Gastrointestinal Mucormycosis - A Report of Two Cases.
Gastrointestinal Mucormycosis - A Report of Two Cases.
Indu Manicketh1*, Victoria Liza N2, Praveen Kumar C3
*Correspondence to: Dr. Indu Manicketh, Apollo Speciality Hospital, Lakeview Road, KK Nagar
Madurai-625020, Tamil Nadu, India. ORCID ID :0009-0008-3922-7962.
Copyright
© 2025 Dr. Indu Manicketh. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 07 Aug 2025
Published: 01 Sep 2025
Abstract
Abstract: Fungal infection of the gastrointestinal tract, particularly Mucormycosis is a rare entity. We report two cases of Mucormycosis of the stomach and sigmoid colon. Due to the rarity of this entity, the disease may be difficult to diagnose clinically. The disease may masquerade as malignancy clinically. Histopathological examination combined with microbiological studies play a key role in clinching the diagnosis and starting appropriate treatment.
Key words: Mucormycosis, Gastrointestinal, Immunocompromised.
Gastrointestinal Mucormycosis - A Report of Two Cases.
Introduction
Gastrointestinal Mucormycosis is a fungal infection caused by fungi of the subphylum Mucoromycotina, order Mucorales.1. It commonly affects the sino nasal cavity, orbit and brain.1 Cases involving the gastrointestinal tract are rare. Over the past two decades there has been an increase in the number of cases of gastrointestinal Mucormycosis. Stomach is the commonest site of infection followed by the colon and ileum. The disease is more common in immunocompromised population.2,6 We report two cases of gastrointestinal Mucormycosis in a tertiarty care hospital in India.
Case 1: A 76 year old female was admitted to the emergency with the complaints of malena and severe abdominal pain. Patient was a known diabetic on insulin. Investigations revealed the following. Hemoglobin- 8.2 g% Total WBC count -3100/mm3. Platelet count -1.5 lakhs/mm3. The peripheral smear revealed normocytic normochromic anemia with neutrophilia. The biochemical investigations revealed random blood glucose of 155 mg/dL.Serum urea was elevated- 110mg/dL. Serum creatinine was elevated-1.4 mg/dL.
The Computed Tomography (CT) scan of abdomen revealed a polypoid growth in the sigmoid colon with areas of necrosis[K1] . A provisional clinical diagnosis of malignancy of sigmoid colon was made and the patient was posted for a colonoscopy and biopsy.
Colonoscopy revealed a polypoid growth in the splenic flexure of colon with ulceration which was suspicious for malignancy. A biopsy was performed. The clinical condition of the patient deteriorated post procedure and the patient was intubated.
Biopsy revealed friable colonic mucosa with dense ulceration. Many aseptate broad hyphae were seen with right angled branching. There was no evidence of tissue invasion and angioinvasion in the sections examined. The Periodic Acid Stain (PAS) highlighted the fungal hyphae. (Figure 1A and 1B).There was no dysplasia or malignancy in the biopsy specimen submitted. Hence a diagnosis of Mucormycosis of the sigmoid colon was made. The diagnosis was conveyed to the treating physician .The patient was started on liposomal Amphotericin B. A repeat procedure was planned to procure material for microbiological confirmation . The second procedure resulted in a perforation,the clinical condition of the patient rapidly deteriorated and the patient went against medical advice. The KOH (Potassium Hydroxide) mount and subsequent fungal culture confirmed the diagnosis of Mucormycosis.
Case 2 – A 58 year old male patient was admitted to the emergency with history of seizure followed by unconsciousness. The patient was a known case of type 2 Diabetes which was uncontrolled and he presented with diabetic ketoacidosis. The patient also had past history of stroke and pyeolnephritis. Following admission,the patient had one episode of malena. Investigations revealed the following- Hemoglobin- 9.9 g% Total WBC count -16000/mm3. Platelet count -1.2 lakhs/mm3. The peripheral smear revealed normocytic hypochromic anemia with neutrophilic leucocytosis. The biochemical investigations revealed random blood glucose of 375 mg/dL. Glycosyalated Hemoglobin (HbA1C)-19.4 g% Serum urea was elevated- 161mg/dL. Serum creatinine was elevated-4.4 mg/dL. Blood Ketone was elevated 6. Liver enzymes were elevated- SGOT 212U/L, SGPT 82 U/L, Alkaline Phospatase- 130 U/L
The patient was in sepsis with a C Reactive Protein (CRP) of 100mg/L and multiple organ dysfunction. The patient was shifted to the intensive care unit.
