Comparing Computer Navigation with a Simple Manual Measurement Device in Measuring Leg Length in Total Hip Arthroplasty
Comparing Computer Navigation with a Simple Manual Measurement Device in Measuring Leg Length in Total Hip Arthroplasty
Haytham Al Husari1*, Dr Kassem El Houcheimi 2
Dr Kassem El Houcheimi, FACS, MBA, Orthopedic surgeon, Clemenceau Medical Center Dubai.
*Correspondence to: H Haytham Al Husari, MD, DFMSA, Lower Limb Arthroplasty and Sports Fellowship Orthopaedic Trauma Fellowship, University Diploma in Arthroscopy and Microsurgery.
Copyright
© 2024 Haytham Al Husari. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 01 Nov 2024
Published: 15 Nov 2024
DOI: https://doi.org/10.5281/zenodo.14168622
Abstract:
This study aimed to determine if computer navigation can improve postoperative leg length discrepancy (LLD) in total hip arthroplasty (THA) compared to manual intra-operative measurement devices. A retrospective study compared 30 computer-assisted THAs with 40 THAs performed using a simple manual measurement device. Results showed that the computer-assisted group had a 3.0 mm postoperative LLD, while the device group had a 2.9 mm LLD. No statistically significant difference was found between the two groups. The results showed good equalization of leg lengths using both computed tomography-based navigation and a simple manual measurement device.
Keywords: Total hip arthroplasty, Leg length discrepancy, Computed tomography-based navigation, Device
Comparing Computer Navigation with a Simple Manual Measurement Device in Measuring Leg Length in Total Hip Arthroplasty
Introduction
The measurement of leg length discrepancy (LLD) is crucial for planning a successful total hip arthroplasty (THA). Various methods have been proposed to assess LLD and femoral offset restoration, including Steinmann pins, K-wires, and proprietary devices. A simple manual measurement device, the PCA limb lengthening gauge, has been used for intraoperative leg length measurement. The mean error for this device was 2.1 mm, with an average postoperative LLD of 3.1 mm. Other studies have shown that the mean LLD with published techniques ranged from 0.3 to 9.0 mm, with a total range of –22 to +35 mm.
However, the use of computer navigation in arthroplasty has increased over the last decade, with studies comparing CT-based and imageless navigation systems with freehand methods. These studies have shown a higher percentage of acetabular cups implanted within the safe zone compared to freehand implantation. However, no study has reported on any clinical advantages of using navigation compared to intraoperative measurement devices. A retrospective study comparing 30 computer-assisted THAs with 40 THAs performed using a simple manual measurement device system aims to determine if computer navigation in THA could achieve better results in terms of postoperative LLD than a simple measurement device.
Fig 1
PCA limb lengthening gauge. The left pin goes into the acetabulum,and the right pin into the femur. A stopper and a thread cutting are added to the pin for the acetabulum.
Fig 2
Methods
The study involved 85 patients who underwent a unilateral primary total hip arthroplasty (THA) between August 2002 and July 2007. The patients were divided into two groups: those who underwent a computer-assisted THA using a CT-based navigation system, and those who underwent a THA using a previously studied gauge. The mean age at the time of the operation was 63 years in the computer-assisted group and 62 years in the device group.
The preoperative diagnosis was osteoarthritis (OA) in 58 hips, osteonecrosis of the femoral head in 7 hips, and rheumatoid arthritis (RA) in 5 hips. All operations were performed by a single surgeon through the posterolateral approach, with patients in the lateral decubitus position under general anesthesia. The postoperative leg length was determined in preoperative planning, with the objective being to have no LLD after THA.
In the computer-assisted group, the anterior pelvic plane was identified with a tracker fixed with two 4.0 threaded pins on the same side as the anterior superior iliac spine. Following the dislocation of the hip joint, a femoral tracker was fixed on the distal femur with two more 4.0 threaded pins to determine the leg length. The pelvis and femur were registered by surface matching and digitizing over 30 points with a pointer, respectively.
In the device group, the leg-length was assessed using the PCA limb lengthening gauge, which is composed of 2 pins and a gauge. The distance between the pins was recorded three times during the surgery: before the dislocation, after inserting the trial components, and after setting the real prosthesis. The difference between the length before the femoral head dislocation and the length after setting the real prosthesis was determined as the intraoperative leg-lengthening.
Fig 3: The lengthening axis is marked and the device is placed and showing the location of the device.
Preoperative and postoperative LLD measurements were made using radiographs, with the anteroposterior radiographs obtained preoperatively and postoperatively in a standardized fashion with both hips extended and internally rotated. The Pearson coefficient of correlation was evaluated between the two values.
