Atherogenic Dyslipidemia in Diabetes Mellitus: A Literature Review of Pathophysiology and Potential Drugs for Treatment
Atherogenic Dyslipidemia in Diabetes Mellitus: A Literature Review of Pathophysiology and Potential Drugs for Treatment
Raphael de Magalhães Cipriano a, Thayná Nara Costa Silva a, João Pedro Mores Artifon a, Larissa Gomes Melo Matos a, Artur de Tassis Cabral Fernandes a, Mariana da Costa Portugal Duarte b, Rodrigo Oliveira Moreira d,e, Humberto Batista Ferreira a,f
a Faculdade Ciências Médicas de Minas Gerais (FCM-MG). Belo Horizonte - MG, Brazil.
b Felício Rocho Hospital. Belo Horizonte. MG, Brazil.
d Centro Universitário Presidente Antônio Carlos Juiz de Fora (UNIPAC/JF). Juiz de Fora - MG, Brazil.
e Instituto Estadual de Diabetes e Endocrinologia Luiz Capriglione (IEDE). Rio de Janeiro - RJ, Brazil.
f Universidade Federal de Minas Gerais (UFMG). Belo Horizonte - MG, Brazil.
*Correspondence to Raphael de Magalhães Cipriano, Faculdade Ciências Médicas de Minas Gerais (FCM-MG). Belo Horizonte - MG, Brazil.
Copyright
© 2025 Raphael de Magalhães Cipriano. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 02 January 2025
Published: 17 January 2025
DOI: https://doi.org/10.5281/zenodo.14677416
Abstract
INTRODUCTION: Dyslipidemic in diabetic patients is an important factor in the increase of cardiovascular risk. The use of statins reduces mortality and cardiovascular risk, mainly by decreasing LDL levels. AIMS: Review the cardiovascular risk in diabetic, the therapies used, their benefits and risks. METHODS: The present review was conducted using the PICOs a search strategy. By means of a literature search in CENTRAL (MEDLINE) via Pubmed and EMBASE databases. RESULTS AND DISCUSSION: The studies included in the review presented as outcomes to statin use the reduction of overall mortality between 10-14% in primary prevention with risk factors for cardiovascular events. A 25% reduction in all-cause relative risk was noted, and a trend toward a near 22% reduction in the number of fatal and nonfatal strokes. In 7 other clinical trials, a 30% reduction in the number of fatal acute infarctions was estimated. CONCLUSION: Secondary prevention is well established in diabetic patients using statins, its risks and benefits are balanced with additional gain in longer life to the patient and low risk of complications. In primary prevention there is a need for stratification of patients so that we achieve the greatest individual benefit.
Keywords: Diabetes; Hypercholesterolemia; Cardiovascular Risk; Statins.
Atherogenic Dyslipidemia in Diabetes Mellitus: A Literature Review of Pathophysiology and Potential Drugs for Treatment
Introduction
Dyslipidemia is a cumulative risk factor alongside other metabolic disorders in patients with diabetes mellitus (DM) that increases cardiovascular risk. In this patient group, atherogenesis is accelerated by quantitative and qualitative characteristics of cholesterol patterns, suggesting higher cardiovascular risk (CVR).¹.
According to the World Health Organization (WHO) and the International Diabetes Federation, it is estimated that by 2045 there will be approximately 630 million people aged 20 to 70 diagnosed with type 2 diabetes mellitus (DM). Complications associated with poor disease control are significant determinants in the costs of public and private healthcare.².
Atherosclerotic cardiovascular disease (ASCVD) is the leading cause of morbidity and mortality among patients with DM, occurring up to 14.6 years earlier. Approximately two-thirds of deaths in these patients are due to cardiovascular diseases (CVD).3
At the diagnosis of DM, dyslipidemia is found in 75-82% of patients. Therefore, an individualized and intensive approach, both pharmacological and non-pharmacological, is necessary.
Clinically, the impact of dyslipidemia on cardiovascular outcomes was established following evaluations from the "Coronary Drug Project" study. Elevated levels of Low Density Lipoprotein (LDL) were established as a direct predictor of risk for mortality and morbidity outcomes related to CVD.
In diabetic patients, the approach to dyslipidemia has been intensively modified with the aim of achieving increasingly challenging reductions, due to gains in life expectancy, cost savings to healthcare systems worldwide, and prevention of cardiovascular events through lowering levels of low-density lipoprotein cholesterol (LDL-C).
The aim of this study is to review cardiovascular risk (CVR), especially in patients with DM, the therapies used, their benefits, and risks.
Methodology
The exploratory review was conducted using an evidence-based review method and aimed to answer the following question: The use of statins is able to prevent cardiovascular outcomes associated with dyslipidemia, and pharmacological therapies are effective and safe?
The search strategy was constructed based on the PICOs framework:
? P (population): population at increased risk of dyslipidemia;
? I (intervention): pharmacological therapy for dyslipidemia;
? C (comparator): placebo;
? O (outcomes): cholesterol control, cardiovascular outcomes, adverse events, and serious adverse events;
? S (studies): randomized clinical trials, literature reviews, systematic reviews, and cohort studies published from 2000 to 2021;
A review was conducted in the CENTRAL (MEDLINE) database via PubMed and EMBASE, using keywords to search for scientific articles evaluating the treatment of dyslipidemia. Double-blind, randomized, controlled clinical trials, systematic reviews, literature reviews, and meta-analyses on dyslipidemia treatment published from 1990 to 2022 were selected.
The sample size calculation was not conducted, as this is a narrative review.
As research instruments, databases available in major methodological references were used.
The search strategy will be adapted to the equivalent language of other reference databases in possible databases.
