Comparative Assessment of Clinical Effectiveness and Patient Acceptability of Hawley and Vacuum-Formed Retainers- An Analytical Study
Comparative Assessment of Clinical Effectiveness and Patient Acceptability of Hawley and Vacuum-Formed Retainers- An Analytical Study
Dr. Preeti Bhattacharya1, Dr. Abhishek Singh2*, Dr. Anil Kumar Chandna3, Dr. Ankur Gupta4, Dr. Ravi Bhandari5, Dr. Resham Irshad6
Dr. Preeti Bhattacharya - Head of the Department
Dr. Abhishek Singh - Post graduate studentIntern Medical officer at Vydehi Institute of Medical Sciences and Research Centre , Bengaluru, Karnataka, India"
Dr. Anil Kumar Chandna - Director of PG studies
Dr. Ankur Gupta - Professor
Dr. Ravi Bhandari - Professor
Dr. Resham Irshad - Senior Lecturer
Workplace: Institute of Dental Sciences, Bareilly, India
*Correspondence to: Dr. Abhishek Singh, Post Graduate student, Department of Orthodontics and Dentofacial Orthopaedics, Institute of Dental Sciences, Near Suresh Sharma Nagar, Pilibhit bypass road, Bareilly. Pin Code 243006
Copyright.
© 2025 Dr. Abhishek Singh This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 21 Aug 2025
Published: 18 Sep 2025
DOI: https://doi.org/10.5281/zenodo.17181190
ABSTRACT
Background: Post-orthodontic retention is critical to prevent relapse and ensure long-term treatment stability. Among removable retainers, Hawley Retainers (HR) and Vacuum-Formed Retainers (VFR) are the most commonly prescribed.
Aim: To evaluate and compare the clinical effectiveness and patient acceptance with Hawley retainers and Vacuum-formed retainers.
Material and Methods: A total of 45 patients who completed fixed orthodontic treatment were randomly assigned to either HR (Group I) or VFR (Group II). Retainers were worn full-time for 6 months and at night for 3 months. Data were collected at debonding (T0), 3 months (T1), and 9 months (T2). Parameters assessed included archwidth changes (using dental casts), occlusal contacts (using Aluwax impressions), and patient acceptability (using a 10-point Visual Analogue Scale).
Results: Arch Width: Significant intergroup differences were found, with Group II showing greater archwidth changes . Occlusal Contacts: Both groups showed an increase in anterior, posterior, and total occlusal contacts from T0 to T1; however, Group I demonstrated a significantly increase in contact points. Patient Acceptance: Group II shows statistically significant differences in appearance, speech, and self-esteem. Other parameters showed non-significant differences but trend was in favor of Group II.
Conclusion: Both HR and VFR are clinically effective in maintaining orthodontic outcomes. HR promotes better occlusal settling, whereas VFR are more favored by patients for aesthetics and comfort. Clinical choice should consider both functional stability and patient preference.
Keywords: Hawley, Essix, Retainer, Retention Techniques, VFR.
Comparative Assessment of Clinical Effectiveness and Patient Acceptability of Hawley and Vacuum-Formed Retainers- An Analytical Study
Background
The success of orthodontic treatment mainly depends on retaining the teeth in the corrected position after the debonding appointment as they are potentially unstable therefore retention is necessary1. Retention is maintained through orthodontic retainers, which can either be fixed or removable. Removable retainers which are commonly used are Hawley retainers (HR) and vacuum formed retainers (VFR).2,3 HR have been a reliable and effective option for removable orthodontic retention for more than a century. Since the advent of VFR in 1971, it has become increasingly popular. Successful outcome of any retention device depends on its ability to maintain archform, preventing undesirable tooth shifting while allowing required settling.4 Effectiveness also depends on patient’s compliance which in turn again linked to its acceptability.
A study done by Tarman ke, et al. aimed to compare patient acceptance and satisfaction with two types of removable retainers, concluded that VFR were preferred for speech comfort, while no substantial differences were found between the two retainers in other aspects of patient perception.5
Kalaydzhieva M, et al. evaluated the effectiveness of Hawley retainers, Vacuum-formed retainers and fixed retainers in maintaining dental arch dimensions and tooth alignment and found that Vacuum-formed retainers were superior in maintaining maxillary anterior alignment, while Hawley retainers preserved maxillary arch length. Both types of retainers showed no significant difference in maintaining transverse dimensions, intercanine width, interpremolar width and intermolar width.6
The objective of this study was to compare archwidth and how occlusal contacts in maximum intercuspation change over time during the post-retention period, as well as to assess patient compliance in individuals wearing HR and those wearing VFR.
