An Uncommon Presentation of Sarcoidosis: Disparate Brain, Breast, and Gastric Lesions – A Complex Case Report.
An Uncommon Presentation of Sarcoidosis: Disparate Brain, Breast, and Gastric Lesions – A Complex Case Report.
Dr Praneet Singh Bedi1, Dr Maheboob Hussain Shaik1*
1. Deparment of medical oncology, Max Super specality hospital, Delhi, India.
*Correspondence to: Dr Maheboob Hussain Shaik, Deparment of medical oncology, Max Super specality hospital, Delhi, India.
Copyright.
© 2025 Dr Maheboob Hussain Shaik This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 14 March 2025
Published: 20 March 2025
DOI:https://doi.org/10.5281/zenodo.15781974
Abstract:
Sarcoidosis is a multisystem granulomatous disease that can present with a wide spectrum of clinical manifestations. Rarely, it can involve organs such as the breast, stomach, and brain, often masquerading as malignancy. This case report describes an exceptionally rare presentation of sarcoidosis involving bilateral breast lesions, a dural-based brain lesion, gastric antral thickening, and widespread lymphadenopathy in a 55-year-old postmenopausal woman. The diagnosis was initially prompted by incidental hypercalcemia during a routine health checkup. Comprehensive evaluations, including histopathology, imaging, and laboratory studies, confirmed systemic sarcoidosis complicated by concurrent fibroadenomas, meningioma, and focal gastritis. This case underscores the importance of considering sarcoidosis in patients with atypical multisystem presentations and highlights the critical role of a multidisciplinary approach in diagnosis and management. The report also emphasizes the diagnostic challenges posed by overlapping pathologies and the need for meticulous evaluation to avoid misdiagnosis.
Keywords: Sarcoidosis, Breast lesion, Gastric lesion, Brain lesion, Malignancy mimic, non-caseating granulomas, Cervical lymph node biopsy.
An Uncommon Presentation of Sarcoidosis: Disparate Brain, Breast, and Gastric Lesions – A Complex Case Report.
Introduction
Sarcoidosis is a chronic, multisystem granulomatous disease characterized by the formation of noncaseating granulomas. While pulmonary involvement is the hallmark of the disease, affecting over 90% of patients, extrapulmonary manifestations can occur in virtually any organ system, including the skin, eyes, heart, liver, spleen, and nervous system.¹ However, simultaneous involvement of the breast, central nervous system (CNS), and gastrointestinal (GI) tract in the same patient is exceedingly rare.²
This case report presents a unique and complex presentation of sarcoidosis, involving disparate organ systems, and aims to highlight the diagnostic challenges and management strategies in such scenarios. The case also serves as a reminder of the importance of maintaining a broad differential diagnosis when evaluating patients with multisystem involvement, particularly when initial findings are nonspecific or overlapping with other conditions.
Case Presentation
Patient Profile:
A 55-year-old postmenopausal woman presented to the clinic for a routine health checkup. She reported no significant symptoms aside from occasional fatigue, which she attributed to aging. She had no history of smoking, alcohol use, or significant family medical history.
Initial Findings:
Hypercalcemia: Routine blood work revealed elevated serum calcium levels (11.2–11.8 mg/dL; reference range: 8.5–10.2 mg/dL), prompting further investigation.
Generalised Lymphadenopathy: Physical examination and imaging identified enlarged lymph nodes in the cervical, mediastinal, and abdominal regions. A biopsy of the cervical lymph nodes revealed noncaseating granulomas, raising suspicion for sarcoidosis. ³ (Fig.1.1)
Breast Lesions: Mammography (Fig.2.1) and ultrasound identified bilateral breast lesions. A BIRADS IV lesion in the left breast was excised and confirmed as a benign fibroadenoma (Fig.1.2) on histopathology.
Brain Lesion: Magnetic resonance imaging (MRI) of the brain revealed a 10 × 10 mm dural-based lesion in the left frontal cortex, consistent with a meningioma. ? (Fig.2.2)
Gastrointestinal Involvement: Upper gastrointestinal endoscopy (UGIE) demonstrated gastric antral thickening, and biopsy revealed focal active gastritis without evidence of Helicobacter pylori infection or malignancy. ? (Fig.1.3)
Laboratory Results
Elevated angiotensin-converting enzyme (ACE) levels: 40.10 U/L (reference range: 8–52 U/L).?
Polyclonal hypergammaglobulinemia.
Negative Mantoux test, ruling out tuberculosis.
Histopathological Confirmation
Cervical Lymph Node Biopsy: Noncaseating granulomas consistent with sarcoidosis. ³ (Fig.1.1)
Breast Lesion Excision: Histopathology confirmed fibroadenoma without evidence of malignancy. (Fig.1.2)
Gastric Biopsy: Focal active gastritis without granulomas or neoplasia. ? (Fig.1.3)
Imaging Studies
PET-CT Scan: Demonstrated FDG-avid lesions in the stomach, lymph nodes, and a subdural-based nodule in the brain. ?
