Spinocerebellar Ataxia: A Report of a Very Rare Disease
Spinocerebellar Ataxia: A Report of a Very Rare Disease
Dr. Hassan Jazayeri*
*Correspondence to: Dr. Hassan Jazayeri - Neurologist – Albania.
Copyright
© 2025 Dr. Hassan Jazayeri, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 07 Feb 2025
Published: 14 Feb 2025
DOI: https://doi.org/10.5281/zenodo.14870033
Abstract
Ataxia is a neurological disorder that affects the coordination of body movements. People with ataxia may have difficulty performing simple movements such as walking, standing, and picking up objects. The disorder can affect different parts of the body, such as the arms, legs, trunk, and even the eyes.
Keywords: Polymerase chain reaction, next-generation sequencing , comparative genomic array Ataxan, tuberculosis therapy and DBS
Spinocerebellar Ataxia: A Report of a Very Rare Disease
Introduction
I saw him in the hospital when,he had injuried to his ribs in the back. He was having difficulty breathing and was in critical condition. The cause of the injury was that he had tried to get out of bed, to pick up an object that he had lost control of on the dresser in his room, and as a result, he had fallen and the dresser had hit his back, causing a local injury. Initial examinations and a chest CT scan fortunately ruled out serious lung injuries, but he had to be monitored in the thoracic department for a while in the hospital until his condition stabilized. When I saw him, those around him reminded me that he had a history of ataxia, but no one knew what caused this imbalance. I remembered that I had visited him five years ago and that because his refugee status had not yet been resolved, he could not benefit from full medical services, and the patient's family could not provide him with financial assistance until his problem was definitively diagnosed.
Spinocerebellar ataxia
He told me that, he had a cousin who was almost the same age as him who had this imbalance, when he was very young, and of course his condition was much worse than his. Recently he had not known about his cousin for several years, but he told me that his condition was much better now. When I asked him about his history, I realized that he could not speak fluently. Although his companions understood him well, it was very difficult for me to understand what words he was pronouncing. He said that I have not been able to stand and walk on my own for more than a year and that I mostly use a wheelchair and walker.
He had difficulty swallowing food and had to drink water, especially dry food, which was difficult for him to chew and swallow. He told me that even 30 years ago, when he was in another country, he could easily run and do sports. But over the past ten years, these problems have gradually increased, to the point that he has been paralyzed for almost two years now and needs someone to help him with his personal tasks. One of the most difficult tasks for him is buttoning clothes, which is a delicate and difficult task.
Previously, due to the heterogeneous set of symptoms that this patient had, ataxia had been discussed, but this time, when the patient was re-evaluated, especially from a neurological perspective, we all agreed that he had cerebrospinal ataxia because both the severity of the symptoms had increased significantly and because of his family history, we realized that the problem was not ataxia in the general sense, but rather cerebrospinal ataxia, which naturally progressed and expanded and will continue to do so, although it has not caused any disruption to the brain tissue at present.
Epidemiology:
Its prevalence is 1-2 people per 100,000 population (4)
Age
The age of onset of SCA is highly variable and can occur from childhood to adulthood. In general, different types of SCA have different ages of onset:
A. Childhood onset:
Some types of SCA , such as SCA type 7, may present in childhood with symptoms such as retinitis pigmentosa.
B. Onset in adulthood:
Most types of SCA begin in adulthood, and symptoms progress gradually
Gender
In general SCA is equally common in men and women. However, some studies suggest that some types of SCA may be more common in one sex..
Race
Race can also affect the prevalence of some types of SCA For example, SCA type 2 is more common in the Cuban population.
Geographical area
Some types of SCA are more common in certain geographic areas. This may be due to specific gene mutations in different populations.
Factors affecting prevalence
Gene involved: The type of mutated gene and the number of abnormal repeats in the gene affect the age of onset, severity, and rate of progression of the disease.
Environmental factors: Environmental factors such as nutrition, toxins, and infections may influence the incidence and severity of the disease.
