Current Status of Integrated Pharmacological and Interventional Treatment of Cancer Pain
Current Status of Integrated Pharmacological and Interventional Treatment of Cancer Pain
Melisa Hunis MD1*, Adrian Hunis MD2
*Correspondence to: Melisa Hunis MD, School of Medicine, Universidad de Buenos Aires (UBA), Argentina.
Copyright
© 2025 Melisa Hunis. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 07 May 2025
Published: 19 May 2025
Abstract
Background: Cancer pain is a complex, multifactorial syndrome that significantly impairs quality of life. Despite advances in oncology, pain remains undertreated.
Objective: To review the current pharmacological and interventional approaches to cancer pain, including epidemiology, assessment, types, and management strategies.
Methods: Literature review of recent guidelines, clinical trials, and meta-analyses.
Results: Effective cancer pain management requires a multimodal approach, integrating pharmacological, interventional, psychological, and physiotherapeutic strategies.
Conclusion: Despite progress, challenges remain in individualized pain control, opioid stewardship, and access to interventional therapies.
Current Status of Integrated Pharmacological and Interventional Treatment of Cancer Pain
Cancer Pain Syndrome
Cancer pain is defined as pain caused directly by tumor infiltration, cancer-related treatment, or associated complications. It is a multidimensional experience involving physical, emotional, and social components [1]. Cancer pain may be acute or chronic and is often persistent, with episodes of breakthrough pain.
Epidemiology, Frequency, and Tumor Types Most Associated with Pain
Cancer pain affects up to 70% of patients with advanced disease [2]. Prevalence varies by cancer type and stage (see Table 1).
Table 1. Prevalence of Pain by Cancer Type
Adapted from van den Beuken-van Everdingen et al. [2]
Pain is more frequent in advanced and metastatic stages, particularly with bone, pancreatic, and head and neck cancers [3].
D) Semiological Assessment and Pain Measurement
Accurate pain assessment is crucial. Key elements include:
- Location, intensity, quality, duration, and aggravating/relieving factors
- Impact on function and mood
Pain Measurement Tools:
- Visual Analog Scale (VAS)
- Numeric Rating Scale (NRS)
- Brief Pain Inventory (BPI)
- McGill Pain Questionnaire
Table 2. Common Pain Assessment Tools
Types of Cancer Pain
Cancer pain is heterogeneous:
- Visceral pain: Deep, poorly localized (e.g., liver metastases)
- Somatic (bone) pain: Well-localized, often severe (e.g., bone metastases)
- Neuropathic pain: Burning, shooting, due to nerve infiltration or treatment (e.g., chemotherapy-induced neuropathy)
- Breakthrough pain: Transient exacerbations despite baseline control
- Incident pain: Triggered by movement or procedures
- Refractory pain: Resistant to standard therapies
Pharmacological Treatment: Analgesic Ladder and Drug Classes
The WHO Analgesic Ladder remains the cornerstone (see Figure 1).
Figure 1. WHO Analgesic Ladder (Described):
- Step 1: Non-opioids (NSAIDs, acetaminophen)
- Step 2: Weak opioids (codeine, tramadol) ± non-opioids
- Step 3: Strong opioids (morphine, fentanyl) ± adjuvants
Table 3. Pharmacological Agents in Cancer Pain
Morphineis the gold standard for severe cancer pain [4].
Fentanyl patches are preferred in patients with swallowing difficulties or renal impairment [5].
Interventional Treatments
When pharmacological therapy is insufficient or limited by side effects, interventional procedures are considered.
Table 4. Interventional Techniques
Psychological Treatment
Psychological interventions are essential in comprehensive pain management. Techniques include:
- Cognitive-behavioral therapy (CBT)
- Relaxation training
- Mindfulness and coping strategies
- Supportive counseling
These approaches reduce pain perception, anxiety, and improve coping [6,7].
Physiotherapeutic Treatment
Physical therapy aims to maintain function, reduce pain, and improve quality of life:
- Exercise programs
- Manual therapy
- Transcutaneous electrical nerve stimulation (TENS)
- Heat/cold therapy
Physiotherapy is especially beneficial for musculoskeletal and neuropathic pain components [8].
Final Summary
Cancer pain is a prevalent, multifactorial syndrome requiring a multidisciplinary approach. Pharmacological management, based on the WHO ladder, remains foundational, but interventional, psychological, and physiotherapeutic modalities are critical adjuncts. Individualized treatment plans, regular assessment, and patient education optimize outcomes.
