Aortic Valve Myxoma: A Rare Case Report.
Aortic Valve Myxoma: A Rare Case Report.
Dr. Aamir MD *
*Correspondence to: Dr Aamir MD, Associate Clinical Cardiologist, Hyderabad, India.
Copyright
© 2024 Dr Aamir MD. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 14 Dec 2024
Published: 19 Dec 2024
Abstract
A 47-year-old woman with a history of antiphospholipid syndrome presented with recurrent strokes. Imaging studies, including echocardiogram and cardiac MRI, revealed an unusual case of aortic valve myxoma with associated thrombus formation, contributing to recurrent cerebrovascular events. She underwent successful surgical replacement of the aortic valve with a mechanical prosthesis and was anticoagulated with warfarin, with the target INR set to 3–4.
Aortic Valve Myxoma: A Rare Case Report.
Introduction
Primary cardiac tumors are exceedingly rare, with an incidence rate of approximately 0.02% in the general population. Among these, atrial myxomas are the most frequently encountered, while aortic valve myxomas represent an extremely uncommon subset. Myxomas are benign neoplasms of mesenchymal origin, typically arising from the atrial septum, with only a handful of cases involving the aortic valve reported in medical literature.
Aortic valve myxomas can have significant clinical implications due to their potential to cause valve dysfunction, obstruction, and systemic embolization. The embolic events, often resulting from either tumor fragments or thrombus formation on the tumor surface, can lead to life-threatening complications, such as strokes, transient ischemic attacks (TIAs), and myocardial infarctions. These manifestations often mimic other conditions, making timely and accurate diagnosis challenging.
Case Presentation
Patient History
A 47-year-old woman presented with an acute ischemic stroke. Her medical history included:
- Antiphospholipid syndrome
- A previous stroke
- Recurrent transient ischemic attacks (TIAs)
The patient had been anticoagulated with warfarin and apixaban for the past two years without resolution of her cerebrovascular events.
Initial Workup
Echocardiography
A transthoracic echocardiogram, conducted as part of her routine stroke workup, revealed:
- A large aortic valve mass
- Moderate eccentric aortic regurgitation
- Absence of left ventricular outflow tract (LVOT) obstruction
Cardiac MRI Findings
Cardiac MRI identified a 1.2 cm × 2 cm hypodense lesion attached predominantly to the left coronary cusp of the aortic valve, extending into the LVOT. Additional findings included:
- A trileaflet aortic valve with incomplete coaptation
- Moderate aortic regurgitation
- Normal left ventricular (LV) function
- Moderate concentric LV hypertrophy
- An akinetic apex with evidence of focal transmural infarction extending into the apical septum
The characteristics of the lesion suggested it was more consistent with a thrombus.
Cardiac CT Findings
Cardiac CT confirmed:
- A 1.6 cm × 1.19 cm aortic valve mass between the left and right coronary cusps, extending into the LVOT
- A normal aortic root and ascending aorta
- A pedunculated lesion within the descending aorta, measuring 1.4 cm × 1.2 cm × 4 cm
Diagnosis and Management
Differential Diagnosis
Based on imaging and clinical findings, the differential diagnosis included:
1.Thrombus
2.Myxoma
3.Fibroelastoma
Surgical Intervention
After discussion in a multidisciplinary cardiac team meeting, the decision was made to surgically replace the aortic valve.
- The aortic valve was excised and replaced with a 21 mm On-X mechanical prosthesis.
- Histological analysis confirmed the diagnosis of an aortic valve myxoma with thrombus formation.
Anticoagulation Strategy
Given the patient’s antiphospholipid syndrome and history of recurrent strokes and TIAs, apixaban was deemed unsuitable. Warfarin therapy was initiated with a target INR of 3–4, following European Society of Cardiology (ESC) guidelines for mechanical valves with additional risk factors.
Outcome and Follow-Up
The patient recovered well postoperatively. At her 6-week follow-up, she reported no symptoms or concerns.
Figure 1
Figure 2
Figure 3
Discussion
This case underscores the importance of considering rare cardiac tumors like aortic valve myxoma in patients with unexplained recurrent embolic events, especially in the context of thrombogenic conditions like antiphospholipid syndrome. The thrombus formation within the myxoma likely contributed to her recurrent strokes and myocardial infarction, as evidenced by the findings on cardiac MRI.
