Idiopathic Granulomatous Mastitis Case Report In A Male Patient
Idiopathic Granulomatous Mastitis
Case Report In A Male Patient
Dr. Hamid Esmaeilpour *1
1 Dr. Hamid Esmaeilpour General surgeon, Dar Al Kamal hospital Sharjah. U.A.E.
*Correspondence to: Dr. Hamid Esmaeilpour, General surgeon, UAE.
Copyright
© 2025 Dr. Hamid Esmaeilpour. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 01 April 2025
Published: 17 April 2025
ABSTRACT:
Idiopathic granulomatous mastitis is a benign chronic inflammatory condition of the breast, the etiology of which has not been identified yet; it mimics two common breast disorders: breast carcinoma and tuberculous mastitis. Hence, this clinical entity poses difficulties in the diagnostic work-up. As clinical presentation and imaging findings often simulate other infectious and neoplastic etiologies, an accurate and early diagnosis is crucial to prevent misdiagnosis. Clear guidelines have yet to be established regarding treatment. In this report, we describe a case in which a patient presented with a painful breast abscess and was diagnosed with idiopathic granulomatous mastitis after histological evaluation. We managed this patient with a combination of surgical excision and, subsequently, a course of antibiotics and corticosteroid. To conclude, idiopathic granulomatous mastitis must be considered a possible differential while treating a patient with a abscess in the breast tissue.
Keywords: breast pathology, breast abscess, suppurative breast lesion, tuberculous mastitis, breast cancer, mastitis, idiopathic granulomatous mastitis.
Idiopathic Granulomatous Mastitis Case Report In A Male Patient
Introduction
Idiopathic granulomatous mastitis is a rare but benign chronic inflammatory condition of the breast that often affects women of childbearing age. Several factors have been identified as risk factors for idiopathic granulomatous mastitis such as oral contraceptive pills (OCPs), autoimmunity, infectious agents, and spillage of milk from the breast lobules. Moreover, pregnancy, breastfeeding, hyperprolactinemia, and Alpha-1 antitrypsin deficiency have been associated with the risk of the development of idiopathic granulomatous mastitis. The disease mainly presents as a hard lump that grows over time. Other presentations can be local pain, inflammation, tumorous induration, skin ulceration, fistula formation, and nipple retraction. These presentations resemble cancer so early diagnosis and treatment are vitally important, especially to differentiate it from breast cancer of inflammatory variant. There is no pathognomonic feature on USG, mammography, and MRI. The disease is diagnosed on histological sections showing non-caseating granulomas, and in most of the cases, this is a diagnosis of exclusion. As the name indicates, it is of an idiopathic etiology, therefore it poses a great dilemma in its treatment. Thus, there is no single well-established definitive cure or therapeutic strategy. However, a review of the literature reveals that surgical wide excision, corticosteroid therapy, colchicine, methotrexate, and azathioprine can be used for its treatment. In this case report, we described a male patient, suffering from idiopathic granulomatous mastitis for many weeks. His disease remained undiagnosed for a considerably long period despite seeking healthcare advice. This resulted in prolonged physical, mental, and economic burdens on the patient because delayed diagnosis hampered the initiation of optimal therapy. Hence, the purpose of reporting this case is to educate and raise awareness among practicing physicians regarding this rare clinical entity. Thus, we can avoid unnecessary mastectomies, which are still being reported. This disease is very rare in men and since 2013 till now only few cases (around 21 cases) reported,
Case presentation
The patient was a 50 years old man who was referred to me with secreting blood and pus from the left breast with severe pain.
HISTORY:
The patient was at first referred to hospital eleven years ago with these symptoms and had been drained and given antibiotics with diagnosis of breast abscess. Since then, four more times found with same symptoms and treated the same. Never touched the crisp and underneath the biopsy at the same time. Cystic fluid from his breast was aspirated, and the bacterial culture test showed no growth of any microorganisms after 48 hours. The cytology revealed predominantly neutrophils and degenerating cells in a hemorrhagic background, which suggested an acute suppurative inflammatory process of the affected breast as shown in Figure 2.
