MRI may also be utilized, showing a hyperintense fluid layer around the scrotum(4).
Management depends on the size of the hydrocele and its evolution during pregnancy. Close ultrasound monitoring is necessary. In the case of a very large hydrocele, an in utero puncture may be discussed to prevent complications such as testicular torsion. After birth, most hydroceles regress spontaneously within the first 2 years of life. Surgery is rarely necessary, except in cases of persistence beyond 2 years or recurrence.
Conclusion
Ultrasound is the key examination for diagnosing a fetal hydrocele, allowing its severity to be assessed and for guiding management. Ultrasound monitoring is essential during pregnancy and after birth.
References
1 DiGiacinto TM, Willscher MK, Conway JC. Bilateral fetal hydroceles in utero. Urology. mai 1980;15(5):532?3.
2. Hydroceles identified prenatally: common physiologic phenomenon? - Pretorius - 1998 - Journal of Ultrasound in Medicine - Wiley Online Library [Internet]. [cité 14 sept 2024]. Disponible sur: https://onlinelibrary.wiley.com/doi/abs/10.7863/jum.1998.17.1.49
3. Huzaifa M, Moreno MA. Hydrocele. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 [cité 14 sept 2024]. Disponible sur: http://www.ncbi.nlm.nih.gov/books/NBK559125/
4. Weerakkody Y. Radiopaedia. [cité 14 sept 2024]. Fetal hydrocele | Radiology Reference Article | Radiopaedia.org. Disponible sur: https://radiopaedia.org/articles/fetal-hydrocele-1.
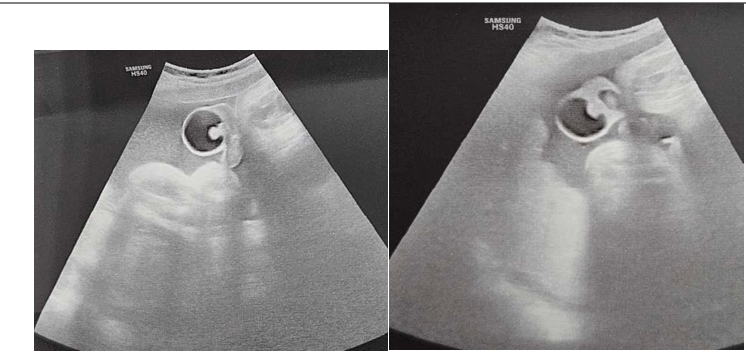
Figure 1

Figure 2