A Rare Case of Poorly Differentiated Thyroid Carcinoma Arising in Lingual Thyroid and Presenting as a Huge Neck Mass
A Rare Case of Poorly Differentiated Thyroid Carcinoma Arising in Lingual Thyroid and Presenting as a Huge Neck Mass
Dr. Janemary Jeesemon *1, Dr.Jyothi Karikkanthra2, Dr. Ferdinant Jabamalai3, Dr. Ramzi Shamsuddeen4, Dr Arya P M5
1. Dr. Janemary Jeesemon, Department of Pathology, Apollo Adlux Hospital.
2. Dr. Jyothi Karikkanthra, Department of Pathology, Apollo Adlux Hospital.
3. Dr. Ferdinant Jabamalai, Department of Endocrine Surgery, Apollo Adlux Hospital.
4. Dr. Ramzi Shamsuddeen, Department of Radiology, Apollo Adlux Hospital.
5. Dr. Arya P M, Department of Pathology, Apollo Adlux Hospital.
*Correspondence to: Dr. Janemary Jeesemon, Department of Pathology, Apollo Adlux Hospital, Kerala, India.
Copyright
© 2025 Dr. Janemary Jeesemon. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 02 Aug 2025
Published: 18 Aug 2025
Abstract
Lingual thyroid refers to ectopic thyroid tissue located at the base of the tongue. It results from an abnormal descent of the thyroid gland during embryological development. Ectopic thyroid is usually asymptomatic. Here we report a rare case of poorly differentiated thyroid carcinoma arising in lingual thyroid of a 64 years female presenting as a long standing left side neck mass.
Key words: Lingual thyroid, neck mass, Poorly differentiated carcinoma.
A Rare Case of Poorly Differentiated Thyroid Carcinoma Arising in Lingual Thyroid and Presenting as a Huge Neck Mass
Introduction
Ectopic thyroid tissue is usually asymptomatic. We report a case of lingual thyroid presenting as a large neck mass, with histopathological evaluation revealing a poorly differentiated thyroid carcinoma. Carcinoma in lingual thyroid is extremely rare and even more rare is a poorly differentiated thyroid carcinoma in lingual thyroid.
Case History
A 64 years old lady presented to the OPD with complaints of a large neck mass in the sub-mandibular region of 20 years duration with a recent rapid increase in size (Figure 1A). Per oral examination showed lingual thyroid enlargement.
Figure 1
MRI revealed a large mixed-intensity lesion (Figure 1B) involving the base of the tongue and floor of the mouth, measuring approximately 9.2 cm anteroposteriorly (AP) × 10.7 cm transversely (TR) × 11.1 cm craniocaudally (CC).The lesion is seen extending exophytically into the neck region with a predilection towards left side. Visualised lung fields show multiple T2 hyperintense nodules on both sides likely metastasis. Thyroid is not visualized in the thyroid fossa-likely absent.
Fine-needle aspiration cytology (FNAC) revealed papillaroid clusters with nuclear features such as crowding, overlapping, nuclear grooves, and intranuclear inclusions (Figure 2A). Based on these findings, the FNAC was reported as thyroid carcinoma with papillary-like nuclear features.
The patient underwent surgical exploration, during which a large mass arising from the base of the tongue and attached to the hyoid bone was identified and successfully dissected out.
Figure 2
Cut section of lesion is fairly circumscribed variegated lesion with grey, white and yellow areas (Figure 2B). Lesion is predominantly solid with small cystic areas. No infiltration into attached skin grossly.
Histopathological examination revealed thyroid tissue with a neoplasm arranged in sheets and an insular pattern (Figure 3A). The tumor cells exhibited convoluted nuclear membranes and areas of necrosis. Additionally, focal areas showed a follicular arrangement with papillary-like nuclear features (Figure 3B). Based on these findings, a diagnosis of poorly differentiated thyroid carcinoma was made. Neoplastic cells are immunoreactive for Thyroglobulin(Figure 3C) and TTF1(Figure 3D) . Thyroglobulin expression is reduced in poorly differentiated areas.
Figure 3
Postoperatively patient had difficulty in swallowing and speech. Hence she was started on Ryles tube feeding.Currently Ryles tube withdrawn and patient is on swallow and speech therapy. Further plan is to withhold Thyroxine for six weeks and to start Radioactive Iodine ablation.