MRI Brain: Confirmed a 10 × 10 mm dural-based lesion in the left frontal cortex, suggestive of a meningioma.? (Fig 2.1)
MRI Breast : Identified bilateral breast lesions, classified as BIRADS II and III, consistent with benign findings. (Fig 2.2)
Fig 1.1: H&E stain reveals noncaseating granulomas, a histopathological feature consistent with sarcoidosis.
Fig 1.2: Fibroadenoma (H&E, 20x): shows uniformly low stromal cellularity with no signs of stromal cellular atypia.
Fig 1.3: Focal active gastritis without granulomas or neoplasia
Fig 2.1: The mammogram reveals a well-defined, dense mass, BIRADS IV A lesion
Fig 2.2: A10 × 10 mm dural-based lesion in the left frontal cortex.
Fig 2.3: CE MRI breasts
Discussion
Sarcoidosis is a multisystem granulomatous disease of unknown etiology, characterized by the formation of non-caseating granulomas in various organs. While it primarily affects the lungs and lymphatic system, it can involve almost any organ, including the skin, eyes, heart, and nervous system. The disease has a variable clinical course, ranging from asymptomatic cases to severe organ dysfunction.
Epidemiology
Sarcoidosis has a worldwide distribution but is more common in certain populations. It is frequently diagnosed in young to middle-aged adults, with a peak incidence between 20 and 40 years. There is a higher prevalence in African American individuals and Northern Europeans, with some evidence suggesting a genetic predisposition.
Pathophysiology
The pathogenesis of sarcoidosis remains unclear, though it is believed to result from an exaggerated immune response to unidentified environmental antigens in genetically susceptible individuals. Activated CD4+ T cells and macrophages drive the formation of non-caseating granulomas, leading to inflammation and fibrosis in affected organs. Key cytokines, such as tumor necrosis factor-alpha (TNF-α) and interleukins (IL-2, IL-12, and IL-18), play a crucial role in granuloma formation.
Clinical Manifestations
Symptoms of sarcoidosis vary depending on organ involvement:
• Pulmonary Sarcoidosis (90% of cases): Dry cough, dyspnea, chest pain, and bilateral hilar lymphadenopathy on imaging.
• Cutaneous Involvement: Lupus pernio (violaceous plaques on the face), erythema nodosum, and maculopapular rashes.
• Ocular Sarcoidosis: Uveitis, conjunctivitis, and keratoconjunctivitis sicca.
• Cardiac Sarcoidosis: Conduction abnormalities (heart block, arrhythmias), cardiomyopathy, and sudden cardiac death.
• Neurosarcoidosis: Cranial neuropathies (especially facial nerve palsy), meningitis, myelopathy, and peripheral neuropathy.
• Hypercalcemia: Due to increased 1α-hydroxylase activity in macrophages, leading to increased vitamin D activation.
Diagnosis
Diagnosis is based on clinical presentation, imaging, histopathology, and exclusion of other granulomatous diseases (e.g., tuberculosis, fungal infections, lymphoma). Key diagnostic steps include:
• Chest X-ray/HRCT: Bilateral hilar lymphadenopathy and parenchymal infiltrates.
• Serum Markers: Elevated serum ACE (angiotensin-converting enzyme), hypercalcemia, and increased soluble IL-2 receptor levels.
• Bronchoalveolar Lavage (BAL): CD4/CD8 ratio >3.5 suggests sarcoidosis.
• Biopsy: Non-caseating granulomas on histopathology confirm the diagnosis.
Treatment and Management
Not all patients require treatment, as sarcoidosis can resolve spontaneously. For symptomatic or organ-threatening disease, the mainstay of treatment includes:
• Corticosteroids: First-line therapy (e.g., prednisone 20–40 mg/day) for pulmonary and systemic involvement.
• Immunosuppressive Agents: Methotrexate, azathioprine, or mycophenolate mofetil for steroid-sparing effects.
• Biologic Therapy: TNF-α inhibitors (infliximab, adalimumab) in refractory cases.
• Symptomatic Management: Calcium and vitamin D restriction in hypercalcemia, anti-arrhythmic drugs for cardiac involvement.
Gastrointestinal Involvement
Gastrointestinal involvement in sarcoidosis is rare, occurring in less than 1% of cases. The liver and spleen are the most commonly affected abdominal organs, often presenting asymptomatically. Symptomatic hepatic sarcoidosis may manifest as hepatomegaly, elevated liver enzymes, or intrahepatic cholestasis, while splenic involvement can lead to nonspecific systemic symptoms such as fatigue, fever, and weight loss. ?
Breast and CNS Involvement
Breast involvement in sarcoidosis is exceedingly rare, with most cases presenting as palpable masses or imaging abnormalities. ? CNS involvement, particularly dural-based lesions, is also uncommon and can mimic other pathologies such as meningiomas. ? the coexistence of these manifestations in the same patient poses significant diagnostic challenges, necessitating a thorough and systematic approach.