Figure 2. Histopathological findings of acute mastitis demonstrating areas of acute inflammation. Polymorphonuclear cells seen in acute inflammation are depicted by an unfilled blue arrow.
Figure 3. Ultrasonography of the breast showing an ill-demarcated hypoechoic irregular lesion with no fluid components. The area of pathology is marked by a solid red arrow.
Figure 4
The repeated cytological examination also showed cellular clusters comprising histiocytes and epithelioid-like cells. Hence, based on these findings, the treating physician concluded that the ongoing clinical picture was more suggestive of tuberculosis of the breast. Therefore, after discussing with the patient, a therapeutic trial of an anti-tuberculosis therapy (ATT) was prescribed for four weeks. However, instead of any clinical improvement, her condition worsened over time and she had to visit her physician again just after three weeks. Her re-assessment by sonomammography was performed, which indicated an ill-demarcated hypoechoic irregular lesion, measuring 44.7×35.4 millimeters in the outer lower and adjoining upper quadrants of the right breast with thin fluid streaks as shown in Figure 4.
The sonologist concluded that these findings were consistent with an infectious or inflammatory lesion. Afterward, the primary care physician referred her to a teaching hospital for a surgical consult. So, re-evaluation of the patient was performed by a detailed history, thorough general physical examination, and routine laboratory investigations. It was then planned to perform incision and drainage of pus collection and excisional tissue biopsy after surgical resection of the mass. The excisional biopsy material was sent for histopathology and pussy discharge for acid-fast bacilli (AFB) smear. After surgery, she received broad-spectrum antibiotics (ceftriaxone and moxifloxacin) for two weeks. The subsequent histopathology showed areas of acute and chronic inflammation along with predominant lobulocentric granulomatous inflammation as shown in Figure 5.
Discussion
Idiopathic granulomatous mastitis is an uncommon pathological process involving breast tissue. Owing to the variety and non-specificity in the spectrum of clinical manifestations, this disease has been quite a diagnostic challenge for healthcare professionals. Therefore, many a time this debilitating condition remains undiagnosed or misdiagnosed, causing unnecessary investigations and procedures. This puts patients at risk of functional impairment along with an economic burden. The current case was initially diagnosed as acute mastitis with an underlying breast abscess and afterward, it was falsely labeled as tuberculosis of the breast. It is noteworthy that these conditions are among common differential diagnoses of idiopathic granulomatous mastitis. During the early course of the disease, the patient received antibiotics and antituberculosis therapy (ATT), which is similar to the findings of a detailed study by Mahmoodlou R et al. in which two out of 46 patients had ATT as part of the management [2]. It is worthy to note that this patient belonged to the tuberculosis (TB) endemic region, so an anchoring bias might have played a role in the misdiagnosis of breast TB. In addition to it, Seo HR et al. have studied the differentiating features between TB of breast and idiopathic granulomatous mastitis [6]. This study found statistically significant clinical differences between the breast TB and idiopathic granulomatous mastitis patient groups. These differentiating features include older age in breast TB as compared to idiopathic granulomatous mastitis (40 vs 33.5 years, p =.018), more frequent axillary lymphadenopathy in the tuberculous mastitis group (50% vs 20.6%, p =.048), and a history of tuberculosis of lungs in patients with tuberculosis of breast [6]. Interestingly, our case also presented in the younger age group and did not have axillary lymphadenopathy. Moreover, the absence of lymphocytosis on complete blood count (CBC) was against the diagnosis of tuberculosis.
Establishing the diagnosis of idiopathic granulomatous mastitis is a complex and laborious task that involves a series of investigations. The ultrasonography of the breast proved its significance and accuracy in the workup of this complicated and rare clinical entity. A study by Hasbahcec M et al. revealed that a hypo-echoic or heterogeneous mass with or without tubular extensions is the most frequent finding on sonomammography of the breast. This study concluded that, in the case of an inflammatory lesion in the breast, heterogeneity of the breast parenchyma and abscess formation was likely to be the cardinal features of idiopathic granulomatous mastitis [7]. These radiological features are also consistent with the sonomammography findings of our patient.