Discussion
Occurrence of ectopic thyroid tissue is rare and it is due to the failure of its embryological descent from floor of the primitive foregut to the pretracheal position.[1] The cause for the condition is still not known completely.[2] The most common site of ectopic thyroid is at the base of the tongue.[2] Most cases of ectopic thyroid including Lingual thyroid is asymptomatic. Symptoms if present depend on the size and location.[3]
In majority of patients with lingual thyroid, it is the only thyroid tissue present and hence the only source of thyroid hormone production. Hypothyroidism and very rarely hyperthyroidism is reported in patients with lingual thyroid.[4]
Malignancy in lingual thyroid is extremely rare. Approximately 1% of patients with lingual thyroid develop carcinoma. The female to male ratio of carcinoma in lingual thyroid is approximately 3:1and the prevalence is more in the third decade of life.[5,6,7]
The first case of carcinoma in lingual thyroid was described by Hickman W. in 1869.[8]
The predominant carcinoma arising in lingual thyroid as per latest literature is papillary carcinoma. However earlier studies reported a higher incidence of follicular carcinoma over papillary. The possible explanation for this is a histological misclassification in the early reports due to the lack of standardization in the classification of differentiated Thyroid carcinoma.[9]Only reported is a single case of medullary thyroid carcinoma[10]and no case of anaplastic thyroid carcinoma.
The natural history of the disease is not completely known due to the extreme low prevalence of lingual thyroid carcinoma. Out of the reported cases, predominant cases are confined to the tongue. Cases with loco-regional metastasis account for 20% cases and distant metastasis account for 14% of the total cases.[5]In our case, the patient had bilateral lung metastasis.
Conclusion
Carcinoma in a lingual thyroid is extremely rare and to the best of our knowledge there has been no case report of a poorly differentiated thyroid carcinoma in lingual thyroid.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient has given her consent for her images and other clinical information to be reported in the journal. The patient understand that their name and initial will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship Nil.
Conflicts of interest: There are no conflicts of interest
References
1.Noussios G, Anagnostis P, Goulis DG, Lappas D, Natsis K. Ectopic thyroid tissue: anatomical, clinical, and surgical implications of a rare entity. Eur J Endocrinol. 2011;165:375–382.
2.Guerra G, Cinelli M, Mesolella M, Tafuri D, Rocca A, Amato B, et al. Morphological, diagnostic and surgical features of ectopic thyroid gland: a review of literature. Int J Surg. 2014;12:S3–S11. doi:10.1016/j.ijsu.2014.05.076.
3.Ibrahim NA, Fadeyibi IO. Ectopic thyroid: etiology, pathology and management. Hormones (Athens). 2011;10:261–269. doi:10.14310/horm.2002.1317.
4.Y 4. J.S. Yoon, K.C. Won, I.H. Cho, J.T. Lee, H.W. Lee, Clinical characteristics of ectopic thyroid in Korea, Thyroid 17 (2007) 1117e1121.
5.Klubo-Gwiezdzinska J, Manes RP, Chia SH, Burman KD, Stathatos NA, Deeb ZE, et al. Clinical review: Ectopic cervical thyroid carcinoma--review of the literature with illustrative case series. J Clin Endocrinol Metab. 2011;96:2684–2691. doi:10.1210/jc.2011-0611.
6.Kennedy TL, Whitaker M, Wadih G. Thyroglossal duct carcinoma: a rational approach to management. Laryngoscope. 1998;108:1154–1158. doi:10.1097/00005537-199808000-00010.
7.Massine RE, Durning SJ, Koroscil TM. Lingual thyroid carcinoma: a case report and review of the literature. Thyroid. 2001;11:1191–1196. doi:10.1089/10507250152741055.
8.Hari CK, Kumar M, Abo-Khatwa MM, Adams-Williams J, Zeitoun H. Follicular variant of papillary carcinoma arising from lingual thyroid. Ear Nose Throat J. 2009;88:E7. PMID: 19517394.
9.Sturniolo G, Violi MA, Galletti B, Baldari S, Campennì A, Vermiglio F, Moleti M. Differentiated thyroid carcinoma in lingual thyroid. Endocrine. 2016;51:189–198. doi:10.1007/s12020-015-0593-y.
10.Mazzaferri EL, Kloos RT. Clinical review 128: Current approaches to primary therapy for papillary and follicular thyroid cancer. J Clin Endocrinol Metab. 2001;86:1447–1463. doi:10.1210/jcem.86.4.7407.

