High Prevalence of Work-Related Musculoskeletal Disorders among Indian Orthopaedic Surgeons: A Nationwide Cross-Sectional Survey
High Prevalence of Work-Related Musculoskeletal Disorders among Indian Orthopaedic Surgeons: A Nationwide Cross-Sectional Survey
Udit Kumar Biswal1, Pooja Priyadarsini2, Sujith B.S.3, Kalpesh Saindane4, Raman Jindal4, Shilp Verma5
1. Department of Orthopaedics, IMS & SUM Hospital, Bhubaneswar, Odisha, India.
2. Department of Biochemistry, IMS & SUM Hospital, Bhubaneswar, Odisha, India.
3 Department of Orthopaedics, TNMC & BYL Nair Charitable Hospital, Mumbai, Maharashtra, India.
4 Department of Arthroplasty, Sparsh Hospital, Infantry Road, Bengaluru, Karnataka, India.
5 Department of Orthopaedics, AIIMS , Raipur, Chhatisgarh, India.
*Correspondence to: Dr. Udit Kumar Biswal, Assistant Professor, Department of Orthopaedics,IMS & SUM Hospital, Bhubaneswar, Odisha, India.
Copyright
© 2025 Dr. Udit Kumar Biswal is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 23 July 2025
Published: 01 August 2025
DOI: https://doi.org/10.5281/zenodo.16629767
Abstract
Background: Work-related musculoskeletal disorders (MSDs) are prevalent among orthopaedic surgeons due to physically demanding tasks, yet data from low- and middle-income countries like india are limited. This study estimates msd prevalence, identifies risk factors, and assesses ergonomic practices among indian orthopaedic surgeons.
Methods: A cross-sectional survey was conducted from march to may 2025 using a modified nordic musculoskeletal questionnaire. Practicing orthopaedic surgeons and residents with ≥6 months of surgical experience were recruited via professional networks. Data on demographics, work patterns, ergonomic practices, and msd symptoms were collected anonymously via google forms. Descriptive statistics, chi-square tests, and subgroup analyses were performed using ibm spss v25.
Results: Of 117 respondents, 104 (88.9% response rate) completed the survey (78% male, mean age 36.4 years). Msd prevalence was 82%, with lower back (58%), neck (47%), and shoulder (39%) pain most common. Surgeons with >30 operating theatre hours/week had higher lower back pain (p=0.02). Frequent lead apron use correlated with neck and shoulder pain (p=0.01). Only 34% were aware of ergonomic guidelines, and 18% used anti-fatigue mats.
Conclusions: Indian orthopaedic surgeons face a high msd burden, exacerbated by long operating hours, lead apron use, and limited ergonomic resources. Integrating ergonomic training into residency programs and improving workplace infrastructure are critical to enhance surgeon well-being and healthcare sustainability.
Keywords: Orthopaedic surgeons, musculoskeletal disorders, ergonomics, occupational health, india, nordic musculoskeletal questionnaire, cross-sectional survey, surgeon wellness.
High Prevalence of Work-Related Musculoskeletal Disorders among Indian Orthopaedic Surgeons: A Nationwide Cross-Sectional Survey
Introduction
Background
Musculoskeletal disorders (MSDs) are an important occupational health concern among health-care professionals, especially in surgical specialties such as orthopaedics. Orthopaedic surgeons experience unique biomechanical stressors as their profession is physically demanding in nature (1). Trauma surgeries, joint arthroplasties, and spinal stabilizations involve forceful movements, several times daily. Prolonged standing, poorly postured movement, and manipulation of heavy devices such as power drills, mallets and retractors make orthopaedic surgeons vulnerable to MSDs (1,2). Additionally, daily repeated usage of lead aprons for fluoroscopy guided procedures places considerable weight tension on the shoulders and neck (3). These pile up cumulative stress, resulting in localized discomfort, functional impairment, decreased surgical dexterity, psychological morbidity, and, most critically, a very real possibility of early career termination (1,4–6).
Global burden
In global evidence, extremely high prevalence of MSDs among surgeons has been demonstrated in United States, European, and East Asian studies at the rate of 60–90% across all surgical specialties (5,7,8). For example, in 2018, the American Academy of Orthopaedic Surgeons (AAOS) conducted a survey in which 67% of the respondents who were interviewed reported occupational pain, with the most frequent being lower back and neck pain.