Modifiers: Other genetic factors may influence the expression of the mutated gene and the severity of the disease.
Why is the prevalence almost equal?
Genetic cause: As mention SCA is mainly caused by gene mutations, and a person's gender does not play a direct role in causing these mutations.
Lack of influence of hormones: Unlike some other diseases that are influenced by sex hormones , SCA is not directly related to sex hormones.
Risk factors:
Controllable risk factors:
Healthy lifestyle: Having a healthy diet, exercising regularly, and avoiding alcohol and tobacco can help reduce the risk of developing neurological diseases.
Control underlying diseases: Controlling underlying diseases such as diabetes, high blood pressure, and heart disease can help reduce the risk of disease progression
Uncontrollable risk factors:
Family history: Family history cannot be changed.
Gene mutations: Gene mutations are inherited from parents to children and cannot be changed.
Types of Spinocerebellar ataxia:
Cerebellar ataxia is caused by damage or dysfunction of the cerebellum. There are several types of this condition, each with its own causes and symptoms
Hereditary Spinocerebellar ataxia:
Friedreich's ataxia: The most common type of inherited ataxia, caused by a mutation in the Friedreich gene, symptoms include movement problems, heart problems, and neurological problems.
Ataxia telangiectasia: In addition to movement problems, this disease is associated with dilated blood vessels in the eyes and skin, immune problems, and an increased risk of cancer.
Episodic ataxia: In this type of ataxia, symptoms occur in short, repeated periods.
Acquired Spinocerebellar ataxia:
Ataxia caused by stroke: A stroke that occurs in the cerebellum can cause ataxia
Ataxia caused by a brain tumor: Brain tumors, especially those located in the cerebellum can cause ataxia.
Ataxia due to MS: MS can gradually damage the cerebellum and cause ataxia
Alcohol-induced ataxia: Long-term alcohol use can damage nerve cells in thecerrebeum
Ataxia caused by vitamin deficiencies: Deficiencies in certain vitamins, such as vitaminE , can cause ataxia.
Idiopathic Spinocerebellar ataxia-
In this type of ataxia, the cause of the disease is unknown.
Cerebellar ataxia associated with other diseases or secondary.
Some diseases, such as Parkinson's disease, multiple system atrophy, and Huntington's disease, can be associated with cerebellar ataxia.
Symptoms:
Symptoms of SCAcan vary, but some of the most common includes:
• Impaired motor coordination, especially in the limbs
• Gait disturbances, including limping and falling
• Speech problems, including stuttering and pronunciation disorders
• Swallowing problems
• Muscle weakness
• Numbness and tingling in the limbs
• Vision changes
• Cognitive problems
In our patient, who has examined, all the symptoms in detail, it can be said that he had most of these symptoms. Although the main key to the disease is gait and balance disorders and limping, speech problems, especially stuttering in certain languages, as well as pronunciation of difficult words or non-native languages, along with a significant decrease in muscle strength and swallowing problems, were more obvious than the other symptoms. However, no significant damage was seen in terms of vision problems or psychological.problems, as well as short-term or long-term memory. MMSE test =27 Especially since he can concentrate on a single subject for hours and even do significant research. The latest MRI of the brain, taken at the end of 2024, is attached and shows that no lesions are visible. (2)
Fig 1
Fig 2
Differences in symptoms in different types of SCA :
• Age of onset: Some types of SCA begin in childhood, while others begin in adulthood.
Fig 5
Characteristics of Vestibular, Cerebellar, and Sensory Ataxia. (6)
• varies in different types of SCA .
• Associated symptoms: Some types of SCA are associated with associated symptoms such as retinitis pigmentosa, diabetes insipidus, and cognitive impairment.
Examples of differences in symptoms across different types of SCA :
• SCA1: Usually characterized by cerebellar ataxia, dysarthria, and nystagmus.
• SCA3: In addition to common symptoms, it is associated with severe cerebellar atrophy and extrapyramidal motor disorders.
• SCA7: Associated with retinitis pigmentosa and diabetes insipidus.