Future Directions in Cancer Pain Management
- Personalized medicine: Genetic profiling for opioid response [9]
- Novel analgesics: Peripherally acting opioids, cannabinoids [10]
- Neuromodulation: Spinal cord stimulation, dorsal root ganglion stimulation [11]
- Telemedicine: Remote pain assessment and management [12]
- Integration of palliative care: Early involvement improves pain and quality of life [13]
Conclusions
Optimal cancer pain management requires integration of pharmacological, interventional, psychological, and rehabilitative therapies. Ongoing research into novel agents and techniques, alongside improved access to interventional procedures and palliative care, will further enhance patient outcomes.
References
1. Portenoy RK, Lesage P. Management of cancer pain. Lancet. 1999;353(9165):1695-1700.
2. van den Beuken-van Everdingen MH, et al. Prevalence of pain in patients with cancer: a systematic review of the past 40 years. Ann Oncol. 2007;18(9):1437-1449.
3. Fallon M, et al. Cancer pain in Europe: a longitudinal study. Eur J Pain. 2018;22(3):533-540.
4. Caraceni A, et al. Use of opioid analgesics in the treatment of cancer pain: evidence-based recommendations. J Clin Oncol. 2012;30(5):623-631.
5. Mercadante S, et al. Fentanyl transdermal system for the treatment of cancer pain. J Pain Symptom Manage. 2001;21(2):102-109.
6. Syrjala KL, et al. Psychological approaches to cancer pain management. J Clin Oncol. 2014;32(16):1703-1711.
7. Bennett MI, et al. Psychological interventions for cancer pain. Cochrane Database Syst Rev. 2019;5:CD006275.
8. Oldenmenger WH, et al. Physical therapy for cancer pain: a systematic review. Pain Physician. 2018;21(6):541-558.
9. Lotsch J, Geisslinger G. Current evidence for a genetic modulation of the response to analgesics. Pain. 2006;121(1-2):1-5.
10. Fallon MT, et al. Cannabinoids for cancer pain: efficacy, safety, and pharmacology. Curr Opin Support Palliat Care. 2017;11(2):109-115.
11. Deer TR, et al. Neuromodulation for cancer pain and cachexia. Cancer J. 2013;19(5):403-410.
12. Watanabe SM, et al. Telemedicine for cancer pain management: a systematic review. J Telemed Telecare. 2014;20(6):276-282.
13. Temel JS, et al. Early palliative care for patients with metastatic non–small-cell lung cancer. N Engl J Med. 2010;363(8):733-742.
14. Bennett MI, et al. Neuropathic pain in cancer: mechanisms and treatment. Curr Opin Support Palliat Care. 2012;6(1):15-24.
15. Swarm RA, et al. Adult cancer pain: clinical practice guidelines in oncology. J Natl Compr Canc Netw. 2013;11(8):992-1022.
16. Paice JA, et al. Management of cancer pain: ESMO Clinical Practice Guidelines. Ann Oncol. 2018;29(Suppl 4):iv166-iv191.
17. Smith TJ, et al. American Society of Clinical Oncology provisional clinical opinion: the integration of palliative care into standard oncology care. J Clin Oncol. 2012;30(8):880-887.