Indian context
Such data may not necessarily reflect the picture in LMIC countries such as India, where surgeons are known to bear extended working hours, lack of ergonomic facilities (e.g., adjustable operation theater tables, anti-fatigue mats), and poor training in postural optimization. Cultural underreporting and avoidance of seeking medical help for pain further contributes to the issue, potentially hiding the true burden.
In India, orthopaedic surgeons function in varied environments ranging from poorly equipped yet volume-high public hospitals to private centers. The surge in demand for elective procedures such as joint replacements with a heavy trauma volume overwhelms surgeons with tremendous physical workload. In contrast to high-income environments where ergonomic equipment and automation (e.g., robotic surgery) are available, Indian surgeons default to manual methods, which leave them vulnerable to excessive repetitive strain and injuries (9). In addition, ergonomic education is not a usual part of surgical residency training and thus surgeons are poorly prepared to detect and minimise occupational trauma (2,10,11).
Rationale for the study
Notwithstanding the global focus on burnout and doctor wellness, comparatively little research has been conducted on MSDs among Indian orthopaedic surgeons. This void in research is critical, because surgeons' physical health directly affects patient safety, outcomes of surgery, and system sustainability. This research addresses this lacuna by estimating MSD prevalence and anatomical distribution, occupational risk factor identification, and ergonomics awareness and practice assessment among Indian residents and orthopaedic surgeons. By reporting region-specific evidence, we hope to inform evidence-based, focused interventions, such as policy modification, institutional ergonomic improvement, and education reform promoting a healthier and sustainable orthopaedic workforce.
Materials and Methods
Study Design
This cross-sectional observational descriptive study utilized an online survey spanning three months (March–May 2025). The study was approved by the Institutional Ethics Committee, with adherence to ethics guidelines for human research.
Participants and Inclusion Criteria
Participants were practicing orthopaedic surgeons and residents from India, contacted through professional networks such as email lists, WhatsApp and Telegram groups run by orthopaedic societies, and social media platforms. We included practicing orthopaedic surgeons or residents (trainees) with at least 6 months of surgical experience (to have adequate exposure to occupational stressors) who voluntarily participated in the study with digital informed consent. Surgeons in specialties other than orthopaedics (e.g., general surgeons, neurosurgeons) and those with incomplete, repeat or invalid responses to the survey were excluded.
Sample Size Calculation
To determine the prevalence of MSDs with 95% confidence levels and 10% margin of error, and assuming a conservative prevalence rate of 50% as per literature from global studies, a minimum sample size of 96 was estimated by applying the proportion estimation formula. Taking into account a 20% non-response rate as well, we planned to send the survey to a minimum of 120 potential respondents.
Survey Tool
The survey was created on Google Forms to be readily accessible and shareable. Pilot testing was done among 10 orthopaedic surgeons to check for ease of use and simplicity, and some changes were made post-feedback. The survey comprised five domains:
1. Demographics: Age, gender, designation (resident, consultant, academic, private practitioner), years of surgical practice, and practice region (urban/rural, state).
2. Work Profile: OT hours per week, procedure types (e.g., trauma, joint replacement, spine), intraoperative lead apron usage frequency, and most preferred surgical position (standing, sitting, or a combination of both).
3. Ergonomic Practices: Frequency of intraoperative use of ergonomic equipment (e.g., anti-fatigue mats, adjustable tables, stools), frequency of intraoperative breaks, and postural adjustment habit.
4. Musculoskeletal Symptoms: The original NMQ was adapted to suit the occupational context of orthopaedic surgeons (12,13). We retained the core structure assessing symptoms in nine anatomical regions (neck, shoulders, upper back, lower back, elbows, wrists/hands, hips/thighs, knees, and ankles/feet) over the past 12 months. Additional items were added to assess pain intensity, impact on surgical tasks, medical consultations sought, workdays lost due to MSDs, and consideration of career change due to symptoms. These additions provided a more comprehensive view of the professional impact of MSDs among surgeons. Internal consistency of the survey tool was not formally assessed in this study. However, the musculoskeletal symptoms section was based on the widely validated NMQ, which has demonstrated high reliability in previous occupational health studies.
Figure 1 : Modified Nordic Musculoskeletal Questionnaire (NMQ) used in our study
5. Ergonomic Awareness: Awareness of existing ergonomic guidelines for surgeons, previous training, and willingness to participate in future workshops.