- LILACS (Latin American and Caribbean Health Sciences Literature);
- MEDLINE (Medlars On Line)
- The Cochrane Central Register of Controlled Trials (CENTRAL);
- PUBMED
The sampling consisted of a two-stage analysis; in the first stage, a simple random sample of studies that meet the eligibility criteria according to the Jadad scale will be conducted. In the second stage, studies that allowed the evaluation of the desired objectives were included.
The data will be stored in the Access 2013 program, Microsoft Corporation®USA. For statistical analysis, the SPSS 21.0 program, IBM®SPSS Statistics, will be used.
With the method adopted for this research, no risks for patients were identified.
Results
In this review, 6 articles were included, encompassing systematic reviews, clinical trials, and literature reviews. Based on the reading of these articles, we organized Table I to highlight aspects such as: article authorship, study design, main data obtained regarding samples/location, participant characteristics, and the main results of the respective articles, focusing primarily on the comparison of cardiovascular outcomes based on the therapeutic approach studied by the authors.
Table I. Main results of the meta-analyses included in this revie
|
Author |
Study design |
Sample / Location |
Participants' characteristics |
Main results |
|
C Baigent et al.4 |
Systematic Review |
Meta-analyses of individual participant data from randomized trials involving at least 1000 participants and at least 2 years of treatment duration comparing more versus less intensive statin regimens. |
169,138 patients, of whom 87,903 were women and 25,920 had a diagnosis of diabetes. 41% of the sample did not have established cardiovascular disease. |
In trials comparing more aggressive therapy versus less intensive statin therapy, the weighted mean reduction in LDL at 1 year was 0.51 mmol/L. Compared to less intensive regimens, more intensive regimens resulted in a highly significant 15% additional reduction in major vascular events, consisting of separately significant reductions in coronary death or non-fatal myocardial infarction of 13%, coronary revascularization of 19%, and ischemic stroke of 16%. |
|
Paul M Ridkeret al.5 |
Clinical Trial |
Randomized clinical trial of 17,802 apparently healthy men and women. |
17,802 apparently healthy men and women. |
Median follow-up of 1.9 years (maximum, 5.0). The use of Rosuvastatin reduced LDL levels by 50% and high-sensitivity C-reactive protein levels by 37%. The rates of the primary endpoint were 0.77 and 1.36 per 100 years of follow-up in the rosuvastatin and placebo groups, respectively, with corresponding rates of 0.17 and 0.37 for myocardial infarction, 0.18 and 0.34 for stroke, 0.41 and 0.77 for revascularization or unstable angina, 0.45 and 0.85 for the combined endpoint of myocardial infarction, stroke, or death from cardiovascular causes, and 1.00 and 1.25 for death from any cause. Consistent effects were observed in all evaluated subgroups. The rosuvastatin group did not have a significant increase in myopathy or cancer but had a higher incidence of physician-reported diabetes. |
|
Rory Collins et al.6 |
Systematic Review |
Review comprising 308 articles that analyze the main aspects of cholesterol reduction and cardiovascular risk reduction, as well as the profile of side effects. |
(The original table did not include the characteristic of patients) |
Reducing LDL cholesterol by 2 mmol/L with an effective low-cost statin regimen (e.g., atorvastatin 40 mg per day for 5 years in 10,000 patients) would typically prevent major vascular events from occurring in about 1000 high-risk patients (i.e., 10% absolute benefit) with pre-existing occlusive vascular disease (secondary prevention) and in 500 patients (i.e., 5% absolute benefit) who are at higher risk but have not yet had a vascular event (primary prevention). Since statin therapy further reduces the risk of vascular events during each year it is taken, longer therapy would yield even greater absolute benefits. The only adverse events definitively shown to be caused by statin therapy — that is, adverse effects of statins — are myopathy (specifically defined as muscle pain or weakness combined with large increases in blood concentrations of creatine kinase) and diabetes. |
|
James A. Blument hal et al.7 |
Randomized Clinical Trial |
Voluntary sample of 160 older sedentary adults with cardiovascular disease (CVD) followed at an academic tertiary care medical center. |
Patients over 60 years old enrolled in the ILLUMINATE trial between December 2011 and March 2016. |
The prevalence of obesity, central obesity, and lipids were elevated at 13%, 11%, and ≥20%, respectively, and 70% of the children had at least one cardiometabolic risk factor. Most correlations between obesity and central obesity indicators were moderate to strong (0.40 < r < 0.96). Obesity was positively, but weakly associated with C-reactive protein in both sexes and with homeostasis model assessment of insulin resistance only in girls (all r < 0.3, P < 0.05). Obesity indicators were not related to interleukin-6 concentrations and lipids (P > 0.05). Overall, obesity indicators explained a maximum of 8% of the variability in cardiometabolic risk factors. |
|
Richard Kones et al.8 |
Non-systematic Literature Review |
516 randomized clinical trials, cohort studies, and prospective studies. |
Heterogeneous and multivariate analysis not amenable to individual comparison. Heterogeneous profiles. |
In primary prevention, traditional risk factors used in combination to generate global scores do not predict risk sufficiently, nor do they adequately discriminate between those who will have cardiovascular events and those who will not. Defining the best approach to cardiovascular prevention cannot currently be based solely on hard endpoint data but partly on evidence-based synthesis using inductive reasoning. |
|
Rory Collins et al.6 |
Systematic Review |
Review comprising 308 articles that analyze the main aspects of cholesterol reduction and cardiovascular risk reduction, as well as the profile of side effects. |
(The original table did not include the characteristic of patients) |