The importance of accurately diagnosing the type of SCA :
Accurate diagnosis of SCA type is crucial for determining disease prognosis, genetic counseling, and selecting appropriate treatment MRI scan (sagittal and transverse T 1 -weighted image) of a 72-year-old woman with idiopathic late-onset cerebellar ataxia (ILOCA gradually progressive isolated cerebellar syndrome). Obvious atrophy of the cerebellar vermis, also of the brainstem (5)
Fig 3
Genetics:
To accurately diagnose the type of ataxia and identify its genetic cause, your doctor may order various genetic tests. The right test depends on the type of symptoms, family history, and other factors.
Here are some common genetic tests for diagnosing ataxia:
• PCR (Polymerase Chain Reaction) test: This test is used to detect specific gene mutations that cause certain types of ataxia, such as Friedreich's ataxia. This test looks for abnormal repeats in a specific section of DNA .
• Next-Generation Sequencing: This powerful method allows scientists to sequence the entire genome or exome (the protein-coding portion of the genome) simultaneously. This method is very useful for identifying unknown or rare gene mutations.
• Comparative Genomi Hybridization Array : This test is used to identify deletions, additions, or other large changes in chromosomes.
• Gene panel: This test is used to simultaneously examine several genes associated with ataxia.
Tables (Fig 5, 6 )
Genetic and Clinical Features of Hereditary Spinocerebellar Ataxias (7)
Names of some specific genetic tests for diagnosing ataxia:
• FXN gene test: to diagnose Friedreich's ataxia
• ATXN1 gene test: to diagnose spinocerebellar ataxia type 1
• ATXN3 gene test : to diagnose spinocerebellar ataxia type 3 (Machado-Joseph disease)
• ATXN8 gene test: to diagnose spinocerebellar ataxia type 8
ATXN8 is the name of a gene. Genes contain instructions that tell the body's cells how to make proteins. Proteins are important molecules that are essential for the body to function properly.
The doctors who have visited the patient are almost unanimous in their belief that he is genetically in the ATXN8 category . Why? Because of the set of clinical symptoms that have developed in the patient over time.
The mutation that causes SCA8 causes an over-repetition of a specific part of the gene. This duplication causes the ataxin-8 protein to be made in excess and to take on an abnormal shape. This abnormal protein accumulates in nerve cells and damages them. As a result, the nerve cells die and the symptoms of the disease appear.
But the reality is that these tests are not performed in our country, and the costs of performing them in European countries are very expensive for this patient's family, especially since they themselves know that the disease has no cure and that conservative treatments and monitoring of his condition are necessary. For this reason, genetic tests for this patient have been stopped for now.
Family history:
A family history of ataxia , if present , is very helpful in diagnosing genetic ataxia . However , when family history is absent or unknown , this It does not rule out a genetic cause . Common inheritance patterns include autosomal dominant (AD ) , recessive ( AR ) , and X-linked . Consanguinity between parents should alert the child to the possibility of an autosomal recessive disorder (3).
Complications:
consequences, and complications of spinocerebellar ataxia appear late and depend on the progression of the disease and the extent of involvement CNS -related . Most sub - groups of cerebellar spinal ataxias extend beyond the cerebellum and spinal cord. These include:
• Parkinsonism is caused by the associated neurodegeneration of dopaminergic neurons in the substantia nigra and is most commonly seen in SCA2 , and rarely in SCA3 and SCA17 . The progression of dystonia , tremor , and ataxic movement disorders associated with dystonia increases the severity of the disease . Dystonia One of the most common concomitant disorders is SCA .
• Depression , dementia and cognitive disorders Depression is a high -risk factor. It is the first term to affect the mental health concept of patients with neurological diseases including SCAs with impaired emotional functioning . Depressive symptoms are influenced by sexual and urinary dysfunction , personality disorder , and cognitive impairment . Cognitive impairment is mainly associated with SCA1 . Dementia was found in a case study in Japan that was associated with the end - stage SCA31 exists .