Results
The study found no significant differences in patient demographics or preoperative leg lengthening (LLD) between two groups. The mean preoperative LLD on radiographs was 10.0 mm in the computer-assisted group and 9.8 mm in the device group. The mean radiographic measurements on leg lengthening were 12.0 mm in the computer-assisted group and 9.7 mm in the device group. The mean errors between radiographic and intraoperative measurements were 2.4 mm and 2.1 mm, respectively. Postoperative LLD was 3.0 mm in the computer-assisted group and 2.9 mm in the device group. Statistically significant differences in postoperative LLD and measurement error were not seen between the two groups. Two patients had a post-operative LLD of 6 mm or greater in the computer-assisted group compared to seven patients in the device group. All patients in this group had recognized the loosening of the pins with osteoporotic bones during surgery. No intraoperative complications were encountered in either group.
Fig 4
Discussion
Leg length equality is a crucial factor in successful Total Hip Anterior (THA) surgery, as it can lead to hip instability, ipsilateral knee pain, low back pain, sciatic nerve palsy, and aseptic prosthesis loosening. Postoperative LLD can result in revision surgeries and even litigation. To avoid this, several techniques have been proposed to assess leg length intraoperatively, such as the use of an 'L' shaped caliper, carpenter's or dual pin calipers, and direct measurement with a ruler.
The PCA limb lengthening gauge provides equivalent or even more precise data on postoperative leg-length compared to devices introduced in these reports. However, the disadvantage of this device is loosening of the pins in patients with osteoporotic bones, as the pin on the femur is removed during surgery, causing it to become easily loosened. Inaccurate abduction/adduction repositioning of the femur with respect to the pelvis also can cause substantial error in the measurement of the length and can offset changes.
Computer navigation systems have been developed for more precise surgery, with studies showing that better placement of the acetabular cup and femoral stem can be achieved in THA using either a CT-based or image-free computer navigation system than using free-hand alignment methods. The authors of many of these studies suggest that the technological advances now available could result in more accurate implant alignment, translating into better stability, performance, and survivorship.
The range of LLD cases in which such a navigation system has been used is well reported in the literature. Manzotti et al. used image-free navigation and reported that the postoperative LLD was 5.06 ±2.99 mm and the LLD was within 12 mm in all of their patients. Murphy and Ecker used CT-based navigation and reported that postoperative LLD and measurement errors were 6.1 ± 4.3 mm (range, –5 to 20 mm) and –0.5 ± 1.77 mm (range, –5 to 3.9 mm), respectively.
This study showed reasonable and equivalent results compared to previous reports and showed that CT-based navigation is reliable for leg length adjustment. However, there is no literature demonstrating any relevant clinical advantages of using navigation compared to manual intraoperative measurement devices. The study shows quite acceptable equalization of the leg-length after THA, using both computer navigation and a simple manual device.
However, the study has some limitations. First, postoperative evaluation was based on plain pelvic radiographs instead of CT scans, which have been used in other studies to eliminate variables of pelvic tilt. Various authors have pointed out that linear measurements and calculations from plain X-rays are susceptible to error due to variations in positioning of the pelvis relative to the plane of the film and the divergence of the X-ray beams.
Since this was a retrospective analysis, the patients were not randomized and follow-ups were too short to detect differences in clinical outcomes. Further accumulation of cases will be needed. Based on the number of outliers (> 6 mm LLD), it appears that the computer-assisted group may present an advantage when the number of cases is increased.
References
1. Hofmann AA, Bolognesi M, Lahav A, Kurtin S. Minimizing leg-length inequality in total hip arthroplasty: use of preoperative templating and an intraoperative x-ray. Am J Orthop (Belle Mead NJ). 2008;37(1):18-23.
2. White TO, Dougall TW. Arthroplasty of the hip: leg length is not important. J Bone Joint Surg Br. 2002;84(3):335-8.
3. Konyves A, Bannister GC. The importance of leg length discrepancy after total hip arthroplasty. J Bone Joint Surg Br. 2005;87(2):155-7.
4. Jasty M, Webster W, Harris W. Management of limb length inequality during total hip replacement. Clin Orthop RelatRes. 1996;(333):165-71.
5. Sugano N, Nishii T, Miki H, Yoshikawa H, Sato Y, Tamura S. Mid-term results of cementless total hip replacement using a ceramic-on-ceramic bearing with and without computer navigation. J Bone Joint Surg Br. 2007;89(4):455-60.
6. Ybinger T, Kumpan W, Hoffart HE, Muschalik B, Bullmann W, Zweymuller K. Accuracy of navigation-assisted acetabular component positioning studied by computed tomography measurements: methods and results. J Arthroplasty. 2007;22(6):812-7.
7. Langlotz U, Grutzner PA, Bernsmann K, et al. Accuracy considerations in navigated cup placement for total hip arthroplasty. Proc Inst Mech Eng H. 2007;221(7):739-53.