Surgical resection of the mass with valve replacement remains the cornerstone of treatment, particularly when valve dysfunction is present. Long-term anticoagulation is critical to prevent further thromboembolic events in patients with mechanical valves and high-risk conditions.
Conclusion
This case highlights the rare occurrence of an aortic valve myxoma, a condition that is scarcely reported in the literature but carries significant clinical implications. The patient’s presentation with recurrent strokes and a history of antiphospholipid syndrome underscores the complex interplay between a hypercoagulable state and the embolic potential of cardiac tumors. Advanced imaging modalities, including echocardiography, cardiac MRI, and CT, played a crucial role in diagnosing the lesion and guiding management. The successful surgical excision of the myxoma, along with the replacement of the aortic valve, underscores the importance of a multidisciplinary approach in such challenging cases. Postoperative management with appropriate anticoagulation using warfarin, tailored to a higher target INR of 3–4 in accordance with European Society of Cardiology guidelines, was essential in minimizing the risk of further thromboembolic events. This case serves as a reminder of the importance of considering rare cardiac tumors in patients with recurrent cerebrovascular events, particularly in the presence of hypercoagulable conditions, and highlights the necessity of timely surgical intervention to improve patient outcomes.
Reference
1. Reynen, K. (1995). Cardiac Myxomas. New England Journal of Medicine, 333(24), 1610–1617. https://doi.org/10.1056/NEJM199512143332407
2. Pinede, L., Duhaut, P., & Loire, R. (2001). Clinical presentation of left atrial cardiac myxoma: a series of 112 consecutive cases. Medicine (Baltimore), 80(3), 159–172. https://doi.org/10.1097/00005792-200105000-00002
3. Keeling, I. M., Oberwalder, P., Anelli-Monti, M., et al. (2002). Cardiac myxomas: 24 years of experience in 49 patients. European Journal of Cardio-Thoracic Surgery, 22(6), 971–977. https://doi.org/10.1016/S1010-7940(02)00557-2
4. Habib, G., Bucciarelli-Ducci, C., Caforio, A. L., et al. (2021). Multimodality imaging in restrictive cardiomyopathies: An ESC guideline update. European Heart Journal – Cardiovascular Imaging, 22(1), 1–15. https://doi.org/10.1093/ehjci/jeaa317