Participants were explained the purpose of the study, anonymity, and voluntary nature of participation on an introductory page, and electronic consent was obtained prior to entry.
Data Collection
The questionnaire was sent via email invitations, professional group messaging, and posts on orthopaedic society boards. Biweekly reminders were sent to encourage an optimum level of response. Responses were taken anonymously, and no identifiable data were retained.
Statistical Analysis
Data were pulled from Google Forms into Microsoft Excel and analyzed with IBM SPSS v25. Descriptive statistics like frequency, percent, mean, and standard deviation were calculated for demographic and occupational variables. Prevalence of MSDs was determined as the proportion of respondents who reported pain in each anatomical region. Chi-square tests were used to measure associations between risk factors (i.e., OT hours, use of lead aprons, ergonomic practice) and MSD prevalence. Subgroup analyses evaluated differences across gender, experience level, and practice setting. A p < 0.05 was deemed to be statistically significant.
Results
Participant Characteristics
Out of 117 returned responses, 104 were complete and available for analysis (response rate: 88.9%). The group was male predominant (n=81, 78%), with 23 females (22%). Mean age was 36.4 ± 7.5 years (range: 26–59 years), and mean surgical experience was 8.2 ± 6.3 years. Volunteers were composed of 48 residents (46%), 39 consultants (38%), 10 academic surgeons (10%), and 7 private practitioners (7%). Most responses were from practitioners in urban facilities (78%), and spanned 14 states of India. Table 1 delineates the salient demographics of the group.
Table 1: Demographic and Occupational Characteristics of Participants
|
Characteristic |
Value |
|
Total Participants |
104 |
|
Male |
81 (78%) |
|
Female |
23 (22%) |
|
Mean Age (years) |
36.4 ± 7.5 |
|
Mean Surgical Experience (years) |
8.2 ± 6.3 |
|
Designation |
Residents: 48 (46%), Consultants: 39 (38%), Academic: 10 (10%), Private: 7 (7%) |
|
Practice Setting |
Urban: 78% |
Workload and environment
• OT Hours/Week: 25 (24%) had <10, 43 (41%) had 10–20, and 36 (35%) had >20 hours per week. Of the latter, 22 (21%) had >30 hours per week.
• Types of Procedures: Trauma surgery (68%), joint replacement (52%), and spine surgery (34%) were the most frequent, with 62% doing a combination of emergent and elective cases.
• Use of Lead Apron: 65 (62%) used lead aprons regularly (≥3 times/week), primarily in fluoroscopy-assisted trauma and spine procedures.
• Position of Surgery: 87 (84%) performed surgery standing, 13 (12%) used a mixed standing/sitting position, and 4 (4%) performed surgery sitting, primarily arthroscopic cases.
Ergonomic Tools and Practices
• Anti-Fatigue Mats: 19 (18%) reported having access to or using anti-fatigue mats in the OT.
• Height -adjustable equipment: 27 (26%) employed adjustable stools or chairs, and 77 (74%) employed height-adjustable OT tables.
• Intraoperative Breaks: 35 (34%) took breaks for posture adjustment during operations, with the majority of breaks being <5 minutes.
• Posture Awareness: 41 (39%) made a conscious effort to adjust posture during operations, but only 12 (12%) employed systematic techniques (e.g., micro-breaks, stretching).
Prevalence and Distribution of MSDs (Table 2)
85 (82%) of the respondents indicated musculoskeletal pain in one or more anatomical sites during the previous 12 months. Breakdown was:
•Lower Back: 60 (58%), of which 32 (31%) experienced moderate-to-severe pain.
•Neck: 49 (47%), of which 25 (24%) experienced pain that compromised surgical tasks.
•Shoulders: 41 (39%), typically bilateral (28, 27%).
•Wrists/Hands: 23 (22%).
• Upper Back: 18 (17%).
• Knees: 19 (18%).
• Ankles/Feet: 11 (11%).
• Hips/Thighs: 9 (9%).
• Elbows: 7 (7%), least affected.
23 (22%) consulted a medical specialist (e.g., orthopaedist, physiotherapist), 11 (11%) had workdays lost (mean: 4.2 days/year), and 9 (8.6%) considered reducing surgical work or changing to non-surgical roles.