Reducing LDL cholesterol by 2 mmol/L with an effective low-cost statin regimen (e.g., atorvastatin 40 mg per day for 5 years in 10,000 patients) would typically prevent major vascular events from occurring in about 1000 high-risk patients (i.e., 10% absolute benefit) with pre-existing occlusive vascular disease (secondary prevention) and in 500 patients (i.e., 5% absolute benefit) who are at higher risk but have not yet had a vascular event (primary prevention). Since statin therapy further reduces the risk of vascular events during each year it is taken, longer therapy would yield even greater absolute benefits. The only adverse events definitively shown to be caused by statin therapy — that is, adverse effects of statins — are myopathy (specifically defined as muscle pain or weakness combined with large increases in blood concentrations of creatine kinase) and diabetes. |
|
James A. Blument hal et al.7 |
Randomized Clinical Trial |
Voluntary sample of 160 older sedentary adults with cardiovascular disease (CVD) followed at an academic tertiary care medical center. |
Patients over 60 years old enrolled in the ILLUMINATE trial between December 2011 and March 2016. |
The prevalence of obesity, central obesity, and lipids were elevated at 13%, 11%, and ≥20%, respectively, and 70% of the children had at least one cardiometabolic risk factor. Most correlations between obesity and central obesity indicators were moderate to strong (0.40 < r < 0.96). Obesity was positively, but weakly associated with C-reactive protein in both sexes and with homeostasis model assessment of insulin resistance only in girls (all r < 0.3, P < 0.05). Obesity indicators were not related to interleukin-6 concentrations and lipids (P > 0.05). Overall, obesity indicators explained a maximum of 8% of the variability in cardiometabolic risk factors. |
|
Richard Kones et al.8 |
Non-systematic Literature Review |
516 randomized clinical trials, cohort studies, and prospective studies. |
Heterogeneous and multivariate analysis not amenable to individual comparison. Heterogeneous profiles. |
In primary prevention, traditional risk factors used in combination to generate global scores do not predict risk sufficiently, nor do they adequately discriminate between those who will have cardiovascular events and those who will not. Defining the best approach to cardiovascular prevention cannot currently be based solely on hard endpoint data but partly on evidence-based synthesis using inductive reasoning. |
BMI: Body Mass Index; CVD: Cardiovascular Diseases; IR: Insulin Resistance.
Discussion
Atherogenic Dyslipidemia and Cardiovascular Risk
On average, 25% of body cholesterol is obtained from the diet, and 75% is synthesized in hepatocytes via the mevalonate pathway. In the bloodstream, cholesterol is transported in the form of lipoproteins, especially LDL and high-density lipoprotein (HDL). The regulation of the transport process occurs through apolipoproteins.10-12
Atherogenesis is a process characterized by the gradual and linear oxidation of vascular structures through the formation of foam cells (FCs), macrophages filled with cholesterol molecules with a pro-inflammatory phenotype, in the intima and media layers. This process exhibits different biomolecular characteristics in certain individuals.13
Patients with insulin resistance (IR), such as in DM and metabolic syndrome (MS), exhibit accelerated oxidation of FCs compared to patients without IR.
There is deposition of a molecule called Small Dense LDL (sd-LDL), a smaller phenotype of LDL-C with higher affinity for proteoglycans in the arterial wall, a higher percentage of apolipoprotein B, and more susceptible to glycation. It is associated with elevated triglyceride (TG) levels and low HDL-C concentration, accelerated lipolysis and proteolysis processes, acting as a chronic stimulator of inflammation. There is activation of the coagulation cascade to express adhesion molecules on the surface that bind to receptors on circulating monocytes and stimulate migration to the intima.14
Figure 1 - Chylomicron remnants accumulation contributes to the progression of atherosclerotic plaque
Image provided free of charge Copyright 2017 Japan Atherosclerosis Society. This article is distributed under the terms of the latest version of the CC BY-NC-SA Creative Commons Attribution license. http://creativecommons.org/licenses/by-nc-sa/3.0/
Legend: Many metabolic disorders are associated with the accumulation of chylomicron remnants and high concentrations of apolipoprotein B-48, such as Chronic Kidney Disease, Metabolic Syndrome, Impaired Glucose Tolerance, Diabetes Mellitus, Postprandial Hypertriglyceridemia and Type III Hyperlipidemia. In serum, chylomicron remnants can directly penetrate into the arterial wall and infiltrate the subendothelial space, contributing to systemic inflammation, platelet activation, smooth muscle cell proliferation, monocyte adhesion, endothelial cell apoptosis, and the proliferation of foam cells rich in cholesterol. Atherosclerotic tissues exhibit a significantly higher concentration of chylomicron remnants, suggesting it is a primary cause of atherosclerosis.
Dyslipidemia has multiple and interactive pathophysiology that not only includes the atherosclerotic process. Several factors contribute to the phenomenon of accelerated atherosclerosis, such as: systemic arterial hypertension (SAH), IR, obesity, and the new concept of visceral fat.15
Recent evidence suggests that the most important factor in atherogenesis is the binding of modified LDL to Toll-like receptors (TLRs), which is the main trigger for the secretion of these pro-inflammatory factors. Activation of TLRs triggers the NF-Kappa B pathway and activating protein-1, which modulate the expression of pro-inflammatory cytokines. Internalization into macrophages by scavenger receptors is responsible for inflammasome activation, stimulating the secretion of IL-1β, which favors plaque progression and instability.15,16
Although LDL is recognized as the main source of intracellular lipid accumulation in the plaque, native LDL particles do not cause accumulation in cultured cells, therefore, they seem to lack atherogenicity.15
The pathophysiological explanation of this phenomenon has some theories, which are:
1. Due to their higher density, they have lower affinity with endothelial LDL receptors, resulting in longer circulation time and a tendency to establish vascular deposits and oxidative phenomena;
2. They penetrate the arterial vascular intima more easily and bind more readily to proteoglycan structures of the wall, favoring the development of cholesterol streaks;