Regarding treatment, our patient showed a dramatic response to high-dose corticosteroids (prednisolone). This supports the findings of a previous research study, emphasizing a higher success rate with lower recurrences by using high-dose steroids [8]. It is also proposed that steroids possibly reduce the need for surgery [9]. Hence, Montazer M et al. reported that the patients who received a high dose of corticosteroids had a significantly higher rate of remission compared to the patients who received a low dose of corticosteroids (93.3% vs. 53.3%, p=0.03) [8]. Interestingly, among patients with remission, recurrence was also significantly lower in the high dose compared to low dose prednisolone (0% vs. 37.5%, p=0.04) [8].
Therefore, systemic corticosteroids and antibiotics are the most frequently used agents in the medical treatment of idiopathic granulomatous mastitis. However, immunosuppressant agents such as methotrexate and azathioprine can also be used for the management of idiopathic granulomatous mastitis. Furthermore, we can opt for a therapeutic trial of bromocriptine and anti-inflammatory agents (colchicine) in combination with steroids [10-11]. In cases, where medical management fails, surgical intervention should be the next best step. This includes abscess drainage, local and wide excisions, or even mastectomy when there is no significant remission after a long time of conservative management [12].
Conclusions
Idiopathic granulomatous mastitis is an exceedingly rare pathology of breast tissue. Owing to non-specific and ambiguous clinical features, it can remain undiagnosed or misdiagnosed, which leads to an undue delay in the initiation of treatment. The sonomammography of the breast is the cornerstone of its diagnostic work-up. In case of an inflammatory lesion of the breast, a hypoechoic or heterogeneous mass with or without tubular extensions on sonomammography should raise the suspicion of idiopathic granulomatous mastitis.
References
1.Idiopathic granulomatous mastitis: challenges of treatment in Iranian women. Shojaee L, Rahmani N, Moradi S, Motamedi A, Godazandeh G. BMC Surg. 2021;21:206. doi: 10.1186/s12893-021-01210-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
2.Idiopathic granulomatous mastitis: dilemmas in diagnosis and treatment. Mahmodlou R, Dadkhah N, Abbasi F, Nasiri J, Valizadeh R. Electron Physician. 2017;9:5375–5379. doi: 10.19082/5375. [DOI] [PMC free article] [PubMed] [Google Scholar]
