Placenta Previa Major with Suspected Placenta Accreta/Percreta Managed with Caesarean Hysterectomy
Placenta Previa Major with Suspected Placenta Accreta/Percreta Managed with Caesarean Hysterectomy
Ahmed Abdelsalm.1*, Ibrahim Talat Kasar MCH, MOH2, Aisha Babikir Taha, MBBS, MD, MRCOG.3
2. Obstetrics and Gynaecology Consultant, Bisha Maternity Hospital, KSA.
3. Obstetrics and Gynaecology Registrar, Princess Royal Maternity Hospital, Glasgow, Scotland, UK.
*Correspondence to: Ahmed Abdelsalm, Obstetrics and Gynaecology Registrar, Cavan general hospital, Republic of Ireland.
Copyright
© 2025 Ahmed Abdelsalm. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 20 Aug 2025
Published: 03 Sep 2025
Abstract
Placenta accreta spectrum (PAS) disorders, including placenta percreta, pose significant maternal and foetal risks, particularly in women with prior caesarean deliveries.
This case report describes a 36-year-old female, gravida 6, para 4+1, with a history of three caesarean sections, presenting at 34 weeks and 2 days gestation with minimal vaginal bleeding. Bedside ultrasound confirmed placenta previa major, with suspected placenta accreta/percreta.
She was admitted to the hospital with plan of optimizing and preparation for delivery by caesarean birth. Imagine and bloods were requested. The gestational age was of reasonable maturity thus delivery was recommended specially that she presented with bleeding.
Multidisciplinary team, including obstetrics, anaesthetist, urologist, vascular surgeon, and neonatologist made, she was delivered via emergency caesarean performed to mitigate risks of massive haemorrhage, DIC, organ damage and maternal death.
The procedure, performed under general anaesthesia, with intraoperative findings of placental invasion into the bladder. It resulted in the delivery of a viable foetus and successful hysterectomy, with no significant postoperative complications. Blood transfusions (packed red blood cells, fresh frozen plasma, platelets) were administered intra- and postoperatively.
The patient remained stable in the maternal ICU, with normal lochia and normal vital signs. This case revealed the importance of early diagnosis, multidisciplinary coordination, and timely surgical intervention in managing placenta percreta, particularly in high-risk patients with prior caesareans.
Placenta Previa Major with Suspected Placenta Accreta/Percreta Managed with Caesarean Hysterectomy
Introduction
Placenta praevia complicated by placenta accreta spectrum (PAS) represents a significant obstetric challenge associated with high maternal morbidity and mortality. Placenta praevia occurs when the placenta implants in the lower uterine segment, covering part or all of the cervix, increasing the risk of antepartum bleeding and preterm birth. When combined with placenta accreta, the placental villi abnormally invade the myometrium, failing to separate spontaneously after delivery. This abnormal adherence can extend from accreta (superficial invasion) to increta (deep myometrial invasion) and percreta (penetration beyond the uterine serosa), often resulting in massive postpartum hemorrhage.
The incidence of placenta accreta spectrum has risen in parallel with increasing cesarean delivery rates, as prior uterine surgery is a key risk factor. Accurate antenatal diagnosis through ultrasound and magnetic resonance imaging (MRI) is critical for optimal management. Early identification allows for multidisciplinary planning involving obstetrics, anaesthesia, neonatology, and sometimes interventional radiology, with delivery typically scheduled by cesarean hysterectomy in a controlled setting. Management strategies focus on minimizing hemorrhagic complications and ensuring maternal safety. Despite advances in prenatal diagnosis and surgical techniques, placenta praevia with accreta remains a leading cause of severe obstetric hemorrhage and peripartum hysterectomy. Continued research and standardized clinical protocols are essential to improve outcomes for affected women. [1,2,3]
Case Presentation
A 36-year-old. G6P4+1, presented to the emergency department, at 34 weeks and 2 days gestation with vaginal spotting. She had a history of three prior caesarean sections and an ovariancystectomy. She was vitally stable. Physical exam revealed a soft, non-tender abdomen, closed cervix, and minimal vaginal bleeding with small dark clots. Cardiotocography was reactive with no contractions, confirming fetal well-being.
Bedside ultrasound confirmed a single viable fetus in cephalic presentation with placenta previa major. MRI was requested to assess for placenta accreta, but the report was pending at the time of intervention. Full blood count, liver/ renal profile and coagulation profile were normal. Group and save as well as cross-matching for four units was requested.