3. They are molecules more susceptible to oxidation and FCs formation.
HDL and its potential for cardiovascular protection
Low plasma levels of HDL-C appear to represent a robust and independent marker of increased cardiovascular risk. However, no significant evidence demonstrates that this is additive in premature ASCVD. HDL levels may contribute to atheroprotection through cellular cholesterol efflux, attenuating inflammation, cell apoptosis, and platelet cascade activation.17
One of the components linking the biological functions of HDL to ASCVD focuses on the defective function of HDL in low HDL-C dyslipidemias. Impaired cholesterol reverse transport pathway suggests accelerated atherosclerosis in individuals with Tangier disease among other dyslipidemias.14
Despite advances and improvements in the management of CVD, reliable tests are still needed to estimate this risk. Epidemiological studies suggest an inverse association between cardiovascular risk and plasma HDL concentration. While clinical trials have not yet shown that management with pharmacological elevation of HDL would be predictors in reducing mortality or providing direct benefit to primary outcomes in patients.18,19
Visceral Fat and Cardiovascular Risk
Visceral adiposity promotes systemic and vascular inflammation that is fundamental to CVD, from the development of endothelial streaks to atherothrombosis.20
There is an increase in the probability and speed of LDL oxidation. Especially in obese patients, there is a reduction in the antioxidative potential in nitric oxide molecules. Several prospective epidemiological studies correlate patients with higher levels of visceral fat with the incidence of death, fatal and non-fatal MI, peripheral arterial disease, arterial revascularization, fatal and non-fatal stroke, and deaths from all causes (MACE).
Epicardial fat shares many of the pathophysiological properties of other visceral fat deposits, similar to excess hepatic fat, and both appear to be a central factor responsible for several cardiometabolic complications and association with MACE.9
Studies prove that epicardial fat volume is a modifiable cardiometabolic risk factor that presents a therapeutic target. Reduction can be achieved through weight loss, bariatric surgery, or pharmacological treatments.9,21
In obese patients, weight loss is associated with an increase in the adiponectin/leptin ratio and a reduction in pro-inflammatory cytokines, as well as mortality from various causes. Regarding the use of GLP-1, the results are similar. The epicardium presents receptors for this hormone, which favors its action.
Physical activity, especially aerobic exercise, is associated with improved insulin sensitivity, endothelial function, and reduction of pro-inflammatory markers, independent of weight loss. Lifestyle changes have been shown to reduce visceral fat and ectopic fat. The Look AHEAD study demonstrates that a loss of ≥10% of body weight is associated with significant reductions in cardiovascular events.4,9
Given the prospect and possibility of percentage reduction in this fat, various observational and intervention studies seek to develop cardiovascular health scores with correlations between visceral/epicardial adipose tissue, abdominal circumference, blood pressure, insulin resistance, and dyslipidemia. These constitute future alternatives in the stratification and optimization of intensive patient treatment.
Hypertriglyceridemia and residual cardiovascular risk
In hypertriglyceridemia, it is common to have subnormal levels of HDL-C and elevated TG content in HDL particles secondary to the action of cholesteryl ester transfer protein. Subnormal levels of HDL-C result from significant changes in cholesterol metabolism, as typified by common dyslipidemic states: hypertriglyceridemia, hypercholesterolemia, and mixed dyslipidemia.
The properties of HDL molecules are less beneficial than in patients without metabolic syndrome. In patients with IR, it appears that denser chylomicron molecules rise and exhibit a more pronounced oxidative potential.
Other risk factors such as age, hypertension, metabolic syndrome, smoking, and sedentary lifestyle, along with various other factors, contribute to the formation of the so-called Residual Cardiovascular Risk, which statin use is unable to reduce.
Furthermore, the vascular inflammatory process appears to result in increased sodium and water retention, leading to intravascular volume overload.
Pharmacological Treatment for Atherogenic Dyslipidemia
1.1 STATIN MEDICATIONS
1.2 Effectiveness of Statins and Therapeutic Targets
Statins are medications that inhibit the intracellular enzyme called Hydroxymethylglutaryl-CoA Reductase (HMG-CoA), which is responsible for cholesterol synthesis. By blocking HMG-CoA and the pathway of synthesis of sterol regulatory element-binding proteins (SREBPs), there is increased expression of LDL receptors. Additionally, there is a direct reduction in the production of the precursor metabolite for cholesterol synthesis, Mevalonic Acid. This leads to an indirect reduction in VLDL and TG synthesis.22
The use of statins in primary prevention is suggested when the patient has a high risk in CVD stratification, meaning when this risk over 10 years is greater than or equal to 10%.
In secondary prevention, the use of statins is well-established to reduce mortality and MACE. Randomized clinical trials demonstrate that reducing LDL cholesterol reduces the risk of events proportionally to the absolute decrease in its values, independent of other risk factors.6,7
Meta-analyses of large studies, such as the CTT, confirm that statin therapy reduces overall mortality by 10-14% even in primary prevention. The CTT study defines a reduction in relative risk (RR) by 25% in cardiovascular deaths from all causes and by 22% in strokes. Seven other clinical trials estimated a reduction in RR by 30% in the number of fatal heart attacks.23-25
In general, the Number Needed to Treat (NNT) to prevent 1 death from any cause with statin use varies but has approached similar values in different studies. When assessing all-cause mortality in low-risk patients, the NNT to prevent one death ranges from 250 to 138. In high-risk patients, the NNT ranged from 20 to 54. In secondary prevention, the NNT for deaths ranged from 11 to 53. As for reducing non-fatal heart attacks, this value was close to 39.28-30
Three major studies, 4S, LIPID, and TNT, demonstrate in secondary prevention a reduction in RR of new events by 42%, 24%, and 22%, respectively.
1.2 Adverse events associated with statins
Statins generally have good tolerability, and their use rarely causes serious complications. However, it is important to address some occurrences, such as the risk of diabetes, musculoskeletal effects, liver diseases, and cognitive deficits.
