Evaluating Functional Outcomes of ACL Reconstruction using Hamstring Grafts: A Saudi Arabian Perspective
Evaluating Functional Outcomes of ACL Reconstruction using Hamstring Grafts: A Saudi Arabian Perspective
Muhammad Azfar Khanzada, MBBS, FCPS, MRCS (Glasgow)1*, Omer Adil Fathelrahm Awadelkarim, MBBS2, Mohamed Sied Ali Mahgoub Elnor, MBBS, MRCS3, Tariq Yahia Sidahmed Alatta, MBBS4, Qamar Jaleel Akhtar, MBBS, FRCS, FRCSPG5
1. Specialist Orthopedic, Dr. Sulaiman Alhabib Hospital, Riyadh, KSA.
2, 3, 4. Resident Orthopedic, Dr. Sulaiman Alhabib Hospital, Riyadh, KSA.
5. Consultant Orthopedic Surgeon, Dr. Sulaiman Alhabib Hospital, Riyadh, KSA.
*Correspondence to: Muhammad Azfar Khanzada, Specialist Orthopedic, Dr. Sulaiman Alhabib Hospital, Riyadh, KSA.
Copyright
© 2025 Muhammad Azfar Khanzada is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 06 Aug 2025
Published: 19 Aug 2025
DOI: https://doi.org/10.5281/zenodo.16899738
Abstract
Hamstring auto grafts have become widely accepted as a biomechanically superior option for anterior cruciate ligament (ACL) reconstruction, especially among Saudi Arabia’s physically active population. This retrospective study analyzes 178 patients who underwent hamstring graft ACL reconstruction, evaluating functional recovery and the impact of structured rehabilitation protocols. Within six months, 88% showed marked improvement in knee function. The mean Lysholm score improved from 50 preoperatively to 86 at 12 months. Additionally, 92% of patients reported satisfaction, which was closely associated with compliance to rehabilitation programs.
Key words: ACL reconstruction, hamstring graft, knee function, rehabilitation.
Evaluating Functional Outcomes of ACL Reconstruction using Hamstring Grafts: A Saudi Arabian Perspective
Introduction
Anterior cruciate ligament (ACL) injuries are increasingly prevalent in Saudi Arabia, particularly among athletes engaged in sports requiring rapid pivoting and acceleration. Hamstring autografts, typically harvested from the semitendinosus and gracilis tendons, are widely favored for ACL reconstruction due to their biomechanical strength, elasticity, and low donor site morbidity [1,2].
This study aims to evaluate the functional outcomes of ACL reconstruction using hamstring autografts and to analyze the impact of structured rehabilitation protocols. We present a retrospective analysis of 178 patients treated at a tertiary care hospital in Riyadh, Saudi Arabia.
Materials and Methods
Patient Selection
A total of 178 patients who underwent anterior cruciate ligament (ACL) reconstruction at Dr. Sulaiman Al Habib Suwaidi Hospital between 2017 and 2024 were included in this retrospective analysis. The cohort comprised 176 male and 2 female patients, with ages ranging from 17 to 52 years. Of the total cases, 76 involved the left knee, while 102 involved the right knee.
Surgical Technique
All procedures employed arthroscopic techniques using hamstring autografts. Graft harvesting utilized semitendinosus and gracilis tendons, followed by rigid femoral and tibial fixation. Tunnel placement was confirmed using anatomical landmarks under arthroscopic visualization [5–8].
Rehabilitation Protocol
Patients followed a four-phase rehabilitation program:
- Weeks 0–4: Edema control, protection of graft, early range of motion
- Weeks 4–8: Strength training, progressive weight-bearing
- Weeks 8–12: Proprioceptive exercises, balance training
- Weeks 12+: Sport-specific drills, return to functional activity [17,18]
Fig 1: Recovery Roadmap: From Swelling to Strength
Outcome Assessment
Postoperative evaluations were conducted at 3, 6, and 12 months using:
- Lysholm Knee Scoring Scale [17]
- International Knee Documentation Committee (IKDC) Questionnaire [18]
Results
In analyzing the patients, a notable 88% demonstrated significant improvements in knee function within six months following surgery. The average Lysholm Knee Score surged from 50 preoperatively to an impressive 86 by twelve months. Functional recovery showed substantial enhancement in patients who followed structured rehabilitation programs, effectively minimizing complications such as stiffness and instability. Furthermore, a resounding 92% of patients reported satisfaction with their surgical outcomes, underscoring the proven effectiveness of hamstring graft techniques in ACL reconstruction.