Table 2: Prevalence of Musculoskeletal Disorders by Anatomical Region
|
Anatomical Region |
Prevalence (%) |
|
Lower Back |
58% |
|
Neck |
47% |
|
Shoulders |
39% |
|
Wrists/Hands |
22% |
|
Upper Back |
17% |
|
Knees |
18% |
|
Ankles/Feet |
11% |
|
Hips/Thighs |
9% |
|
Elbows |
7% |
Statistical Associations
• OT Hours: Surgeons with >30 OT hours/week also had significantly higher lower back pain (p = 0.02) and multi-site pain (≥3 areas, p = 0.03) (Fig 2).
• Lead Apron Use: Frequent users had more neck (p = 0.01) and shoulder pain (p = 0.01), with dose-response to frequency of use.
• Ergonomic Practices: No anti-fatigue mats or breaks was associated with greater pain in ≥3 anatomical locations (p < 0.05).
• Subgroup Results: Residents exhibited more wrist/hand pain (p = 0.04) from repetitive assisting activity, and consultants experienced more lower back pain (p = 0.03). Statistical gender differences were not significant (p > 0.05). Table 3 outlines the key associations identified.
Table 3: Association of Risk Factors with MSD Prevalence
|
Risk Factor |
Associated MSD Findings |
|
OT Hours > 30/week |
Higher lower back pain (p = 0.02), multi-site pain (p = 0.03) |
|
Frequent Lead Apron Use |
Increased neck and shoulder pain (p = 0.01) |
|
No Anti-Fatigue Mats or Breaks |
Greater pain in ≥3 sites (p < 0.05) |
|
Residents |
More wrist/hand pain (p = 0.04) |
|
Consultants |
More lower back pain (p = 0.03) |
Ergonomic Knowledge and Attitudes
- Knowledge: Fewer than 35 (34%) of them were familiar with ergonomic standards (e.g., AAOS or WHO guidelines).
- Training: 22 (21%) had actually undergone ergonomics training, primarily through international fellowships.
- Interest in Interventions: 74 (71%) were extremely interested in participating in ergonomic workshops with hands-on (48%) and online module (32%) choices.
Table 4 summarises the ergonomic practice prevalence and awareness among participants.
Table 4: Ergonomic Practices and Awareness
|
Practice/Awareness Aspect |
Value |
|
Use of Anti-Fatigue Mats |
18% |
|
Use of Height-Adjustable Equipment |
Stools: 26%, OT Tables: 74% |
|
Intraoperative Breaks |
34% |
|
Posture Awareness |
39% (Systematic techniques: 12%) |
|
Awareness of Ergonomic Standards |
34% |
|
Ergonomics Training |
21% |
|
Willingness for Workshops |
71% |
Discussion
Prevalence of MSDs
The research proves a high incidence of MSDs in Indian orthopaedic surgeons, with 82% experiencing pain in more than one anatomical area. Lower back (58%), neck (47%), and shoulders (39%) were common, consistent with international studies for 60–90% surgeon MSD prevalence. Still, the Indian setting has its own issues, such as longer OT working hours (30+ hours/week in 21% of respondents), limited access to ergonomic tools, and poor awareness of prevention measures (14–16). These conditions increase the risks of chronic pain and functional impairment, compromising surgeon well-being and efficiency of the healthcare system (10,17).
Risk Factors and Contextual Challenges
Protracted OT work hours (>30 hours/week) were highly associated with back pain, likely secondary to prolonged static standing and repetitive flexing. Use of lead aprons, required for radiation protection, was highly associated with neck and shoulder pain, as indicated by studies that found up to 20 kg additional weight stress on shoulders and neck during fluoroscopy (18,19). The unavailability of ergonomic equipment, for instance, anti-fatigue mats (utilized by only 18%) or OT stools with adjustable heights (26%), is an indication of systemic infrastructural inadequacies of Indian hospitals, especially in public and rural hospitals. Cultural beliefs such as reluctance to report pain or seek self-care might also be a source of underreporting and delayed intervention (20).
Figure 2 : Relationship between operation theatre (OT) hours per week and musculoskeletal disorder (MSD) pain severity scores. (The mean pain severity score increases progressively with higher OT hours, indicating a positive association between workload and MSD severity. Error bars represent standard deviations).