1.2.1 Glucose Intolerance
The mechanisms by which statin use induces hyperglycemia are not fully understood. Chronic statin use increases gluconeogenesis and impairs insulin signaling pathway and GLUT-4 transporter.29
Pancreatic β cells are also compromised by statin use, as they alter circulating free fatty acids (FFAs), which are strongly related to adiponectin and leptin. These hormones cause damage to β cells, affecting adipocyte maturation and differentiation.29
1.2.2 Skeletal Muscle Effects
The main adverse event associated with statins is myopathy, especially myalgia. On average, around 2 to 10% of patients experience this symptom, whether related to the elevation of muscle inflammatory markers or not. The PRIMO study assessed this adverse event in 7,924 patients. The average time between the onset of side effects and the use of statins was 1 to 6 months.30,31
Myalgia is a differential diagnosis established after excluding other causes. In the case of myalgia, there is no elevation in CPK levels. In myopathy, CPK levels and Glutamic-oxaloacetic transaminase (AST)/Alanine aminotransferase (ALT) increase. Clinical trials and meta-analyses have shown serious complications such as rhabdomyolysis with an incidence of <0.01%.31
All major trials and meta-analyses involving statin use have concluded that the overall benefit of their use outweighs the risk associated with myopathies.29,31
1.2.3 Cognitive Impairment
Statin use may contribute to cognitive impairment, such as reversible memory loss, after discontinuation of the medication. According to the Food and Drug Administration
(FDA), cognitive decline is not clinically significant; however, it may cause functional deficits and loss of quality of life. Statin therapy should be evaluated due to mild cognitive impairment, vascular dementia, and Alzheimer's disease. 30
2. EZETIMIBE - Intestinal cholesterol absorption inhibitors
Ezetimibe acts on the microvilli of the intestinal lumen, blocking the NPC1-L1 enzyme (Niemann-Pick C1-Like 1). There is increased cellular expression of LDL receptors with reduced hepatic cholesterol synthesis and increased serum absorption, reducing the amount of circulating cholesterol. Alone, it reduces LDL-C by an average of 10-18%, but there are no studies with well-established results on the benefit of monotherapy in reducing cardiovascular mortality.32
The IMPROVE-IT study brought a potential breakthrough for Ezetimibe when added to Simvastatin, leading to a cholesterol reduction close to 25%, enhancing the potency of statins. The aggressive reduction of cholesterol from this combination has promoted the emergence of new therapeutic tools for dyslipidemia in high-risk and very high-risk patients.30
Compared to a group using Ezetimibe + Simvastatin 40mg (group 1) "versus" patients using simvastatin 40mg/day (group 2), a reduction of 7.2% in major vascular events was observed, with a need to treat 50 patients to prevent one death from all causes. Patients with DM showed greater benefit with ezetimibe/simvastatin, with a 14% reduction in the odds ratio of cardiovascular death. 32
The indications for Ezetimibe include its use in combination with statins when reduction targets have not been achieved and in patients who need to lower their cholesterol levels but have some contraindication to statin use or an increase in their dose. Adverse events are rare and minor, mainly non-serious gastrointestinal symptoms.32
3. PCSK9 Inhibitor
PCSK9 inhibitors (iPCSK9) are monoclonal antibodies that act by preventing PCSK9 from binding to the LDL receptor, increasing its availability in hepatocytes, thus allowing a marked reduction in serum LDL-C levels and in the secondary risk of CVD in patients with genetic disorders associated with dyslipidemia alleles. 31-33
Therefore, the FOURIER, ODISSEY, and SPIRE-2 studies suggest that PCSK9 inhibitors (Evolocumab and Alirocumab) can be safely used in patients with statin intolerance and/or therapeutic failure, without a significant increase in adverse events related to skeletal muscle.32-35
It seems advantageous to combine iPCSK9 with high-intensity statins due to their effect on stabilizing atherosclerotic plaques and reducing cholesterol levels. There are no robust studies confirming the additive potential of dual lipid-lowering therapy in reducing cardiovascular mortality. However, it is possible to extend the results of the CTT 2010 study, which associates lower LDL levels with a reduction in relative risk.
The therapeutic and pharmacological safety is well established, making it a safe medication from a pharmacokinetic perspective.
Although there are randomized clinical trials available, meta-analyses on the topic still need to be better developed. The high cost of these medications is a limiting factor in their prescriptions, as well as the lack of studies demonstrating efficacy in homozygous monogenic familial dyslipidemias.32-35
The first step in the therapy for patients with dyslipidemia consists of non-pharmacological treatments, followed by the use of high-potency statins. Simulation model studies demonstrate that approximately 30% of patients with hypercholesterolemia will achieve expected reduction goals with these measures alone.42 The next step will be to consider the use of Ezetimibe, and in case of therapeutic failure, evaluate the prescription of an iPCSK9.32-35
4. Fibrates
Fibrates are important medications for addressing risks associated with hypertriglyceridemia. They act by activating peroxisome proliferator-activated receptor alpha (PPAR-alpha) receptors. They have a good response in fasting and postprandial triglyceride levels, with a possible additive effect in reducing LDL cholesterol.
Several studies have presented inconclusive results regarding the cardiovascular effect in patients with TG levels <500. The effective reduction of LDL cholesterol levels is still controversial and seems to be related to the reduction of TG itself, given that there is a paradoxical elevation of LDL in high TG levels.
Another important effect associated with fibrates is the elevation of HDL cholesterol through increased levels of Apolipoprotein AI.
In different studies such as FIELD, ACCORD, and LEADER, there was no additional benefit in using fibrates alongside statins. The LEADER study even sought to explore the potential benefit of using Gemfibrozil but also did not show evidence.