• Ocular complications Ocular motility disorders and retinopathy are common ocular features in SCA7 .. Central retinal degeneration involving the macula has been reported with subsequent peripheral spread . Therefore , central visual impairment and subsequent progressive visual loss can occur .
• Blepharospasm is a rare manifestation of SCA31. Abnormal saccadic movements and nystagmus are observed in a few cases.
• Dysphagia and dysarthria , degeneration of the motor nuclei in the brainstem that leads to:
difficulty swallowing and drooling , can be classified into the following SCA2 , SCA3 , SCA6 , and SCA7 were observed . Death from aspiration pneumonia is common in these patients .
• Seizures and Narcolepsy Pentanucleotide D - repeat expansion SCA10 increases your chances of epilepsy by 6 to 10 times . 01
Overall, the exact prevalence of petit mal and grand mal seizures in patients with spinal cervical ataxia SCA has not been precisely determined and may vary depending on the type of SCA , severity of the disease, and other factors.
It is difficult to determine the exact prevalence , partly due to the symptoms of epilepsy, partly due to the lack of studies or changes over time. Timely treatment can prevent complications from epilepsy. While there is a link between SCA and epilepsy, it is not possible to provide an exact figure for the prevalence of epilepsy in SCA patients. Each patient with SCA is unique and the likelihood of developing epilepsy depends on various factors.
Treatments for spinal cervical ataxia SCA:
Fortunately, with the advancement of science and research, important steps have been taken in recent years towards the treatment and management of spinal cervical ataxia SCA. Although there is still no definitive cure for this disease, new and innovative treatments are available that can help improve the quality of life of patients.
Drug treatments:
Disease-modifying drugs are being developed with the aim of influencing the mechanisms of the disease and slowing its progression.
Symptomatic drugs:
Drugs used to control symptoms such as tremors, muscle spasms, pain, and sleep disorders
Non-pharmacological treatments
Specialized exercise training helps improve balance, muscle strength, and motor coordination.
Occupational therapy:
Teaching daily living skills and using assistive devices to increase individual independence
Speech therapy:
Improving speech and swallowing problems
Proper nutrition:
A balanced, nutrient-rich diet to maintain overall health.
Complementary therapies:
Some complementary therapies, such as acupuncture and massage, may help reduce some symptoms, but more research is needed.
Innovative treatments
Gene therapy:
With the advancement of gene therapy technology, we hope that in the future it will be possible to cure disease by correcting defective genes.
Cell therapy:
Transplantation of stem cells or nerve cells can help repair damaged tissues.
Deep brain stimulation( D.B.S ):
This treatment helps control some symptoms by implanting electrodes in the brain and sending electrical pulses.
Fig 4
The impact of SCA on daily life: challenges and solutions
Main challenges
• Impaired motor coordination :
Difficulty performing delicate tasks such as writing, buttoning, and eating. This is particularly evident in the patient I have reported. These symptoms are so challenging that they would lead any neurologist to initially suspect Parkinson's disease, Parkinson's plus, or even PSP.
• Difficulty walking and maintaining balance:
Increased risk of falling and limited mobility
• Speech disorders :
Difficulty pronouncing words clearly, decreased voice volume, and difficulty swallowing.
• Muscle weakness:
Decreased muscle strength and premature fatigue
I can admit that all the signs and symptoms I have discussed above were very prominent in the patient I have prepared the report on.
• Emotional changes:
Depression, anxiety, and feelings of isolation .
• Social limitations :
Avoiding social activities due to fear of judgment and problems caused by the illness
But in the psychological aspect of the disease, which is very controversial for all patients with this history and especially the lack of sufficient prospects for getting rid of this disease, I would like to say in this regard that fortunately, due to the environment in which the patient was, the family's care, and especially the understanding of the patient and his problems, even if we do not have a perfect solution for his treatment at the moment, and especially the patient's own efforts are very important, so that this patient did not have any psychological problems at all. I remember well when I called him and his chiropractor to my office after the definitive diagnosis to discuss these challenges with him and encourage him to choose a new life with new challenges. I was interested to see that the patient was very, very far ahead. When I wanted to explain the importance of physiotherapy to him, his chiropractor said that one of our problems with him was that he wanted to do more than we said.