Initial management included observation, nill per oral, and enoxaparin held. A multidisciplinary team consisting of senior doctor from OB/GYN, anesthesia, ICU, general surgery, urology, vascular surgery, and NICU was coordinated. 4 days after admission, elective caesarean section with caesarean hysterectomy was performed under general anaesthesia. The procedure involved a midline incision, delivery of a viable fetus via breech extraction, and hysterectomy due to a morbidly adherent placenta invading the uterine wall and bladder.
Blood products (10 units PRBCs, 10 units FFP, cryoprecipitate, and platelets) were prepared, with transfusions administered intra- and postoperatively (e.g., 2 units FFP, 2 units platelets, 2 units PRBCs).The fetus was delivered in good condition, cried immediately and received by the NICU team. Postoperatively, the patient was stable in the ICU, normal lochia, stable observations and good urine output.
Figure 1
Discussion
Placenta praevia complicated by placenta accreta spectrum (PAS) represents a significant obstetric challenge associated with high maternal morbidity and mortality. Placenta praevia occurs when the placenta implants in the lower uterine segment, covering part or all of the cervix, increasing the risk of antepartum bleeding and preterm birth. When combined with placenta accreta, the placental villi abnormally invade the myometrium, failing to separate spontaneously after delivery. This abnormal adherence can extend from accreta (superficial invasion) to increta (deep myometrial invasion) and percreta (penetration beyond the uterine serosa), often resulting in massive postpartum haemorrhage.
The incidence of placenta accreta spectrum has risen in parallel with increasing caesarean delivery rates, as prior uterine surgery is a key risk factor. Accurate antenatal diagnosis through ultrasound and magnetic resonance imaging (MRI) is critical for optimal management. Early identification allows for multidisciplinary planning involving obstetrics, anaesthesia, neonatology, and sometimes interventional radiology, with delivery typically scheduled by caesarean hysterectomy in a controlled setting. Management strategies focus on minimizing haemorrhagic complications and ensuring maternal safety. Despite advances in prenatal diagnosis and surgical techniques, placenta praevia with accreta remains a leading cause of severe obstetric haemorrhage and peripartum hysterectomy. The suspected bladder invasion noted intraoperatively further classifies this case as likely placenta percreta, which occurs in approximately 20–30% of PAS cases with bladder involvement [4].
The management of this case exemplifies best practices for placenta percreta. Early recognition of placenta previa via bedside ultrasound, combined with a planned caesarean hysterectomy at 34 weeks, mitigated the risk of catastrophic haemorrhage, reported to occur in up to 90% of percreta cases with blood loss often exceeding 2,000 mL [1, 4]. The multidisciplinary approach, involving obstetrics, anaesthesia, ICU, urology, vascular surgery, and neonatology, was critical in ensuring a successful outcome. Preparation of 10 units of packed red blood cells (PRBCs), fresh frozen plasma (FFP), and platelets, along with intraoperative transfusions, addressed the high risk of coagulopathy and haemorrhage, which complicates 10–20% of severe PAS cases [2]. The decision to perform a hysterectomy was appropriate given the placenta’s morbid adherence and invasion into the bladder, as conservative management (e.g., leaving the placenta in situ) carries a 20–40% risk of delayed haemorrhage or infection [4, 5].
Compared to the literature, this case is notable for its successful outcome in a potentially resource-constrained setting, as the patient was awaiting transfer to a higher centre. The lack of an MRI report preoperatively, which could have confirmed percreta, highlights a limitation in diagnostic precision. However, clinical suspicion based on risk factors and ultrasound findings guided appropriate management, aligning with American College of Obstetricians and Gynaecologists (ACOG) recommendations for presumed PAS [1]. The absence of significant postoperative complications, such as infection or thromboembolism, despite the patient’s ICU admission and use of DVT prophylaxis show good outcome overall for this case. This case offers several educational points. First, it emphasizes the importance of regular antenatal care to avoid emergency unplanned scenarios, a high index of suspicion for placenta accreta/percreta in patients with multiple prior caesareans and placenta previa. Second, it demonstrates the value of optimizing the patients condition and planning with multidisciplinary team, and blood product preparedness in reducing maternal morbidity, which ranges from 50–70% in percreta cases [4]. Third, it highlights challenges in non-tertiary settings, where delays in advanced imaging or transfer can complicate management. Future research should focus on improving access to early MRI diagnostics and optimizing conservative management strategies for women desiring fertility preservation, though hysterectomy remains the standard for percreta due to its high success rate [5].