Therefore, the isolated use of fibrates for reducing cardiovascular outcomes is not a recommended practice.
5. OMEGA-3
Omega-3 are oily derivatives from fish commonly found in cold waters, with Docosahexaenoic acid (DHA) and eicosapentaenoic acid (EPA) being the most important. At the liver level, these derivatives inhibit the synthesis of TG.
The REDUCE-IT study, published in 2019, evaluated the impact of using 4g/day of EPA versus placebo (mineral oil) in patients at high cardiovascular risk and undergoing statin treatment. A total of 8,179 patients were assessed for an average of
4.9 years. The risk of ischemic events, including cardiovascular death, was significantly lower (25%) in those who received EPA.36
The STRENGTH study, published in 2020, found different results. 13,078 high-risk cardiovascular participants undergoing statin treatment were given either 4g/day of omega-3 or corn oil. This study was projected to last 4.5 years but was stopped early due to the low likelihood of demonstrating a clinical benefit of omega-3 compared to corn oil.37
The TG level was reduced by 18% after 12 months in both groups. Both studies also identified a small increase in new cases of atrial fibrillation compared to placebos.36,37
Omega-3 has become an important therapy to be considered, especially in patients with hypertriglyceridemia already undergoing optimized statin treatment, as an alternative to further reduce cardiovascular risk.
Table II - Most commonly used medications in clinical practice for the treatment of dyslipidemia, adverse events and contraindications(Fig 1 & 2)
*Additional reduction when used alongside statins. ¹ Fluctuating variation. No long-term beneficial effects on HDL. ² There was no benefit in this increase and in reducing cardiovascular risk. ³ When used at doses between 2-4% in patients intolerant or contraindicated to other medications.
6. Mipormesen
Another important therapy for patients with hypercholesterolemia, not yet approved in Brazil, is Mipomersen. The use of this medication, when combined with a statin in patients with familial hypercholesterolemia, reduces LDL-C by between 25% and 28%.38-40
Mipomersen is an antisense oligonucleotide targeting apolipoprotein B-100, which is essential for the synthesis of LDL and VLDL. These molecules use synthetic DNA structures to target specific messenger RNA structures and are responsible for encoding apo B 100 synthesis. Consequently, mipomersen inhibits protein transcription and its intracellular concentration, leading to a final reduction in the synthesis of LDL molecules and atherogenesis.38-40
The most common adverse events are related to local application of the medication, such as erythema, itching, and pain. The most serious adverse effect of this medication is hepatotoxicity, although it is uncommon. It is contraindicated in patients with severe liver dysfunction and should be prescribed with caution in patients using hepatotoxic medications.
Before initiating its prescription, it is suggested to perform laboratory tests for serum levels of transaminases, alkaline phosphatase, and total bilirubin, as well as serum levels of total cholesterol and fractions every 3 months, aiming for maximum reduction in LDL cholesterol after 6 months of using this medication.38-40
Conclusion
The challenges in therapy and controlling cardiovascular mortality in patients with diabetes associated with lipid-lowering therapy still present significant barriers. Although this therapy is well-established for secondary prevention, recent meta-analyses suggest a need for clarification in certain specific groups, especially young diabetic individuals in primary prevention.
The excess of cardiovascular deaths, even in patients with optimized cholesterol therapy, is attributed to the so-called residual effect. Intensive control of blood pressure and glycated hemoglobin levels, along with non-pharmacological measures, is necessary. Additionally, there's a need to more precisely stratify cardiovascular risk.
Statin therapy reduces cardiovascular risk and overall mortality events significantly. The use of statins is beneficial as primary prevention in patients without established CVD but with risk factors, also reducing mortality in this setting. Adverse events of lipid-lowering medications are often reported in studies, but the benefits outweigh the risk of complications.
Declaration of Competing Interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Authorship and Author Contributions
All authors contributed to the conception, writing and editing of this manuscript.
ROM and HBF reviewed it. All authors read and approved the final manuscript.
References
1. Fulcher J, R O'Connell, M Voysey, Emberson J, Blackwell L, B Mihaylova, et al. Efficacy and safety of LDL-lowering therapy among men and women: meta-analysis of individual data from 174 000 participants in 27 randomised trials. The Lancet. 2015 Apr 11;385(9976):1397-405. https://doi.org/10.1016/S0140-6736(14)61368-4
2. Kaptoge S, Pennells L, Dirk De Bacquer, Marie Therese Cooney, Kavousi M, Stevens G, et al. World Health Organization cardiovascular disease risk charts: revised models to estimate risk in 21 global regions. The Lancet Global Health. 2019 Oct 1
;7(10):e1332–45. https://doi.org/10.1016/S2214-109X(19)30318-3
3. Low Wang, Cecilia C., et al. “Clinical Update: Cardiovascular Disease in Diabetes Mellitus.” Circulation, vol. 133, no. 24, 14 June 2016, pp. 2459–2502. https://doi.org/10.1161/CIRCULATIONAHA.116.022194
4. C Baigent, Keech A, Kearney PM, Blackwell L, Buck G, Pollicino C, et al. Efficacy and safety of cholesterol-lowering treatment: prospective meta-analysis of data from 90 056 participants in 14 randomised trials of statins. The Lancet . 2005 Oct 1 ;366(9493):1267–78. https://doi.org/10.1016/S0140-6736(05)67394-1
5. Ridker PM, Everett BM, Thuren T, MacFadyen JG, Chang WH, Ballantyne C, et al. Antiinflammatory Therapy with Canakinumab for Atherosclerotic Disease. The New England Journal of Medicine. 2017 Sep 21 ;377(12):1119–31. https://doi.org/10.1056/nejmoa1707914
6. Collins R, Reith C, Emberson J, Armitage J, Baigent C, Blackwell L, et al. Interpretation of the evidence for the efficacy and safety of statin therapy. The Lancet. 2016 Nov 1;388(10059):2532–61. https://doi.org/10.1016/s0140-6736(16)31357-5
7. Blumenthal JA, Smith PJ, Mabe S, Hinderliter A, Welsh?Bohmer K, Browndyke JN, et al. Longer Term Effects of Diet and Exercise on Neurocognition: 1?Year Follow?up of the ENLIGHTEN Trial. Journal of the American Geriatrics Society. 2019 Nov 22;68(3):559–68. https://doi.org/10.1111/jgs.16252
8. Kones R. Primary prevention of coronary heart disease: integration of new data, evolving views, revised goals, and role of rosuvastatin in management. A comprehensive survey. Drug Design Development and Therapy . 2011 Jun 1;325–5. https://doi.org/10.2147/dddt.s14934
9. Powell-Wiley TM, Poirier P, Burke LE, Jean-Pierre Després, Gordon-Larsen P, Lavie CJ, et al. Obesity and Cardiovascular Disease: A Scientific Statement From the American Heart Association. Circulation. 2021 May 25;143(21). https://doi.org/10.1161/cir.0000000000000973
10. Goldstein JL, Brown MS. Regulation of the mevalonate pathway. 1990 Feb 1;343(6257):425–30. https://doi.org/10.1038/343425a0