Global comparison
Park et al. in 2019 from the United States documented an incidence of 68% MSD in orthopaedic surgeons and a 30% symptom reduction by posture-correcting workshops (8). Epstein et al. in 2020 emphasized the effectiveness of organizational ergonomic guidelines, like compulsory breaks and adjustable equipment, in European hospitals (7). Indian surgeons, nevertheless, are at a resource disadvantage with only 26% of them utilizing adjustable stools and 34% of them enjoying breaks. East Asian countries (e.g., South Korea and Japan) report similar trends of MSD with more usage of robot-assisted surgeries, which minimize physical strain—a technology yet in the nascent stage in India (21–23) .
Practical Implications
The high prevalence of MSD in this study highlights the requirement of multi-level intervention. At the personal level, surgeons can practice micro-breaks, flexibility exercises, and posture awareness. At the hospital level, the hospitals need to spend on ergonomic gear, i.e., anti-fatigue mats, adjustable height furniture, and lighter lead aprons. At the policy level, ergonomics education as part of residency curricula and continuing medical education (CME) courses is essential. The 71% interest in workshops is a statement on the availability of a ready audience for the implementation of these programs.
Strengths and Limitations
Strengths: The research is one of the first to target MSDs in Indian orthopaedic surgeons, utilizing a validated instrument (NMQ) and high response rate (88.9%). The variety of sample, from residents to seniors and from urban to rural areas, increases generalizability in India.
Limitations: Recall bias or symptom magnification may be brought about by the self-reported survey method. Although the sample is representative, private or rural surgeons who are not part of many internet groups may be underrepresented since the study was conducted online. Objective clinical evaluation (e.g., imaging, physical examination) is missing and therefore limits grading of severity. Cross-sectional information prevents causality, and longitudinal follow-up studies would be required to track changes in MSDs. Psychological stressors (e.g., burnout) were not measured and can interact with MSDs.
Recommendations
1. Training: Integrate ergonomic training into orthopaedic residency programs with a focus on posture, breaks, and tool handling.
2. Facilities: Hospitals must perform ergonomic audits and purchase adjustable OT furniture and anti-fatigue mats.
3. Policy: National orthopaedic societies must develop guidelines for surgeon health that involve mandatory ergonomic evaluations.
4. Studies: Future research needs to include longitudinal designs, objective pain measurement, and assessment of the effectiveness of interventions (e.g., workshops, equipment modification).
Conclusion
Musculoskeletal disorders are a widely prevalent occupational risk among Indian orthopaedic surgeons, with 82% complaining of lower back, neck, and shoulder discomfort. Modifiable risk factors like extended OT work hours, utilization of lead aprons, and poor ergonomics fuel the epidemic. There is a poor level of awareness (34%) and training (21%), reflecting a noteworthy lacuna in education among surgeons. Systemic interventions such as ergonomic infrastructure, required training, and policy reform are critical to minimize MSDs, improve surgeon well-being, and ensure sustainable surgical practice. These findings should serve as a call to action for medical institutions, orthopaedic societies, and policy-makers to prioritize ergonomic safety and surgeon wellness
Conflict of Interest : None to declare
Ethical Considerations : The authors declare that all the participants have given informed digital consent for publication of their clinical data without any identifiers. Institutional Ethics Committee approval has been obtained prior to the survey.
References
1. Davis WT, Sathiyakumar V, Jahangir AA, Obremskey WT, Sethi MK. Occupational injury among orthopaedic surgeons. J Bone Joint Surg Am. 2013 Aug 7;95(15):e107.
2. Tan K, Kwek E. Musculoskeletal Occupational Injuries in Orthopaedic Surgeons and Residents. Malays Orthop J. 2020 Mar;14(1):24–7.
3. Livingstone RS, Varghese A, Keshava SN. A Study on the Use of Radiation-Protective Apron among Interventionists in Radiology. J Clin Imaging Sci [Internet]. 2018 Aug 24 [cited 2025 Jul 22];8. Available from: https://clinicalimagingscience.org/a-study-on-the-use-of-radiation-protective-apron-among-interventionists-in-radiology/
4. Baraskar SS, Borkar P. Epidemiology of musculoskeletal disorder among surgeons: a systematic review. International Journal of Research in Medical Sciences. 2022 Jun 28;10(7):1519–26.
