Hypothalamic Hamartoma-Induced Precocious Puberty in a Toddler: A Case Report
Hypothalamic Hamartoma-Induced Precocious Puberty in a Toddler: A Case Report
Patricia Furtenbach1, Patricia Agüero2, Natalia Hoyo3, Maria M Pineyro*4
1,2,3,4. Unidad Académica de Endocrinología y Metabolismo, Hospital de Clínicas “Dr. Manuel Quíntela”,
Facultad de Medicina, Universidad de la República, Montevideo, Uruguay.
*Correspondence to Maria M Pineyro, Avenida Italia S/N, Montevideo UY (CP 116000)
Copyright
© 2025 Maria M Pineyro. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 02 January 2025
Published: 20 January 2025
Abstract
Precocious puberty in males is defined as the development of secondary sexual characteristics before 9 years of age. It is very rare in infants and can be classified as central and peripheral, with central precocious puberty (CPP) being driven by activation of the hypothalamic-pituitary-gonadal axis. Central precocious puberty is isosexual, meaning that the secondary sexual characteristics align with the child’s genetic sex, and it is characterized by an accelerated growth rate and advanced bone maturation. Hypothalamic hamartomas (HH) are rare congenital lesions located in the tuber cinereum, and are one of the most significant causes of CPP in male children. Parahypothalamic hamartomas typically present with central precocious puberty (CPP), while intrahypothalamic hamartomas are associated with the classic triad of gelastic epilepsy, developmental delay, and CPP. Most cases are sporadic, though approximately 5% are associated with Pallister-Hall syndrome, which is linked to genetic anomalies. The main treatment for CPP involves the use of GnRH analogues, with surgery being reserved for severe cases. We report the case of a 21-month-old male who presented with signs of precocious puberty. Hormonal assessment revealed elevated levels of hormones, and a brain MRI confirmed the presence of a hypothalamic hamartoma. Treatment with leuprolide acetate was successful. Timely diagnosis and treatment are essential to prevent psychological sequelae and affect the prognosis of final adult height in cases of CPP. Hypothalamic hamartomas, although rare, can present solely with CPP, necessitating long-term follow-up with a multidisciplinary team.
Keywords: Hypothalamic hamartoma, Precocious puberty, toddler, gonadotropin-releasing hormone (GnRH) analogues
Hypothalamic Hamartoma-Induced Precocious Puberty in a Toddler: A Case Report
Introduction
Precocious puberty in boys is defined as the onset of secondary sexual characteristics before the age of 9 1. This condition, with a low prevalence of less than 5 cases per 10,000, occurs up to 10 times less frequently compared to girls and is classified as either central or peripheral. Central precocious puberty (CPP) originates from the activation of the pituitary-gonadal axis and presents isosexually. It manifests with sequential maturation that mimics normal puberty, starting with an increase in testicular volume, followed by pubarche and penile growth. These changes are accompanied by an increase in growth rate and an acceleration of bone age. Luteinizing hormone (LH), measured by immunochemiluminescence, is indicative of CPP when it exceeds 0.2 to 0.3 mIU/mL. The gonadotrophin stimulation test with gonadotropin-releasing hormone (GnRH) or its analogues confirms the diagnosis of CPP, showing an LH peak greater than 5-7 mU/ml and/or an LH/FSH ratio greater than 0.6-1 1-3.
The causes may include lesions of the central nervous system (CNS) (33-90%), genetic factors, familial patterns or idiopathic originis 4.
Hypothalamic hamartoma is the most common CNS lesion associated with CPP. It is a non-neoplastic congenital lesion that contains normal neurons and glia, generally 0.5-2 cm in size. The precise incidence is not completely established, although it is estimated to vary between 1 in 50,000-100,000, and 1 in 1,000,000. A slight predominance is observed in the male population. The clinical presentation varies according to morphology, size and location, with the pedunculated (parahypothalamic) types generating CPP by autonomously releasing GnRH 4-5. Intrahypothalamic hamartomas present with the classic triad of gelastic epilepsy, developmental delay and CPP. Central precocious puberty has been reported in 30-85% of patients with hamartomas 6,7.
Treatment involves the use of gonadotropin-releasing hormone (GnRH) analogues to reverse or stabilize pubertal development, aiming to mitigate the physical and psychological implications 8.
We present a clinical case of a male infant with precocious puberty due to a hypothalamic hamartoma that presented with isolated CPP.
Case Presentation
A 21-month-old male who presented with pubarche, testicular growth and increase in penis size over the past six months. He did not have seizures. Genital examination showed 5 cc testicles, Tanner stage III pubic hair, and a 6 cm increase in penis size (Figure 1).
Figure 1. A: Increase size of penis, B: testes tanner II.
This was accompanied by an increase in growth velocity of 22 cm/year, calculated in 9 months (Figure 2).
Figure 2. WHO Length Chart. Showing increased length for age percentile.