• Other challenges
Proper nutrition , the use of assistive devices such as canes, walkers, wheelchairs, and other assistive devices can help increase independence and safety. Some complementary therapies, such as acupuncture and massage, may help reduce some symptoms, but more research is needed.
Conclusion
Although cerebrospinal ataxia is very rare in the diagnosed population, given that there is no cure for this disease yet, and especially the genes that cause it are very diverse, it poses various challenges for therapists and, consequently, for patients. In particular, the fact that performing genetic tests, especially in poor countries, routinely faces financial obstacles, especially for families who are not very willing to perform these tests when they understand that definitive diagnosis of the disease gene type has no qualitative impact on the control and improvement of their patients. Or they do not have the financial strength to do so at all, and this issue is further compounded when countries cannot include it in diagnostic routines.
Therefore, paying attention to the patient's clinical condition, controlling the patient's clinical symptoms, and checking for disease progression, especially in old age, which deprives patients of their ability to move naturally, can lead to unpredictable accidents and, consequently, serious complications. Paying attention to the patient's psychological problems and possible challenges, especially in low-income groups, can provide patients with a balanced and almost tolerable lif.
Reference
1. Spinocerebellar Ataxia
Janis Bhandari; Pawan K. Thada; Debopam Samanta.
Author Information and Affiliations
Last Update: September 15, 2023.
2. A Brief Review on Spinocerebellar Ataxia and its Treatment
Rahul Singh Dhariyal1, VishwadeepakKimothi2*, Mohammad Asifb, MohdImran3
1Siddhartha Institute of Pharmacy, Near IT Park, Dehradun- 248001, Uttarakhand, India
2Department of Pharmacy, Himalayan Institute of Pharmacy Research, Dehradun, (Uttarakhand), 248007, India
3.Reprinted with permission from “Broca’s Area,” the newsletter of the Texas Neurological Society.Dr. Khemani is Assistant Professor, Clinical Center for Movement Disorders, Department of Neurology and Neurotherapeutics at University of Texas Southwestern Medical Center in Dallas, Texas
4.MedlinePlus links to health information from the National Institutes of Health and other federal government agencies