5. AlQahtani SM, Alzahrani MM, Harvey EJ. Prevalence of musculoskeletal disorders among orthopedic trauma surgeons: an OTA survey. Can J Surg. 2016 Feb;59(1):42–7.
6. Stucky CCH, Cromwell KD, Voss RK, Chiang YJ, Woodman K, Lee JE, et al. Surgeon symptoms, strain, and selections: Systematic review and meta-analysis of surgical ergonomics. Annals of Medicine and Surgery. 2018 Mar;27:1–8.
7. Epstein S, Sparer EH, Tran BN, Ruan QZ, Dennerlein JT, Singhal D, et al. Prevalence of Work-Related Musculoskeletal Disorders Among Surgeons and Interventionalists: A Systematic Review and Meta-analysis. JAMA Surgery. 2018 Feb 21;153(2):e174947.
8. Park A, Lee G, Seagull JF, Meenaghan N, Dexter D. Patients Benefit While Surgeons Suffer: An Impending Epidemic. Journal of the American College of Surgeons. 2010 Mar;210(3):306.
9. Yasobant S, Rajkumar P. Work-related musculoskeletal disorders among health care professionals: A cross-sectional assessment of risk factors in a tertiary hospital, India. Indian J Occup Environ Med. 2014;18(2):75–81.
10. Catanzarite T, Tan-Kim J, Whitcomb EL, Menefee S. Ergonomics in Surgery: A Review. Female Pelvic Med Reconstr Surg. 2018;24(1):1–12.
11. Rosenblatt PL, McKinney J, Adams SR. Ergonomics in the operating room: protecting the surgeon. J Minim Invasive Gynecol. 2013;20(6):744.
12. Kuorinka I, Jonsson B, Kilbom A, Vinterberg H, Biering-Sørensen F, Andersson G, et al. Standardised Nordic questionnaires for the analysis of musculoskeletal symptoms. Appl Ergon. 1987 Sep;18(3):233–7.
13. Dickinson CE, Campion K, Foster AF, Newman SJ, O’Rourke AM, Thomas PG. Questionnaire development: an examination of the Nordic Musculoskeletal questionnaire. Appl Ergon. 1992 Jun;23(3):197–201.
14. Chahal K, Matwala K. A systematic review of the prevalence of burnout in orthopaedic surgeons. Ann R Coll Surg Engl. 2025 Jan;107(1):61–7.
15. Jain AK. Current state of orthopedic education in India. Indian J Orthop. 2016;50(4):341–4.
16. Shekhar S, Shetty V, Wagh Y. Challenges and Difficulties faced by Orthopedic Surgeons during the COVID-19 Pandemic: A Review of Modified Surgical Protocols.
17. Karam B, Soriano I. Ergonomics and body wellness during surgery: A review and practical guide. Seminars in Colon and Rectal Surgery. 2025 Mar 1;36(1):101085.
18. Pelz DM. Low Back Pain, Lead Aprons, and the Angiographer. AJNR Am J Neuroradiol. 2000 Aug;21(7):1364.
19. Rees CR, Duncan BWC. Get the Lead off Our Backs! Techniques in Vascular and Interventional Radiology. 2018 Mar 1;21(1):7–15.
20. Sau A, Phadikar S, Bhakta I, Chatterjee A. Global and Indian Scenarios of Fatal and Non-fatal Occupational Injuries: A Secondary Data Analysis. Indian Journal of Occupational and Environmental Medicine. 2024 Dec;28(4):282.
21. Wee IJY, Kuo LJ, Ngu JCY. A systematic review of the true benefit of robotic surgery: Ergonomics. Int J Med Robot. 2020 Aug;16(4):e2113.
22. Lee MR, Lee GI. Does a robotic surgery approach offer optimal ergonomics to gynecologic surgeons?: a comprehensive ergonomics survey study in gynecologic robotic surgery. Journal of Gynecologic Oncology. 2017 Mar 17;28(5):0.