Diagnostic Challenges
The concurrent presentation of breast, brain, and gastric lesions in this patient complicated the diagnostic process. Hypercalcemia and systemic lymphadenopathy were key clues that directed investigations toward a systemic granulomatous disorder. Histopathological confirmation of noncaseating granulomas in the cervical lymph node biopsy was pivotal in establishing the diagnosis of sarcoidosis.³
Management Strategies
A multidisciplinary team comprising oncologists, endocrinologists, pulmonologists, and radiologists was essential for managing this complex case. Corticosteroids were initiated as first-line therapy to suppress granulomatous inflammation, while hydroxychloroquine was added to enhance disease control.? Supportive therapies included treatment for osteoporosis and vitamin D deficiency, which are commonly associated with sarcoidosis and its management.¹?
Prognosis and Follow-Up
The patient demonstrated significant clinical and biochemical improvement following corticosteroid therapy, with normalization of serum calcium levels and reduction in inflammatory markers. Long-term follow-up, including periodic imaging and laboratory evaluations, was planned to monitor disease progression and prevent systemic complications.?
Conclusion
This case highlights the diagnostic and therapeutic challenges of atypical and multisystem sarcoidosis, involving rare sites such as the breast, CNS, and stomach. It underscores the importance of maintaining a broad differential diagnosis and employing a systematic, multidisciplinary approach to accurately identify and manage complex cases of sarcoidosis. Early diagnosis and appropriate treatment are crucial for optimizing outcomes and preventing long-term complications.
Acknowledgments
The authors acknowledge the contributions of the multidisciplinary team involved in the care of this patient, including the radiology, pathology, and endocrinology departments.
Conflicts of Interest
The authors declare no conflicts of interest.
Funding:
No external funding was used for this case report.
References
1. Iannuzzi MC, Rybicki BA, Teirstein AS. Sarcoidosis. N Engl J Med. 2007;357(21):2153-2165.
2. Valeyre D, Prasse A, Nunes H, et al. Sarcoidosis. Lancet. 2014;383(9923):1155-1167.
3. Zhou Y, Lower EE, Li H, et al. Clinical manifestations of sarcoidosis in extrapulmonary sites. Clin Chest Med. 2015;36(4):631-646.
4. Krumholz A, Stern BJ. Neurologic manifestations of sarcoidosis. Handb Clin Neurol. 2014;119:305-333.
5. Kennedy MP, Sharma OP. Gastrointestinal and hepatic manifestations of sarcoidosis. J Clin Gastroenterol. 2006;40(9):810-816.
6. Baughman RP, Lower EE, du Bois RM. Sarcoidosis. Lancet. 2003;361(9363):1111-1118.
7. Shorr AF, Hnatiuk OW. Sarcoidosis presenting as isolated splenic involvement. South Med J. 2000;93(10):1008-1010.
8. Sabate JM, Clotet M, Torrubia S, et al. Radiologic evaluation of breast disorders related to pregnancy and lactation.Radiographics. 2007;27(Suppl 1):S101-S124.
9. Bickett AN, Funsch KM, Wu S, et al. Multidisciplinary management of sarcoidosis: Challenges and solutions. Ther Clin Risk Manag.2017;13:1761-1773.
10. Judson MA. Corticosteroids in sarcoidosis. Rheum Dis Clin North Am. 2016;42(1):119-135.

Figure 1
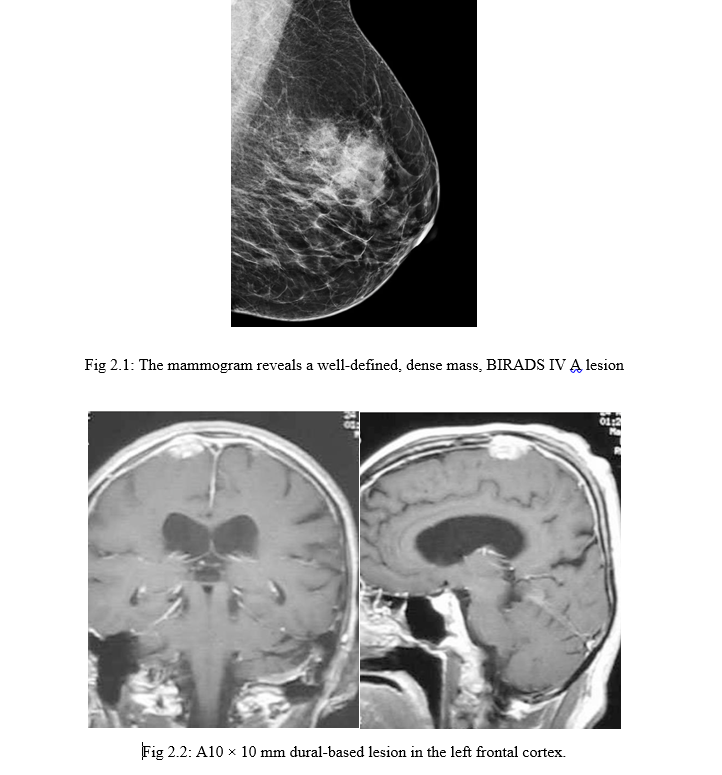
Figure 2

Figure 3