5. Textbook of Clinical Neurology 2018 editors:
J.B.M. Kuks
J.W. Snoek
6. Clinical Neurology, Tenth EditionRoger P. Simon
Michael J. Aminoff
David A. Greenberg
Copyright © 2018
7. First Aid for The Neurology Boards second edition 2015
MICHAEL S. RAFII, MD, PhD
Director, Memory Disorders Clinic Medical Director, Alzheimer’s Disease Cooperative Study Director, Neurology Residency Training Program Assistant Professor of Neurosciences University of California San Diego Health System La Jolla, California
THOMAS I. COCHRANE, MD, PhD Assistant Professor of Neurology Division of Neuromuscular Disease
Department of Neurology Harvard Medical School Brigham and Women’s Hospital Boston, Massachusetts
SERIES EDITOR:
TAO LE, MD, MHS Assistant Clinical Professor of Medicine and Pediatrics Chief, Section of Allergy and Immunology Department of Medicine University of Louisville
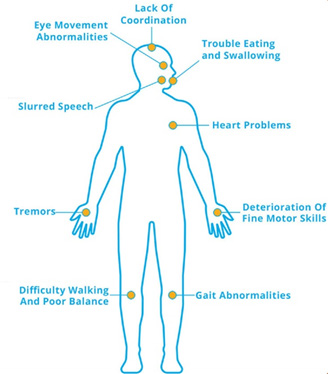
Figure 1
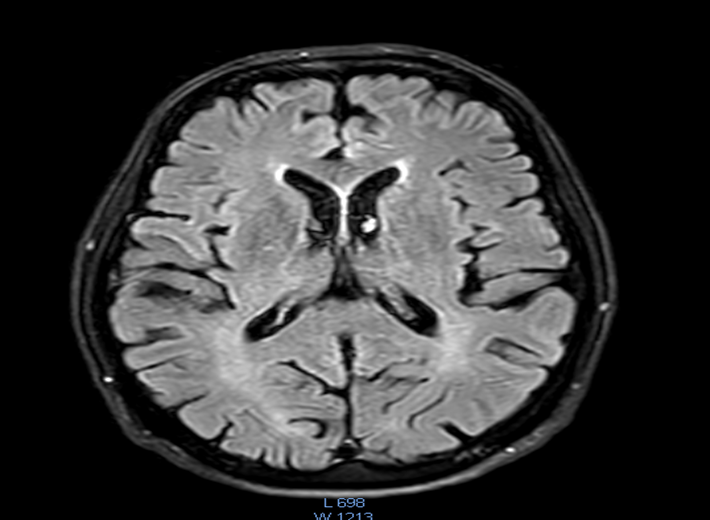
Figure 2
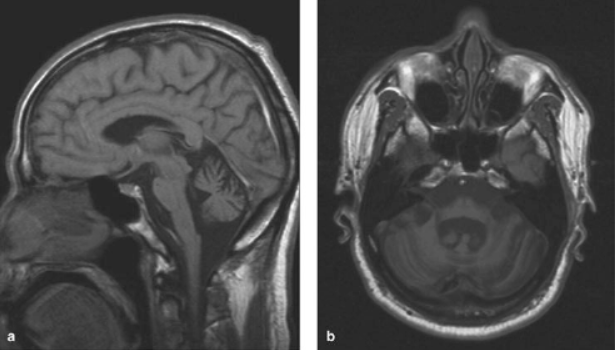
Figure 3

Figure 4
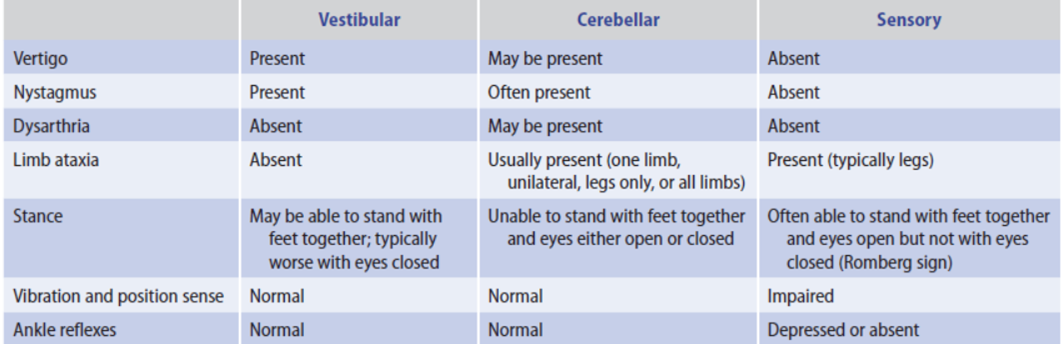
Figure 5
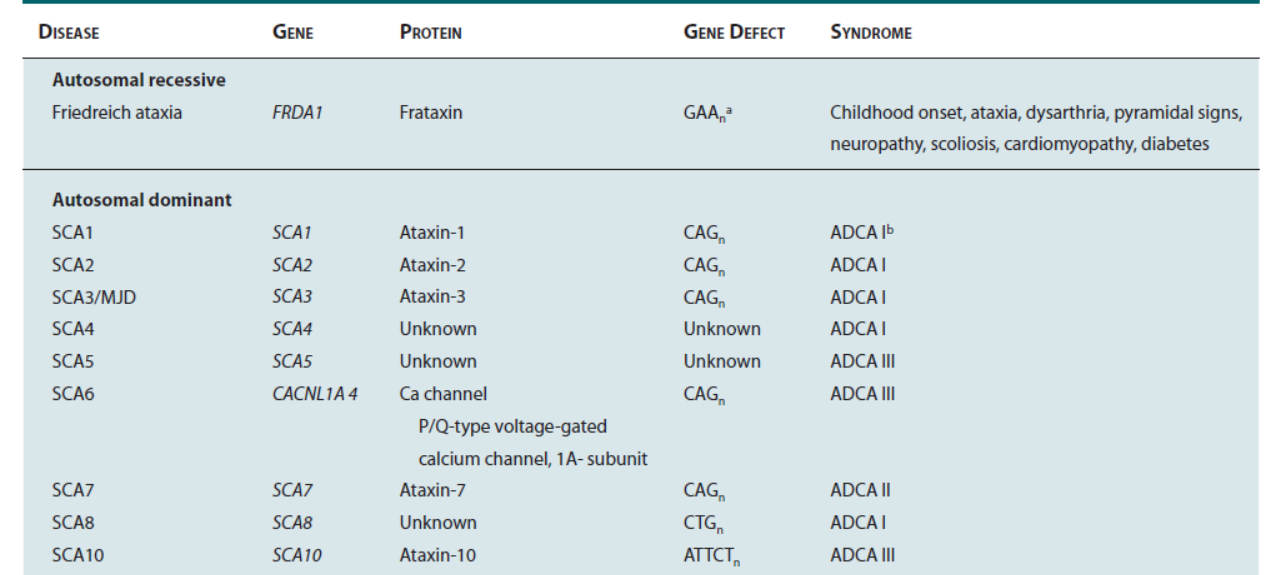
Figure 6
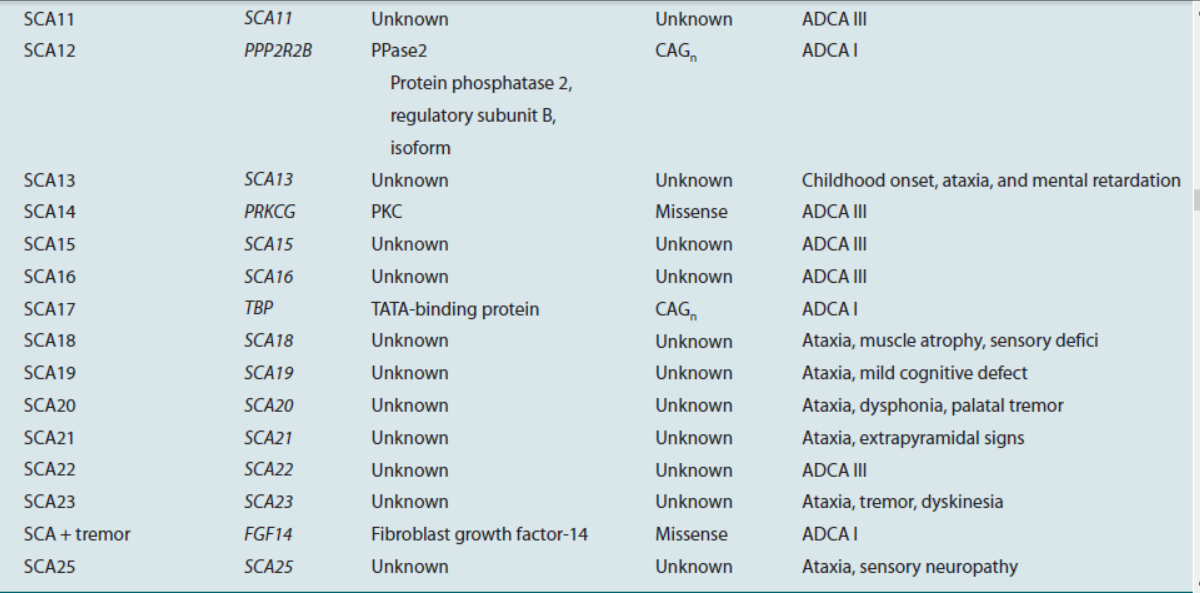
Figure 7