Paraclinical tests reveal elevated levels of LH 2.20 IU/L, FSH 0.66 IU/L and free testosterone 2.58 pg/ml
(normal range for 6 month to 4 years : 0,05- 0,50 pg/ml). Cranial magnetic resonance imaging focused in the sellar region showed an isointense expansive lesion relative to the gray matter behind the pituitary stalk and in relation to the floor of the third ventricle (Figure 3).
Figure 3. Cranial magnetic resonance imaging revealed an isointense expansive lesion behind the pituitary stalk (red arrow).
Given the location and characteristics of the lesion, a hypothalamic hamartoma is suspected. Treatment is initiated with depot GnRH analogues, specifically leuprolide acetate 1.87 mg administered intramuscularly every 28 days. A favorable therapeutic response was achieved, evidenced by a decrease in growth velocity, testicular volume and penis size.
Discussion
Puberty begins with the pulsatile secretion of GnRH, which activates the hypothalamic-pituitary-gonadal axis. Tanner stages are used to evaluate pubertal development. In boys, the onset of puberty is characterized by testicular enlargement, which corresponds to Tanner stage 2 of genital development, defined as a testicular volume greater than 4 ml7. In this case, the clinical examination revealed a testicular volume of 5 ml as an element of precocious puberty along with an increase of growth velocity for the patient’s age and sex. Hormonal evaluation showed elevated basal gonadotropins and testosterone. While the gold standard for evaluation is the measurement of gonadotropins after stimulation with GnRH, the measurement of basal luteinizing hormone is also a viable alternative. An LH value ≥ 0.3 IU/l, as determined by immunochemiluminescence, can be considered an appropriate cut-off point for the diagnosis of central precocious puberty1. In the imaging evaluation, an isointense expansive lesion was identified in the gray matter behind the pituitary stalk, adjacent to the floor of the third ventricle, consistent with hypothalamic hamartoma9.
Hypothalamic hamartomas are the lesions most frequently associated with central precocious puberty in boys. The risk of presenting an organic lesion increases with the earlier onset of puberty2.
Most cases of hypothalamic hamartoma, approximately 95%, are sporadic, while the remaining 5% are linked to Pallister-Hall syndrome. This syndrome is characterized by abnormalities in the hands and feet, such as polydactyly and postaxial syndactyly, as well as involvement of the larynx, anus and hypothalamus. A mutation in the GLI3 gene, which encodes a transcription factor, has been identified in these cases10-11.They can cause precocious puberty, gelastic seizures and cognitive impairments8.
The clinical presentation of hypothalamic hamartomas varies based on their morphology, size and location. Pedunculated (parahypothalamic) hamartomas can cause CPP by autonomously releasing GnRH, functioning as an accessory hypothalamus and stimulating the secretion of pituitary gonadotropins. Intrahypothalamic hamartomas are associated with epilepsy with gelastic and other types of seizures, which are often pharmacoresistant. These hamartomas can also lead to developmental regression, psychiatric and behavioral comorbidities, and precocious puberty. Magnetic resonance imaging is the most important diagnostic test for hypothalamic hamartomas, as these lesions appear isointense to the gray matter on T1-weighted images and iso- or slightly hyperintense on T2-weighted images, facilitating their diagnosis5,8. The usual treatment of hypothalamic hamartomas involves the use of GnRH analogues, with surgery considered for cases involving drug-resistant seizures, cognitive impairment or behavioral disorders. A systematic review and meta-analysis was conducted to evaluate the effectiveness of surgical intervention in patients with isolated precocious puberty. The analysis included 103 patients from 33 studies. It was concluded that surgical treatment for small-sized and pedunculated hamartomas results in minimal morbidity and excellent outcomes, in contrast to the outcomes of sessile hamartomas12.
Conclusion
Although precocious puberty in boys is rare, it is crucial to evaluate clinical elements of puberty during the physical examination for an adequate diagnosis. Hypothalamic hamartomas require prolonged follow-up with a multidisciplinary team to ensure comprehensive care and optimize the patient's quality of life. Magnetic resonance imaging is the most important diagnostic test for hypothalamic hamartomas, and GnRH analogues are an effective management option for these cases. Timely treatment helps avoid long-term consequences, both psychological and concerning final height prognosis.
Declarations
Ethical Approval
Signed informed consent was obtained directly from the patient’s relatives or guardian for the publication of this case and any related images, as well as for the publication of indirectly identifiable data (age, gender, and medical history). A copy of the consent form can be reviewed by the Editor of this journal.
Funding
There was no funding for this manuscript.
Data availability statement
Data sharing not applicable to this article as no datasets were generated or analyzed during the current study.
Conflicts of Interest
The authors declare that they have no conflicts of interest.
Contributors
PF drafted the manuscript. PA, NH and MP contributed to the writing. All authors contributed to acquiring clinical data, agreed with the manuscript's results and conclusions. PF, PA and MP made critical revisions and approved the final version. All authors revised and approved the final manuscript and agreed to be accountable for the content.