11. Feingold KR, et al. Introduction to Lipids and Lipoproteins. Endotext. 2024 jan 14.
12. Ginsberg HN. LIPOPROTEIN PHYSIOLOGY. Endocrinology and Metabolism Clinics of North America. 1998 Sep 1;27(3):503–19. https://doi.org/10.1016/s0889-8529(05)70023-2
13. Theodosios Filippatos, Vasilios Tsimihodimos, Pappa E, Elisaf M, et al. Pathophysiology of Diabetic Dyslipidaemia. Current Vascular Pharmacology. 2017 Sep 28;15(6). https://doi.org/10.2174/1570161115666170201105425
14. Fan J, Liu Y, Yin S, Chen N, Bai X, Ke Q, et al. Small dense LDL cholesterol is associated with metabolic syndrome traits independently of obesity and inflammation. Nutrition & Metabolism. 2019 Jan 21;16(1). https://doi.org/10.1186/s12986-019-0334-y
15. Multiple risk factor intervention trial. Risk factor changes and mortality results. Multiple Risk Factor Intervention Trial Research Group. JAMA. 1982 Sep 24; 248(12): 1465-1477. https://doi.org/10.1001/jama.1982.03330120023025.
16. Macheboeuf, M.A et al. Sur l'etat physico-chimique de la lecithine et des esters de cholesterol dans le serum et le plasma sanguins. Bulletin de la Societe Chimique de France. 1929; 45-46(7): 662-666
17. Feng M, Fabiana Rached, Anatol Kontush, M. John Chapman et al. Impact of Lipoproteins on Atherobiology. Cardiology Clinics. 2018 May 1; 36(2):193–201. https://doi.org/10.1016/j.ccl.2017.10.001.
18. Toth PP. High-Density Lipoprotein and Cardiovascular Risk. Circulation. 2004 Apr 20 ;109(15):1809–12. https://doi.org/10.1161/01.cir.0000126889.97626.b8.
19. Poznyak A, Grechko AV, Poggio P, Myasoedova VA, Alfieri V, Orekhov AN et al. The Diabetes Mellitus–Atherosclerosis Connection: The Role of Lipid and Glucose Metabolism and Chronic Inflammation. International Journal of Molecular Sciences. 2020 Mar 6;21(5):1835–5. https://doi.org/10.3390/ijms21051835.
20. Kim Y, Je Y. Dietary Fiber Intake and Total Mortality: A Meta-Analysis of Prospective Cohort Studies. American Journal of Epidemiology. 2014 Aug 20;180(6):565–73. https://doi.org/10.1093/aje/kwu174.
21. Santilli F, Simeone PG, Guagnano MT, Leo M, Maccarone MT, Augusto Di Castelnuovo, et al. Effects of Liraglutide on Weight Loss, Fat Distribution, and β-Cell Function in Obese Subjects With Prediabetes or Early Type 2 Diabetes. Diabetes Care. 2017 Sep 14;40(11):1556–64. https://doi.org/10.2337/dc17-0589.
22. Tiwari V, Khokhar M. Mechanism of action of anti-hypercholesterolemia drugs and their resistance. European Journal of Pharmacology. 2014 Oct 1;741:156–70. https://doi.org/10.1016/j.ejphar.2014.07.048.
23. Vavlukis M, Vavlukis A, et al. Adding ezetimibe to statin therapy: latest evidence and clinical implications. Drugs in context. 2018 Jul 9;7:212534. https://doi.org/10.7573%2Fdic.212534.
24. Lloyd-Jones DM, Morris PB, Ballantyne CM, Birtcher KK, Daly DD, DePalma SM, et al. 2017 Focused Update of the 2016 ACC Expert Consensus Decision Pathway on the Role of Non-Statin Therapies for LDL-Cholesterol Lowering in the Management of Atherosclerotic Cardiovascular Disease Risk. Journal of the American College of Cardiology. 2017 Oct 1;70(14):1785–822. https://doi.org/10.1016/j.jacc.2017.07.745.
25. Waters DD, Guyton JR, Herrington DM, McGowan MP, Wenger NK, Shear C. Treating to New Targets (TNT) Study: does lowering low-density lipoprotein cholesterol levels below currently recommended guidelines yield incremental clinical benefit? The American Journal of Cardiology. 2004 Jan 1; 93(2):154–8. https://doi.org/10.1016/j.amjcard.2003.09.031.