CT scan of the abdomen revealed an ulcer along the lower curvature measuring approximately 3 X 2 cm. Hence a provisional clinical diagnosis of malignancy of the stomach was made and the patient was posted for an upper GI endoscopy.Endoscopy revealed an ulcer in the incisura of stomach along the lower curvature of stomach.(Figure 2B) Biopsy was performed.
Histopathological examination showed dense ulceration. Many broad , aseptate hyphae were seen with right angled branching. (Figure 2A) Tissue invasion and angioinvasion was present in the biopsy. Also budding spores of Candidal species was seen. The PAS stain highlighted the fungal hyphae and Candidal spores. Hence a diagnosis of polyfungal infection- Invasive Mucormycosis and candidiasis of stomach was made. Microbiological confirmation was advised. The KOH mount showed fungal hyphae morphologically consistent with Mucormycosis and fungal spores of Candidal species. The fungal cultures ascertained the same. Since invasive fungal infection is a critical alert, the diagnosis was immediately conveyed to the clinician. The patient was started on liposomal Amphotericin B and oral Fluconazole. Dose titration was difficult due to the deranged renal parameters of the patient. The clinical condition of the patient marginally improved after starting the antifungal medication, but he succumbed to the disease due to multiorgan dusfunction and sepsis.
Figure 2A Colonic biopsy showing hyphae of Mucormycosis and spores of Candida
Figure 2B Endoscopic appearance of ulcer in Case 2
Discussion
Mucormycosis, previously known as Zygomycosis is a life-threatening fungal infection. Risk factors for the development of invasive mucormycosis include diabetes, immunocompromised states, corticosteroid use, organ or stem cell transplantation1.The commonest site of infection by Mucormycosis is the sino nasal cavity. Gastrointestinal fungal infection is a rare clinical entity which is commonly seen in Diabetic and immunocompromised patients who are critically ill. Both of our patients were critically ill and had deranged renal parameters. The disease is common in premature neonates and association with necrotizing enterocolitis has been reported 2. In our report, both patients were over the age of 60 years and had Diabetes mellitus. There is an increase in the number of cases of gastrointestinal mucormycosis over the past decade as reported in the review by Spellberg1 . There is also an increase in nosocomial gastrointestinal Mucor mycosis over the past decade. An interesting case report describes a nosocomial outbreak of Mucormycosis due to a contaminated wooden tongue depressor which was used for mixing drugs for enteric feeding3. Stomach has been reported as the commonest site of gastrointestinal Mucormycosis followed by colon and ileum 1,4. In our report the sites of infection were stomach and colon. The diagnosis is often not suspected clinically because of the rarity of this entity. The clinical presentation is varied and gastrointestinal bleed is a common symptom. Both our cases presented with malena. The clinical presentation and the necrotic and ulcerated endoscopic appearance often mimics a malignancy as was seen in both of our cases.
Microbiological fungal culture can take up to about 15 days for results . Since Mucormycosis is a critical disease entity which is often fatal if untreated, prompt diagnosis is a must. This underlines the importance of an accurate histopatholgical diagnosis to initiate appropriate patient management. A thorough and meticulous search for fungal organisms combined with special stains like Periodic Acid Schiff (PAS) and Gomori Methenamine Silver (GMS) should be done in all gastrointestinal biopsies exhibiting necrosis to ensure that the diagnosis is not missed. A good clinical practice could be to preserve a few tissue bits in saline for fungal studies in cases where there is extensive necrosis. This could eliminate the need for a repeat biopsy which might cause complications such as perforation,as was seen in our first case. Mucormycosis can cause extensive necrosis and thinning of the intestinal wall. Hence perforation is a common finding in gastrointestinal Mucormycosis.4
Management of Zygomycosis in patients with multi organ dysfunction is a challenge.Succesful treatment includes surgical debridement and antifungal therapy. 5 In our report, both patients had deranged renal parameters which made treatment with antifungals very challenging. A sleeve gastrectomy was planned in the first case for surgical debridement. But it could not be carried out due to the clinical condition of the patient. This highlights the importance of an early and accurate diagnosis to prevent mortality.