5. Ott, D. A., & Cooley, D. A. (1984). Cardiovascular myxomas. Current Problems in Cardiology, 9(1), 1–41. https://doi.org/10.1016/0146-2806(84)90002-5
6. Katsi, V., Skevofilakas, K., Soulaidopoulos, S., et al. (2022). Management of Antiphospholipid Syndrome and Associated Complications. Frontiers in Medicine, 9, 798292. https://doi.org/10.3389/fmed.2022.798292
7. Wada, Y., Kitahara, H., & Tanaka, S. (2019). Aortic valve myxoma: A rare cause of embolic stroke. Journal of Cardiology Cases, 20(6), 204–206. https://doi.org/10.1016/j.jccase.2019.08.003
8. Baumgartner, H., Falk, V., Bax, J. J., et al. (2017). 2017 ESC/EACTS Guidelines for the management of valvular heart disease. European Heart Journal, 38(36), 2739–2791. https://doi.org/10.1093/eurheartj/ehx391
9. Li, D., & Wu, X. (2019). Surgical treatment of cardiac myxomas: A retrospective study of 40 cases. Heart Surgery Forum, 22(4), E259–E264. https://doi.org/10.1532/hsf.2385
10. Tascón, G., & Palomares, R. A. (2021). Cardiovascular Thromboembolic Risk in Antiphospholipid Syndrome. Circulation Research, 128(4), 576–591. https://doi.org/10.1161/CIRCRESAHA.120.318153
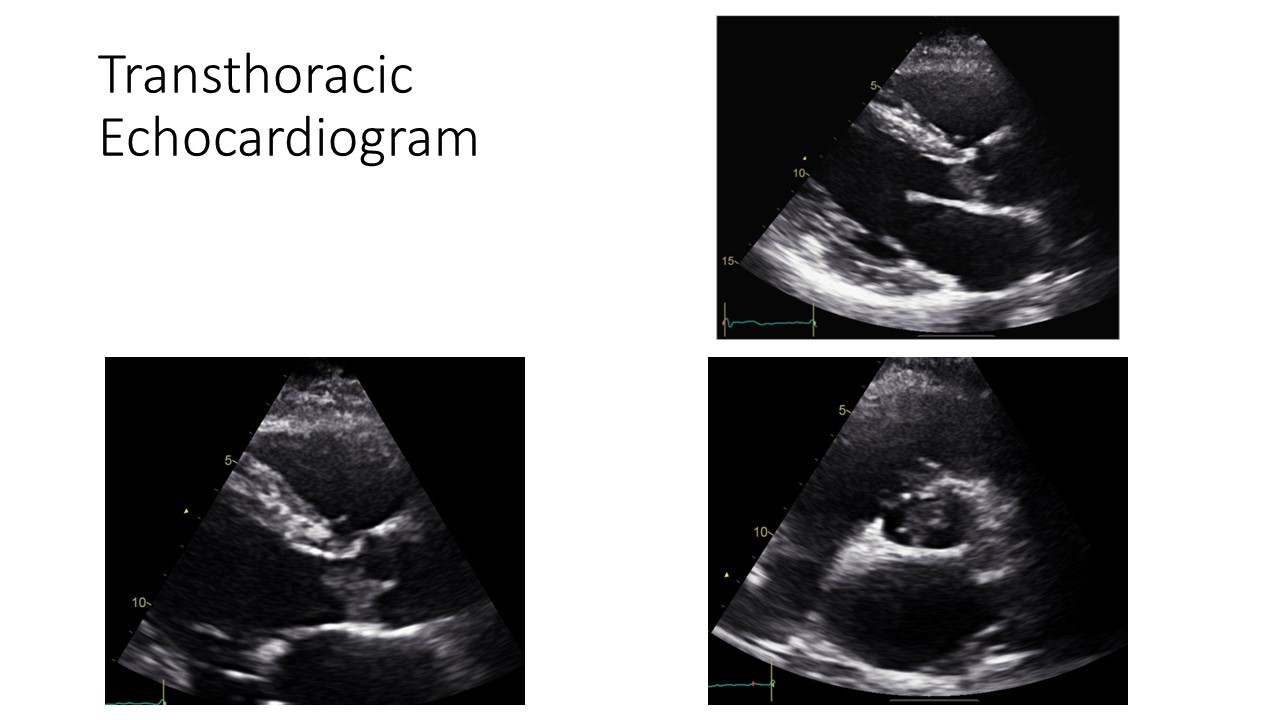
Figure 1
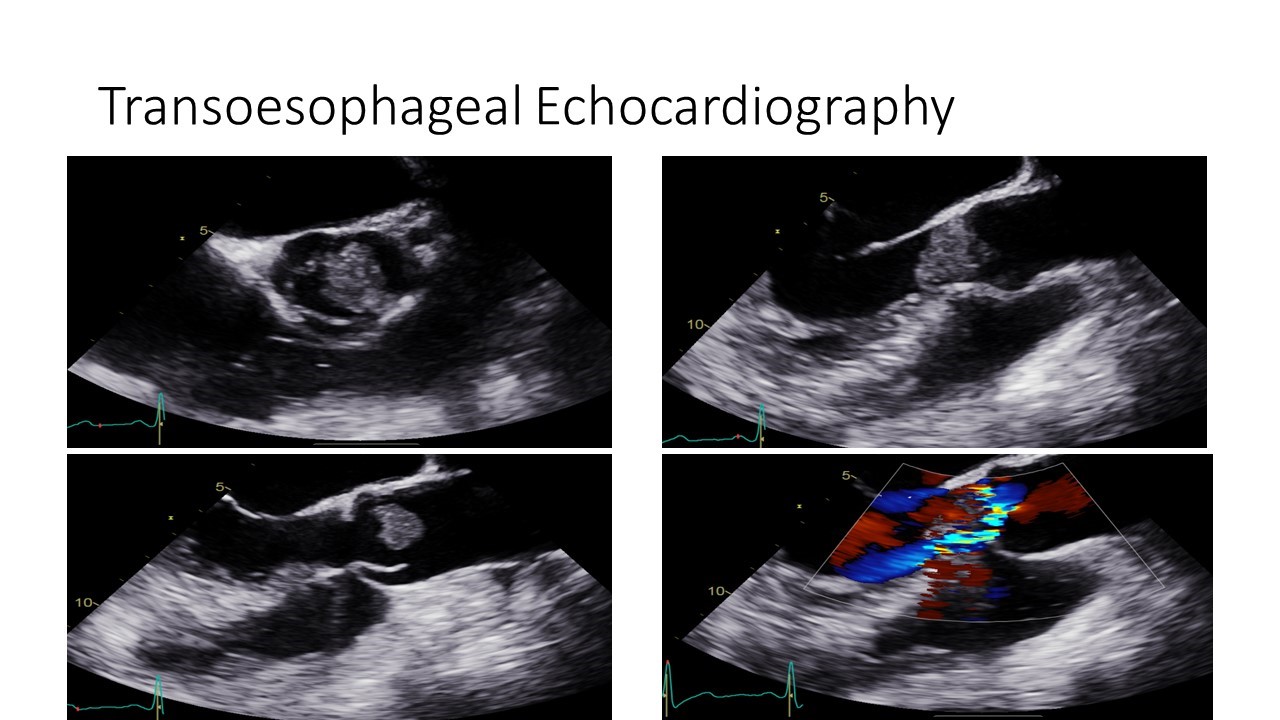
Figure 2
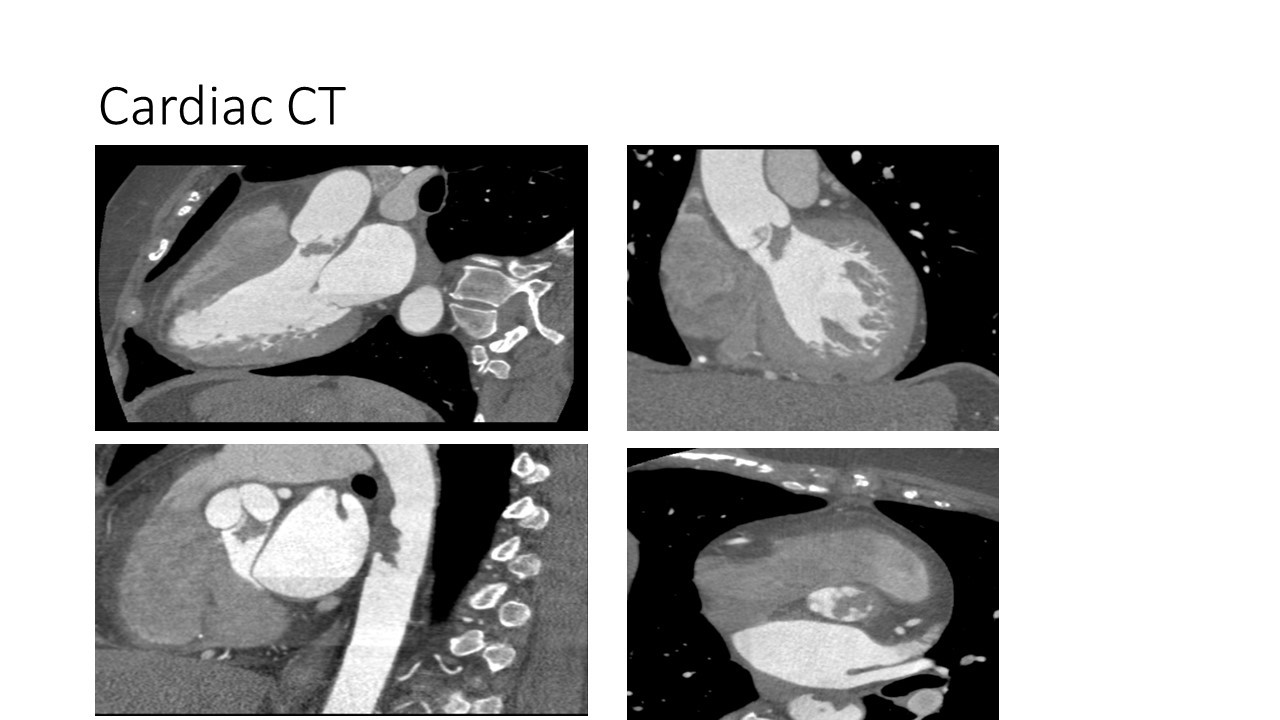
Figure 3