Fig 2: Post-operative progress
Discussion
Our findings align with existing literature, confirming that hamstring auto grafts offer excellent biomechanical properties and contribute to stable long-term outcomes [1–4]. Anatomical tunnel placement significantly influences graft performance, minimizing laxity and failure rates [9–13].
Structured rehabilitation was pivotal to recovery. Patients adhering to therapy protocols exhibited:
- Lower rates of stiffness, instability, and pain
- Higher Lysholm scores and subjective satisfaction
Similar global studies have echoed these outcomes, emphasizing that postoperative physiotherapy, particularly neuromuscular training and proprioceptive reinforcement, enhances recovery and athletic reintegration [3–5,17].
Conclusions
ACL reconstruction using hamstring autografts in Saudi Arabia yields favorable functional outcomes. Structured rehabilitation plays a critical role in minimizing complications and enhancing patient satisfaction. These findings support the widespread use of hamstring graft techniques in ACL surgery and highlight the importance of post-surgical protocol adherence.
References
1. Cirstoiu C, Circota G, Panaitescu C, Niculaita R. Mædica. 2011;6(2):109.
2. Fu FH, Bennett CH, Latterman C, Ma CB. Am J Sports Med. 1999;27(6):821–30.
3. Lyman S, et al. J Bone Joint Surg Am. 2009;91(10):2321–8.
4. Frank CB, Jackson DW. J Bone Joint Surg Am. 1997;79(10):1556–76.
5. Shervegar S, et al. Arch Bone Jt Surg. 2015;3(4):264–8.
6. Moore KL. Clinically Oriented Anatomy. 2nd ed. 1985.
7. Colombet P, et al. Arthroscopy. 2006;22:984–92.
8. Ferretti M, et al. Arthroscopy. 2007;11:1218–25.
9. Purnell ML, et al. Am J Sports Med. 2008;36:2083–90.
10. Siebold R, et al. Arthroscopy. 2008;24:154–61.
11. Siebold R, et al. Arthroscopy. 2008;24:585–92.
12. Takahashi M, et al. Am J Sports Med. 2006;34:787–92.
13. Tantuway V, et al. Int J Res Orthop. 2017;3:43–9.
14. Prins M. Aust J Physiother. 2006;52(1):66.
15. Hing W, et al. J Man Manip Ther. 2009;17(1):22–35.
16. Miller RH III, Azar FM. Campbell's Operative Orthopaedics. 11th ed. 2008.
17. Tegner Y, Lysholm J. Clin Orthop Relat Res. 1985;198:43–9.
18. Collins NJ, et al. Arthritis Care Res. 2011;63(11):208–28.
19. Gurtler RA, et al. Contemp Orthop. 1990;20(2):145–54.
20. Frank CB, Jackson DW. J Bone Joint Surg Am. 1997;79:1556–76..
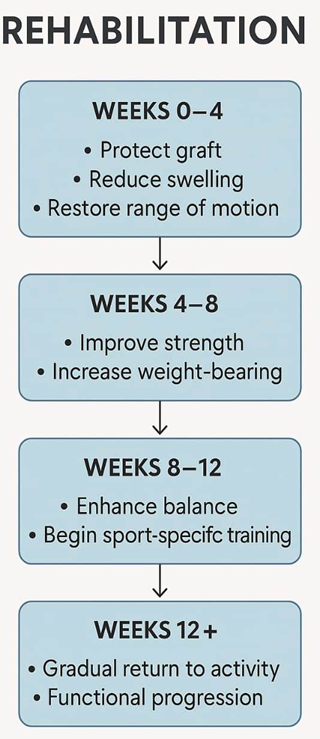
Figure 1
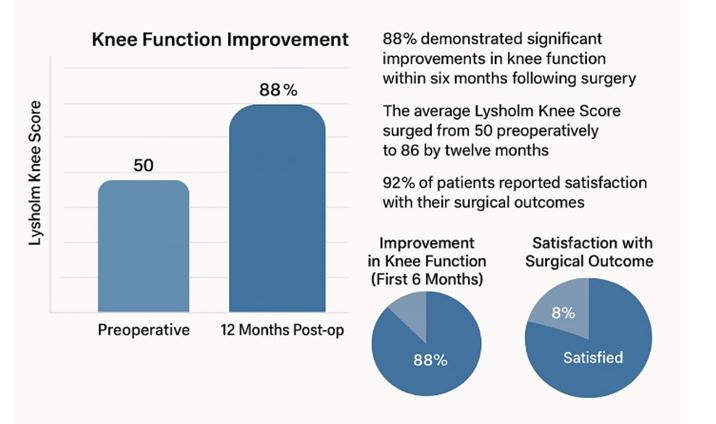
Figure 2