Conclusion
Gastrointestinal Mucormycosis, a rare entity is a leading cause of morbidity and mortality in critically ill and immunocompromised patients. Histopathology is one of the main modalities for ascertaining a quick diagnosis which can be followed up by microbiological confirmatory studies. Early diagnosis and treatment can reduce the risk of mortality.
References
1 Spellberg B. Gastrointestinal mucormycosis: an evolving disease. Gastroenterol Hepatol (N Y). 2012 Feb;8(2):140-2.
2 Kecskes S, Reynolds G, Bennett G. Survival after gastrointestinal mucormycosis in a neonate. J Paediatr Child Health. 1997;33:356–359.
3 Maravi-Poma E, Rodriguez-Tudela JL, de Jalon JG, et al. Outbreak of gastric mucormycosis associated with the use of wooden tongue depressors in critically ill patients. Intensive Care Med. 2004;30:724–728.
4 Sharma MC, Gill SS, Kashyap S, Kataria R, Gupta DK, Sahni P, Acharya SK. Gastrointestinal mucormycosis--an uncommon isolated mucormycosis. Indian J Gastroenterol. 1998 Oct-Dec;17(4):131-3.
5 Alghamdi A, Lutynski A, Minden M, Rotstein C. Successful treatment of gastrointestinal mucormycosis in an adult with acute leukemia: case report and literature review. Curr Oncol. 2017 Feb;24(1):e61-e64.
6 Addasi Y, Nguyen AH, Sabri A, Ahmad F, Rangray R, Velagapudi M. Gastrointestinal Mucormycosis: A Clinical Review. Gastroenterology Res. 2023 Oct;16(5):249-253.
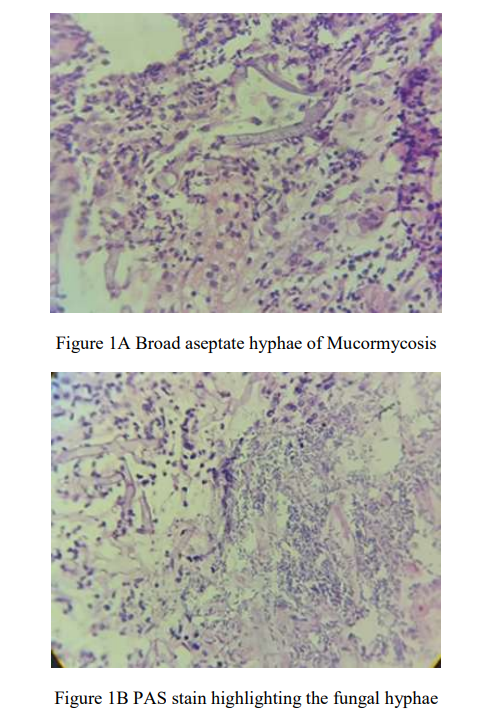
Figure 1
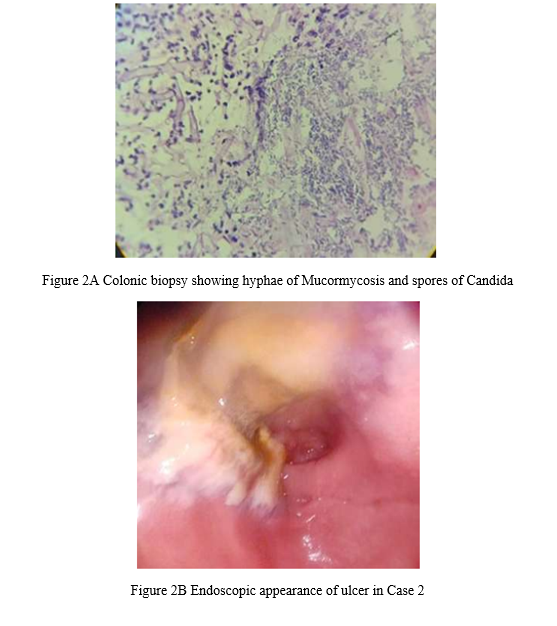
Figure 2