23. Nishimura K. Current status of robotic surgery in Japan. Korean J Urol. 2015 Mar;56(3):170–8.
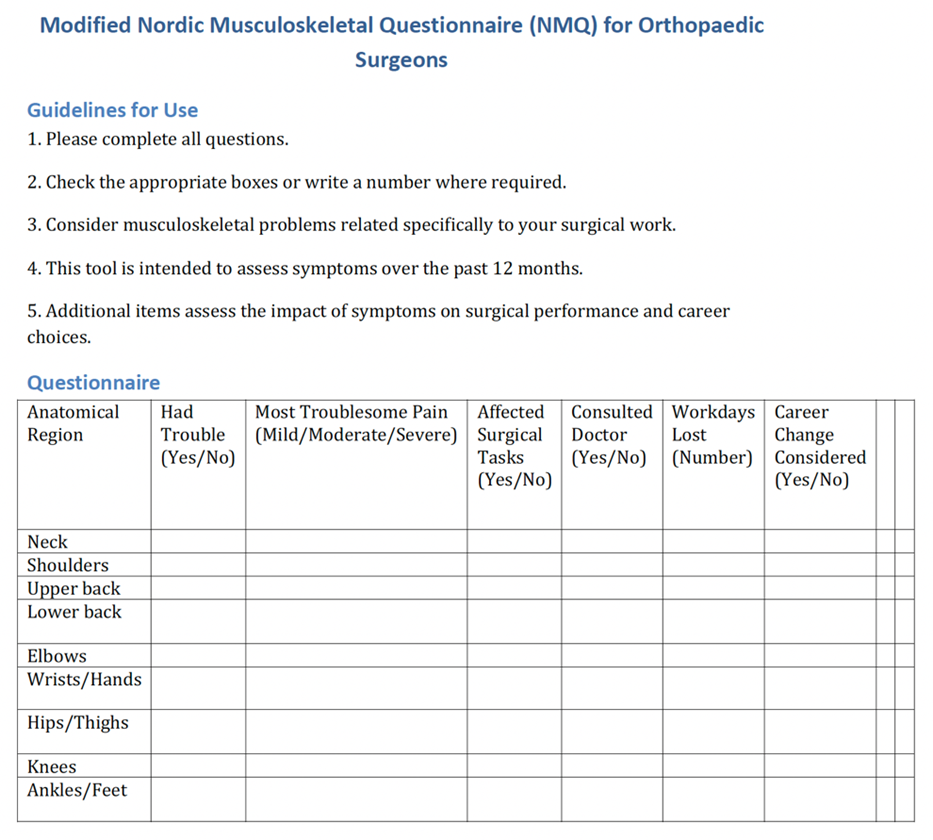
Figure 1
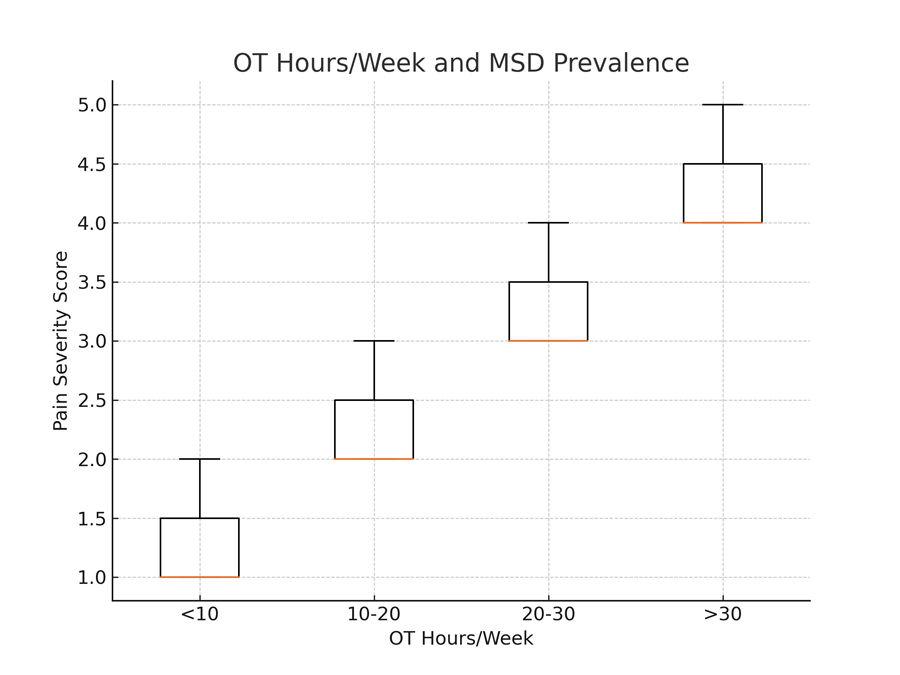
Figure 2