3.Idiopathic granulomatous mastitis-a mystery yet to be unraveled: a case series and review of literature. Mathew Thomas V, Alexander SA, Bindal P, Vredenburgh J. Cureus. 2020;12:0. doi: 10.7759/cureus.6895. [DOI] [PMC free article] [PubMed] [Google Scholar]
4.Idiopathic granulomatous mastitis: an institutional experience. Prasad S, Jaiprakash P, Dave A, Pai D. Turk J Surg. 2017;33:100–103. doi: 10.5152/turkjsurg.2017.3439. [DOI] [PMC free article] [PubMed] [Google Scholar]
5.Idiopathic granulomatous mastitis: time to avoid unnecessary mastectomies. Bani-Hani KE, Yaghan RJ, Matalka II, Shatnawi NJ. Breast J. 2004;10:318–322. doi: 10.1111/j.1075-122X.2004.21336.x. [DOI] [PubMed] [Google Scholar]
6.Differential diagnosis in idiopathic granulomatous mastitis and tuberculous mastitis. Seo HR, Na KY, Yim HE, et al. J Breast Cancer. 2012;15:111–118. doi: 10.4048/jbc.2012.15.1.111. [DOI] [PMC free article] [PubMed] [Google Scholar]
7.Use of imaging for the diagnosis of idiopathic granulomatous mastitis: a clinician's perspective. Hasbahceci M, Kadioglu H. J Coll Physicians Surg Pak. 2018;28:862–867. doi: 10.29271/jcpsp.2018.11.862. [DOI] [PubMed] [Google Scholar]
8.Comparison of the outcome of low dose and high-dose corticosteroid in the treatment of idiopathic granulomatous mastitis. Montazer M, Dadashzadeh M, Moosavi Toomatari SE. Asian Pac J Cancer Prev. 2020;21:993–996. doi: 10.31557/APJCP.2020.21.4.993. [DOI] [PMC free article] [PubMed] [Google Scholar]
9.Factors related to recurrence of idiopathic granulomatous mastitis: what do we learn from a multicentre study? Uysal E, Soran A, Sezgin E. ANZ J Surg. 2018;88:635–639. doi: 10.1111/ans.14115. [DOI] [PubMed] [Google Scholar]
10.Long-term outcome in idiopathic granulomatous mastitis: a western multicentre study. Néel A, Hello M, Cottereau A, et al. QJM. 2013;106:433–441. doi: 10.1093/qjmed/hct040. [DOI] [PubMed] [Google Scholar]
11.Methotrexate in the management of idiopathic granulomatous mastitis: review of 108 published cases and report of four cases. Akbulut S, Yilmaz D, Bakir S. Breast J. 2011;17:661–668. doi: 10.1111/j.1524-4741.2011.01162.x. [DOI] [PubMed] [Google Scholar]
12.Idiopathic granulomatous mastitis: comparison of wide local excision with or without corticosteroid therapy. Akcan A, Oz AB, Dogan S, et al. Breast Care (Basel) 2014;9:111–115. doi: 10.1159/000360926. [DOI] [PMC free article] [PubMed] [Google Scholar].
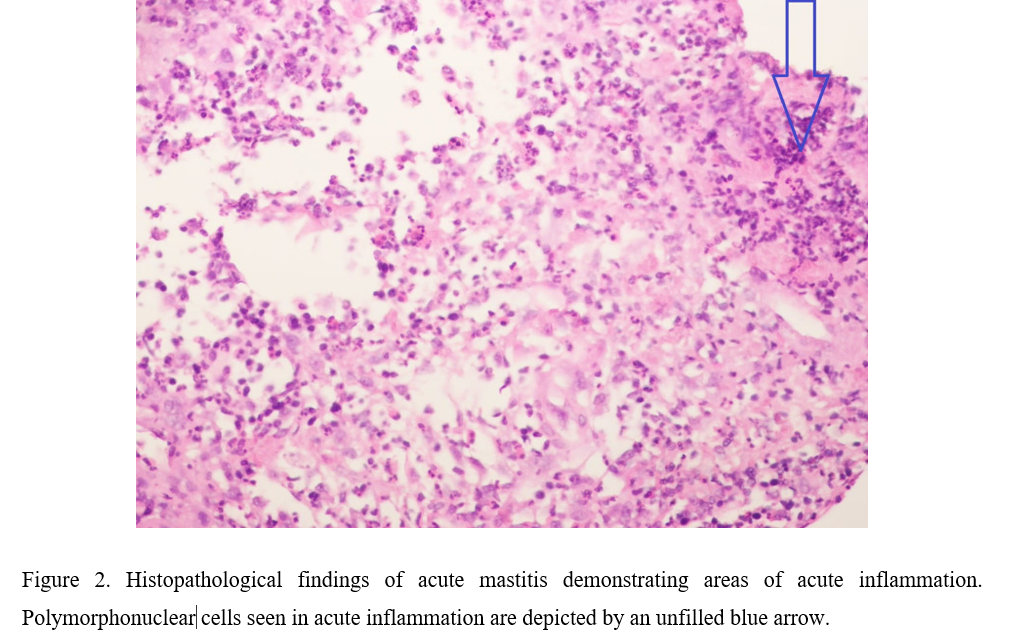
Figure 1

Figure 2