18. Kwon JH. Overcoming barriers in cancer pain management. J Clin Oncol. 2014;32(16):1727-1733.
19. Schug SA, Chandrasena C. Pain management of the cancer patient. Expert Opin Pharmacother. 2015;16(1):5-15.
20. Vellucci R. Heterogeneity of chronic pain. Clin Drug Investig. 2012;32(Suppl 1):3-10..

Figure 1
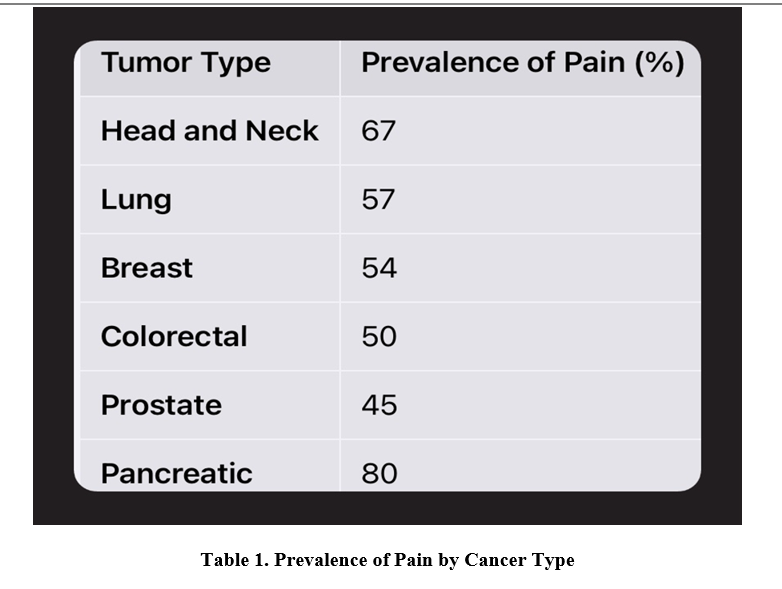
Figure 2
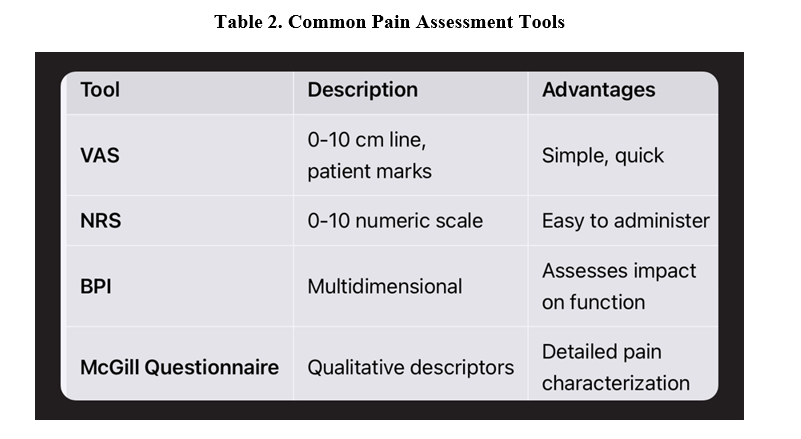
Figure 3
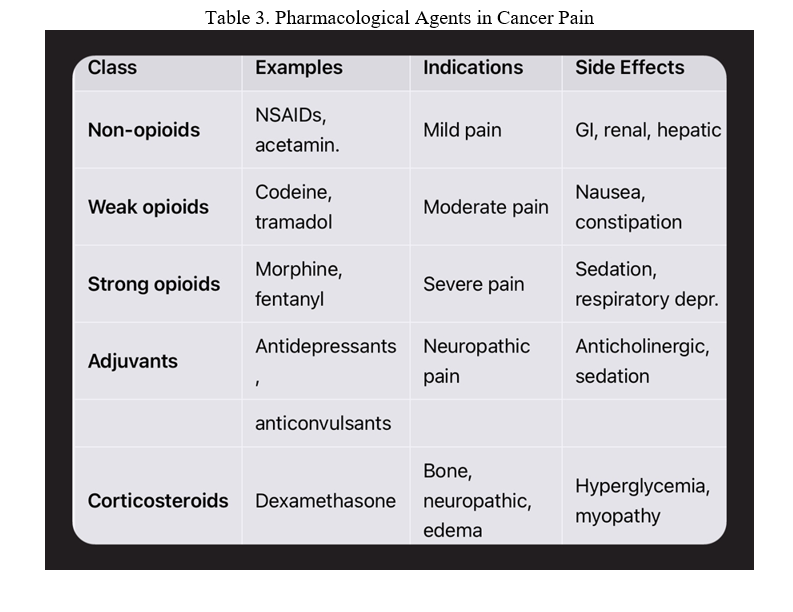
Figure 4
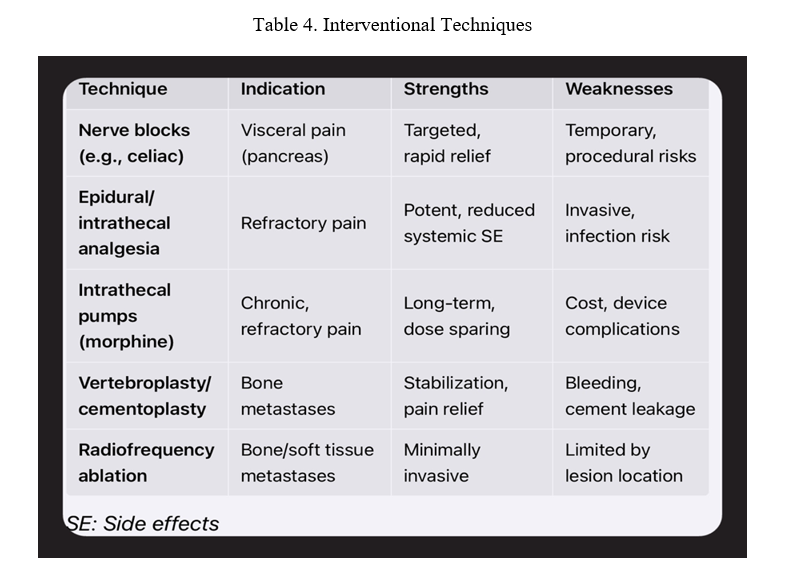
Figure 5