Limitations: The primary limitation is the lack of MRI confirmation of placenta percreta, as the report was pending at the time of surgery. Additionally, long-term follow-up data on maternal and neonatal outcomes were not available in the provided records, limiting insights into potential delayed complications. Finally, the case was managed in a facility awaiting transfer, suggesting potential resource limitations that may not reflect outcomes in tertiary centres.
Conclusion
This case of placenta previa major with suspected placenta accreta/percreta in a multiparous woman with prior caesarean sections illustrates the critical role of early diagnosis, multidisciplinary coordination, and timely caesarean hysterectomy in preventing life-threatening complications. The good maternal and foetal outcomes highlight the efficacy of proactive surgical planning and robust perioperative management. Clinicians should maintain vigilance for placenta accreta spectrum disorders in high-risk patients and ensure comprehensive preparation to optimize outcomes in similar cases.
References
1. Royal College of Obstetricians and Gynaecologists. Placenta praevia, placenta accreta and vasa praevia: diagnosis and management. Green-top Guideline No. 27. London: RCOG; 2011. Available from: https://www.rcog.org.uk/en/guidelines-research-services/guidelines/gtg27/
2. Silver RM. Placenta Accreta Spectrum: Pathophysiology and Management. Obstet Gynecol. 2015 Sep;126(3):654-66. doi: 10.1097/AOG.0000000000001118.
3. NHS. Placenta praevia. Available at: https://www.nhs.uk/conditions/placenta-praevia/ [Accessed 2025 Jul 8].
4. American College of Obstetricians and Gynecologists; Society for Maternal-Fetal Medicine. Obstetric Care Consensus No. 7: Placenta Accreta Spectrum. Obstet Gynecol. 2018 Dec;132(6):e259-e275. doi:10.1097/AOG.0000000000002983.
5. Silver RM, Landon MB, Rouse DJ, Leveno KJ, Spong CY, Thom EA, et al. Maternal morbidity associated with multiple repeat cesarean deliveries. Obstet Gynecol. 2006 Dec;107(6):1226-32. doi:10.1097/01.AOG.0000219750.79480.84.
6. Belfort MA. Placenta accreta. Am J Obstet Gynecol. 2010 Nov;203(5):430-9. doi:10.1016/j.ajog.2010.03.011.
7. Wu S, Kocherginsky M, Hibbard JU. Abnormal placentation: Twenty-year analysis. Am J Obstet Gynecol. 2005 May;192(5):1458-61. doi:10.1016/j.ajog.2004.12.074.
8. Sentilhes L, Kayem G, Chandraharan E, Palacios-Jaraquemada J, Jauniaux E. FIGO consensus guidelines on placenta accreta spectrum disorders: Conservative management. Int J Gynaecol Obstet. 2018 Apr;140(3):291-298. doi:10.1002/ijgo.12407.
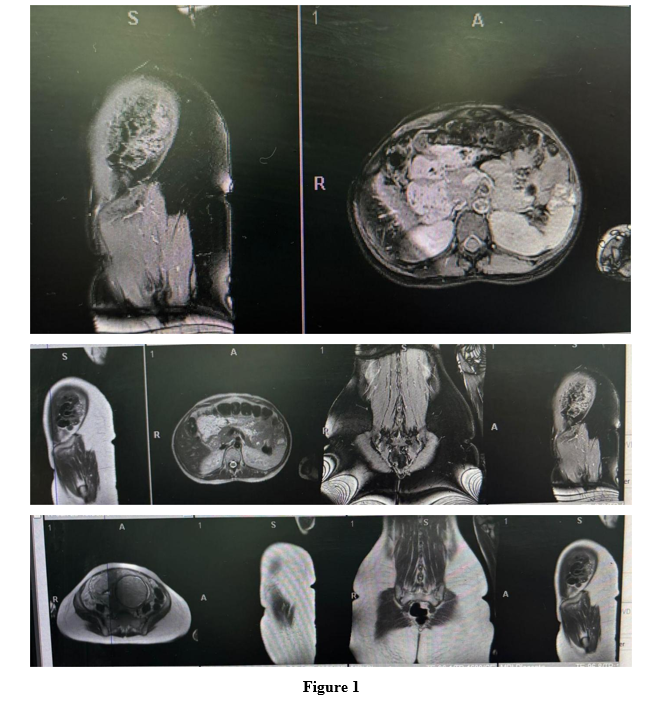
Figure 1