26. Paaladinesh Thavendiranathan P, Bagai A, Brookhart MA, Choudhry NK, et al. Primary Prevention of Cardiovascular Diseases With Statin Therapy. Arch Intern Med. 2006 Nov 27;166(21):2307–13. https://doi.org/10.1001/archinte.166.21.2307.
27. Anderson TJ, Grégoire J, Pearson GJ, Barry AR, Couture P, Dawes M, et al. Canadian Cardiovascular Society Guidelines for the Management of Dyslipidemia for the Prevention of Cardiovascular Disease in the Adult. Canadian Journal of Cardiology. 2016 Nov;32(11):1263–1282. https://doi.org/10.1016/j.cjca.2016.07.510.
28. Yerrakalva D, Griffin SJ. Statins for primary prevention in people with a 10% 10-year cardiovascular risk: too much medicine too soon? British Journal of General Practice. 2017 Jan;67(654):40–41. https://doi.org/10.3399%2Fbjgp17X688789.
29. Kashani A, Phillips CO, Foody JM, Wang Y, Sandeep Mangalmurti, Ko DT, et al. Risks Associated With Statin Therapy. Circulation. 2006 Dec 19; 114(25):2788–97. https://doi.org/10.1161/circulationaha.106.624890.
30. Clark, D, Brennan, D, Rocco, M. et al. CLINICAL CHARACTERISTICS ASSOCIATED WITH COMPLETE STATIN INTOLERANCE: THE CLEVELAND CLINIC EXPERIENCE. J Am Coll Cardiol. 2016 Apr, 67 (13_Supplement) 1895. http://dx.doi.org/10.1016/S0735-1097(16)31896-4.
31. Bruckert E, Gilles Hayem, Dejager S, Yau C, Bégaud B, et al. Mild to Moderate Muscular Symptoms with High-Dosage Statin Therapy in Hyperlipidemic Patients —The PRIMO Study. Cardiovascular Drugs and Therap. 2005 Dec 1; 19(6):403–14. https://doi.org/10.1007/s10557-005-5686-z.
32. Improve-It Investigators. Ezetimibe Added to Statin Therapy after Acute Coronary Syndromes. The New England Journal of Medicine. 2015 Jun 18 ;372(25):2387–97. https://doi.org/10.1056/nejmoa1410489.
33. Kazi DS, Penko J, Coxson PG, Guzman D, Wei PC, Bibbins-Domingo K, et al. Cost-Effectiveness of Alirocumab. Annals of Internal Medicine. 2019 Jan 1; 170(4):221–1. https://doi.org/10.7326/m18-1776
34. Raal FJ, Hovingh GK, Blom D, Santos RD, Harada-Shiba M, Bruckert E, Couture P, Soran H, Watts GF, Kurtz C, Honarpour N, Tang L, Kasichayanula S, Wasserman SM, Stein EA. Long-term treatment with evolocumab added to conventional drug therapy, with or without apheresis, in patients with homozygous familial hypercholesterolaemia: an interim subset analysis of the open-label TAUSSIG study. Lancet Diabetes Endocrinol. 2017 Apr;5(4):280-290. https://doi.org/10.1016/s2213-8587(17)30044-x.
35. Fontes?Carvalho R, Pedro Marques Silva, Rodrigues E, Araújo F, Gavina C, Ferreira J, et al. Guia prático para a utilização dos inibidores da PCSK9 em Portugal. Revista Portuguesa de Cardiologia. 2019 Jun 1; 38(6):391–405. https://doi.org/10.1016/j.repc.2019.05.005.
36. Bhatt DL, Steg PG, Miller M, et al. Cardiovascular Risk Reduction with Icosapent Ethyl for Hypertriglyceridemia. N Engl J Med. 2019;380(1):11-22. https://doi.org/10.1056/nejmoa1812792.
37. Nicholls SJ, Lincoff AM, Garcia M, et al. Effect of High-Dose Omega-3 Fatty Acids vs Corn Oil on Major Adverse Cardiovascular Events in Patients at High Cardiovascular Risk: The STRENGTH Randomized Clinical Trial. JAMA. 2020 Dec 8; 324(22):2268-2280. https://doi.org/10.1001/jama.2020.22258.
38. Drugs and Lactation Database (LactMed®). Bethesda (MD): National Institute of Child Health and Human Development; 2006-. Mipomersen.
39. Raal FJ, Santos RD, Blom DJ, A David Marais, Min-Ji Charng, Cromwell WC, et al. Mipomersen, an apolipoprotein B synthesis inhibitor, for lowering of LDL cholesterol concentrations in patients with homozygous familial hypercholesterolaemia: a randomised, double-blind, placebo-controlled trial. The Lancet. 2010 Mar 1; 375(9719):998–1006. https://doi.org/10.1016/s0140-6736(10)60284-x.
40. McGowan MP, Tardif JC, Ceska R, et al. Randomized, placebo-controlled trial of mipomersen in patients with severe hypercholesterolemia receiving maximally tolerated lipid-lowering therapy PLoS One. 2012;7(11):e49006. https://doi.org/10.1371/journal.pone.0049006.
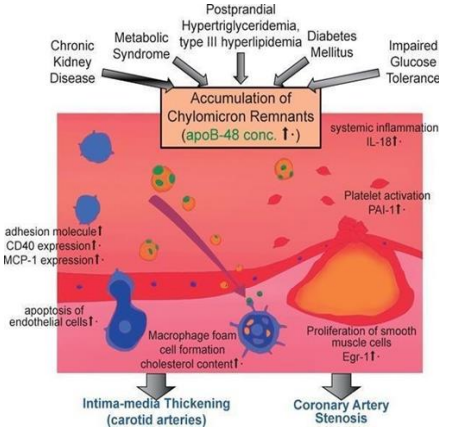
Figure 1