8. Manzotti A, Cerveri P, De Momi E, Pullen C, Confalonieri N. Does computer-assisted surgery benefit leg length restoration in total hip replacement? Navigation versus conventional freehand. Int Orthop. 2011;35(1):19-24.
9. Schmerwitz U. Total hip arthroplasty: first experiences with pinless THA software to determine leg length and offset. Orthopedics. 2007;30(10 Suppl):S124-6.
10. Murphy SB, Ecker TM. Evaluation of a new leg length measurement algorithm in hip arthroplasty. Clin Orthop Relat Res. 2007;463:85-9.
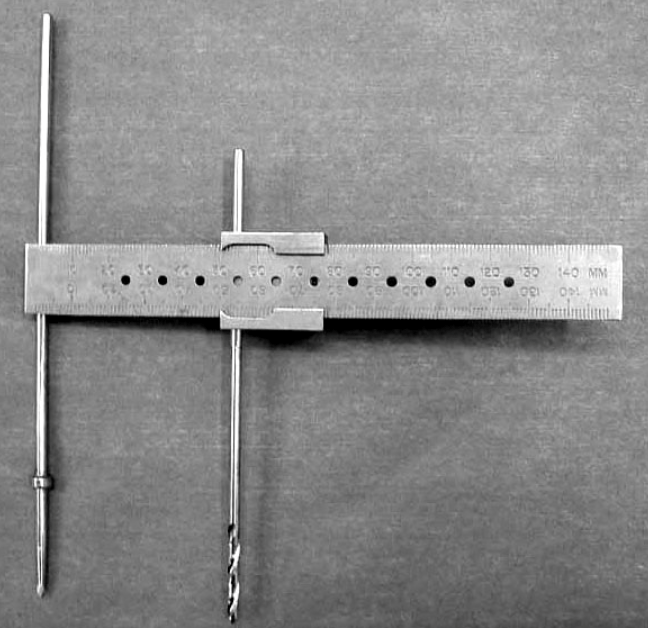
Figure 1
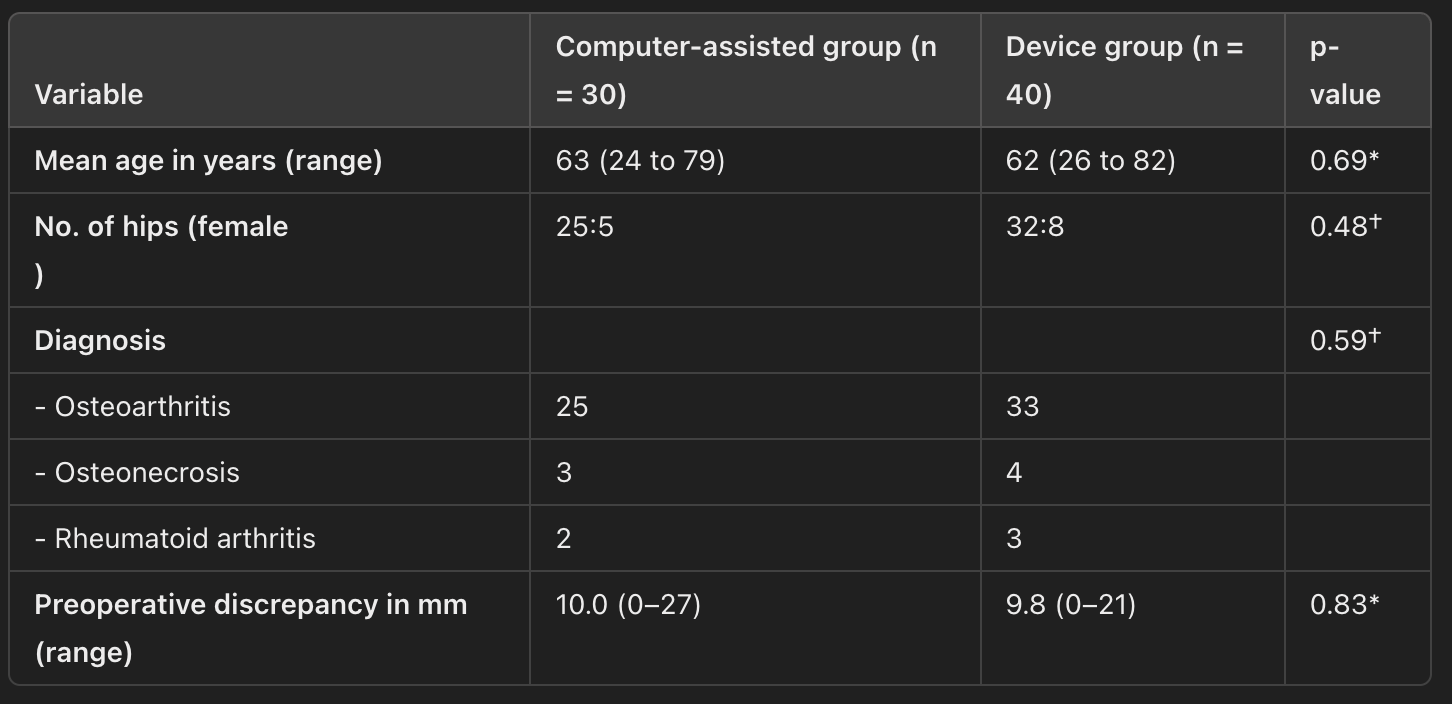
Figure 2

Figure 3
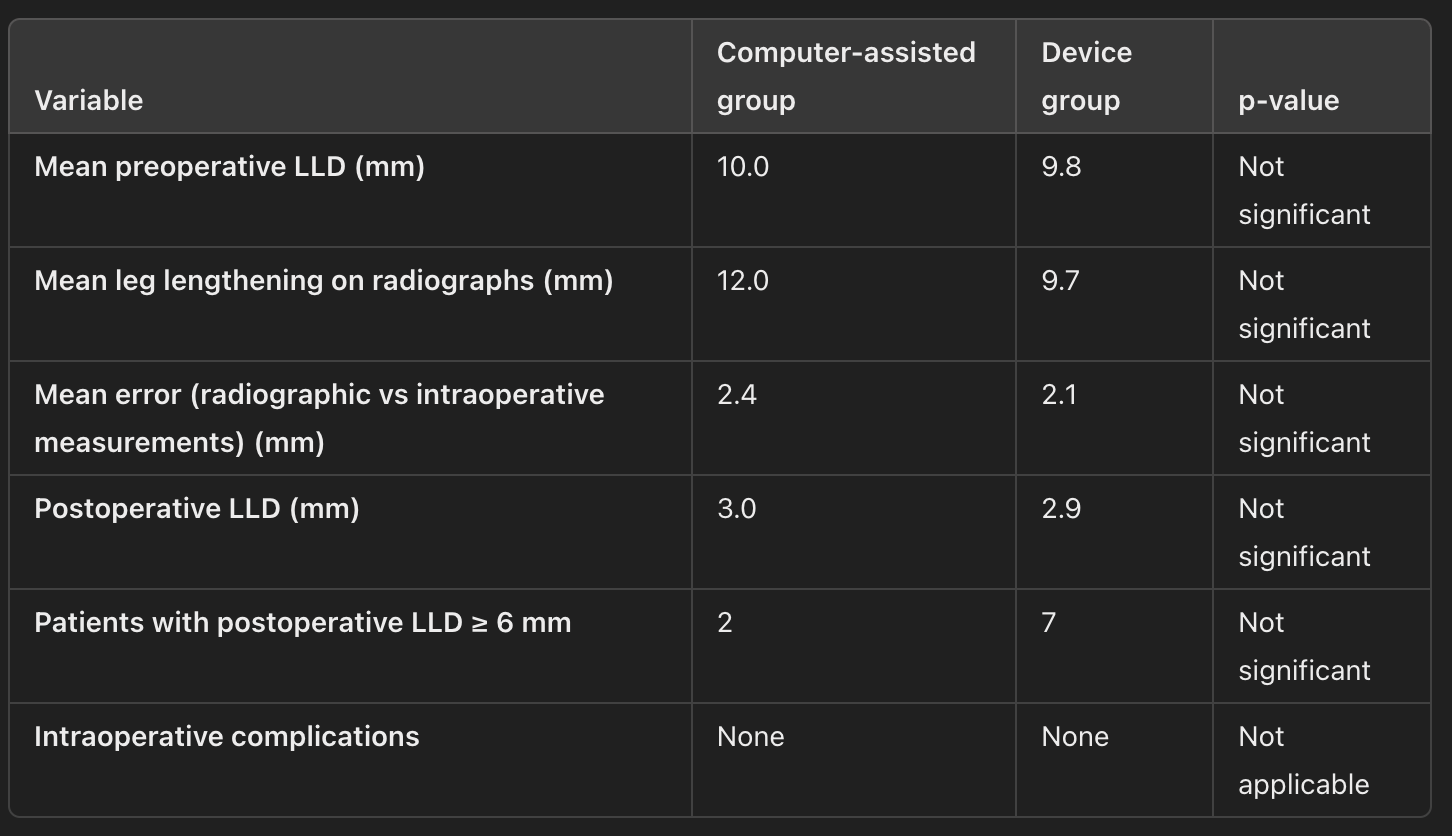
Figure 4