Figure 1
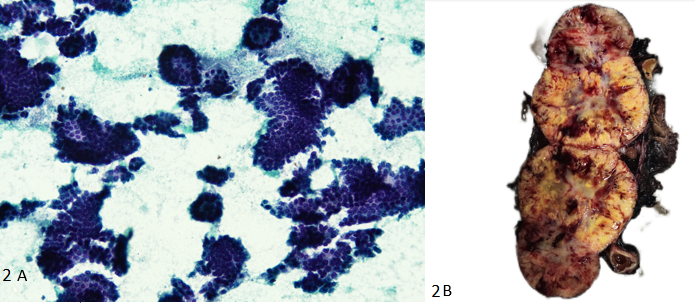
Figure 2
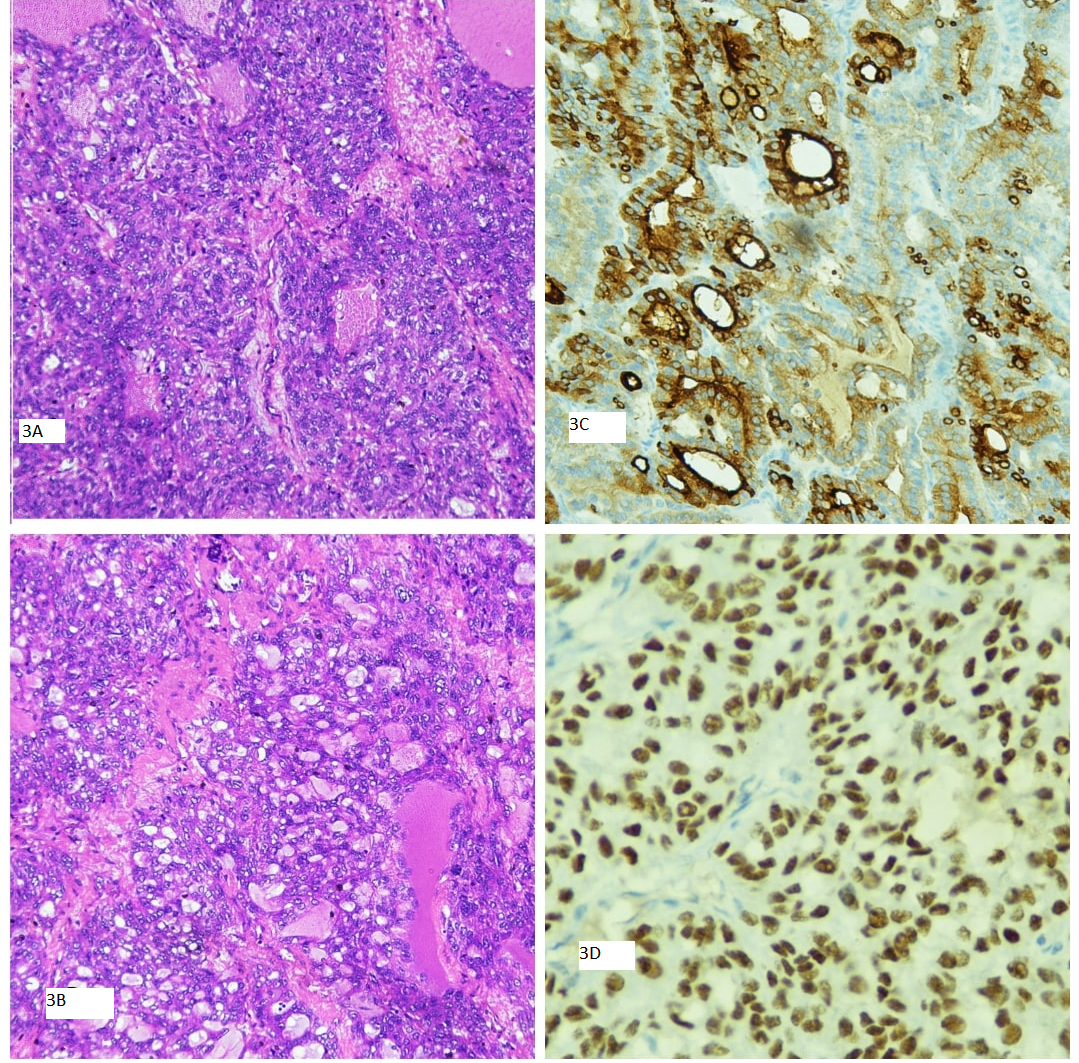
Figure 3