References
1- Miranda-Lora AL, Torres-Tamayo M, Zurita-Cruz JN, Aguilar-Herrera BE, Calzada-León R, Rivera-Hernández AJ, et al. Diagnosis of precocious puberty: Clinical guideline for the diagnosis and treatment of precocious puberty. Bol Med Hosp Infant Mex. 2020;77(Supl 1):7–14.
2- Ab Rahim SN, Omar J, Tuan Ismail TS. Gonadotropin-releasing hormone stimulation test and diagnostic cutoff in precocious puberty: a mini review. Ann Pediatr Endocrinol Metab. 2020 Sep;25(3):152-155. doi: 10.6065/apem.2040004.002. Epub 2020 Jul 30. PMID: 32871650; PMCID: PMC7538306.
3- Kilberg MJ, Vogiatzi MG. Approach to the Patient: Central Precocious Puberty. J Clin Endocrinol Metab. 2023 Jul 14;108(8):2115-2123.
4- Dávila Carmen, Rojas Joselyn, Bermúdez Valmore. Pubertad precoz central secundario a hamartoma hipotalamico. AVFT [Internet]. 2014 Sep [citado 2024 Feb 14] ; 33( 3 ): 79-83. Disponible en: http://ve.scielo.org/scielo.php?script=sci_arttext&pid=S0798-02642014000300002&lng=es.
5- Carballo Cuello CM, De Jesus O. Hypothalamic Hamartoma. 23 de agosto de 2023. En: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; Enero de 2023. PMID: 32809498.
6-Castaño De La Mota C, Martín Del Valle F, Pérez Villena A, Calleja Gero ML, Losada Del Pozo R, Ruiz-Falcó Rojas ML. Hamartoma hipotalámico en la edad pediátrica: características clínicas, evolución y revisión de la literatura [Hypothalamic hamartoma in paediatric patients: clinical characteristics, outcomes and review of the literature]. Neurologia. 2012 Jun;27(5):268-76. Spanish. doi: 10.1016/j.nrl.2011.12.008. Epub 2012 Feb 18. PMID: 22341983
7-Jung H, Neumaier Probst E, Hauffa BP, Partsch C-J, Dammann O. Association of morphological characteristics with precocious puberty and/or gelastic seizures in hypothalamic hamartoma. J Clin
Endocrinol Metab 2003;88:4590-50.
8- Alomari SO, El MN, Bsat S, Moussalem CK, Allouh M, Omeis IA. Hypothalamic hamartomas : A comprehensive review of the literature – Part 1 : Neurobiological features , clinical presentations and advancements in diagnostic tools. Clin Neurol Neurosurg [Internet]. 2020;197(May):106076. Available from: https://doi.org/10.1016/j.clineuro.2020.106076
9- Carel JC, Léger J. Clinical practice. Precocious puberty. N Engl J Med. 2008 May 29;358(22):2366-77. doi: 10.1056/NEJMcp0800459. PMID: 18509122.
10- Rubino S, Qian J, Pinheiro-Neto CD, Kenning TJ, Adamo MA. A familial syndrome of hypothalamic hamartomas, polydactyly, and SMO mutations: a clinical report of 2 cases. J Neurosurg Pediatr. 2018 Oct 12;23(1):98-103
11- Kang S, Allen J, Graham JM Jr, Grebe T, Clericuzio C, Patronas N, Ondrey F, Green E, Schäffer A, Abbott M, Biesecker LG. Linkage mapping and phenotypic analysis of autosomal dominant Pallister-Hall syndrome. J Med Genet. 1997 Jun;34(6):441-6. doi: 10.1136/jmg.34.6.441. PMID: 9192261; PMCID: PMC1050964.
12- Agrawal M, Samala R, Doddamani RS, Goyal A, Tripathi M, Chandra PS. Is surgery effective for treating hypothalamic hamartoma causing isolated central precocious puberty? A systematic review. Neurosurg Rev. 2021;44(6):3087–105.

Figure 1
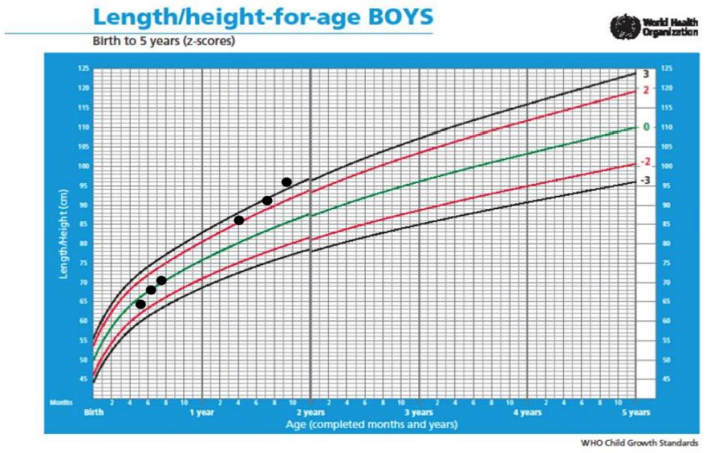
Figure 2

Figure 3