Materials and Methods
Study Design and Population
The study was conducted in the Department of Orthodontics, Institute of Dental Sciences, Bareilly. A total of 45 subjects who completed fixed appliance orthodontic treatment were included. Ethical clearance and informed consent were obtained prior to study commencement.
Patients included in the study had not undergone any prior orthodontic treatment other than that which was provided at the Institute of Dental Science. Additionally, all selected patients were treated using fixed orthodontic appliances in both jaws, following the 0.022-inch slot MBT prescription.
Patients were excluded from the study if they had received single arch or sectional fixed appliance treatment, had undergone Rapid Maxillary Expansion, or required prosthetic treatment for missing teeth. Additionally, individuals with learning disabilities, cleft lip and palate, poor periodontal status, or temporomandibular disorders were not included in the study.
Participants were then randomly allocated to receive either Hawley Retainer (HR) or Vacuum-Formed Retainers (VFR) in both arches [Figure 1]. Based on the type of retainer provided, they were divided into two groups:
Group - I: Subjects who were given Hawley Retainers
Group - II: Subjects who were given Vacuum Formed Retainers
Figure 1 - (A) Hawley retainer; (B) Vacuum- formed retainer
Intervention and Procedure
Hawley Retainers were fabricated using acrylic resin and 21-gauge stainless steel wire. In patients who had undergone premolar extraction, a long labial bow extended from second premolar of 1st quadrant to second premolar of 2nd quadrant and C clasps on the first molars were incorporated. For non-extraction cases, a short canine-to-canine labial bow with Adams clasps on the first molars were used. The labial bow was adjusted to make light contact with the labial surfaces of the incisors.
Vacuum-Formed Retainers (VFR) were made from 1 mm thick polyvinyl siloxane sheets. These were trimmed to extend 1–2 mm over the labial gingiva and 3–4 mm over the palatal or lingual gingiva, covering the occlusal surfaces of all teeth, including the most distally erupted molar.
Retainers were delivered and fitted within 24 hours of debonding. Participants were instructed to wear their retainers full-time for the first 6 months, followed by nighttime wear thereafter. Retainers were advised to be removed only during meals, cleaning, and drinking hot beverages. Fit and adaptation were checked during each follow-up appointment.
Collection of Data
Dental Casts
The maxillary and mandibular dental casts were obtained from all patients at 3 points in time. The first set of records were taken at T0 (at the time of debonding); the second set at T1 (3 months after delivery of retainers) and third set at T2 (9 months after delivery of retainers).
Occlusal Records
Occlusal records were obtained from all patients at two points of time i.e immediately after debonding (T0) and after three months (T1), using Aluwax bite registration. Subjects were made to sit upright, and softened Aluwax was placed on the mandibular occlusal surfaces. Patients were guided to bite in maximum intercuspation firmly and maintain the position for about two minutes. In cases where the initial registration was inadequate due to insufficient material or improper placement, a second bite registration was performed.[Figure 2]
Figure 2 - Occlusal record using Aluwax
Patient Acceptability Assessment
Subjects were evaluated three months after retainer placement (T1) using a 10-cm Visual Analogue Scale (VAS). It consisted of 10 questions related to retainer acceptance. Both oral and written instructions were provided to ensure proper completion of the questionnaire, which ranged from 0 (most favorable response) to 10 (least favorable). The assessments were conducted in the presence of the treating doctor. [Figure 3]
Figure 3 - Visual Analogue Scale (VAS)
Analysis of Data
Measurement on Dental cast
Maxillary and mandibular dental casts were obtained for each subject, and transverse arch dimensions were recorded using an electronic digital caliper (Mitutoyo Digital Vernier Caliper 0–150 mm) with a precision of 0.01 mm . For the maxillary cast, four measurements were taken: Intercanine Width (ICW), defined as the distance between the cusp tips of the right and left canines; Interpremolar Width (IPMW), measured between the buccal cusp tips of the second premolars on both sides; Interfirst Molar Width 1 (IFMW1), the distance between the mesiobuccal cusp tips of the first molars on the right and left quadrants; and Interfirst Molar Width 2 (IFMW2), the distance between the distobuccal cusp tips of the first molars [Figure 4]. Similarly, for the mandibular cast, the same parameters were recorded.
Figure 4: (A) & (B) Shows archwidth measurement in maxillary and mandibular arch respectively
Measurement on occlusal records
Interocclusal records were analyzed on a radiographic viewing screen in a dark room to identify areas of perforation and translucent zones without perforation. Contact points were assessed for the first molars, second premolars, canines, lateral incisors, and central incisors. Anterior contacts included central incisors, lateral incisors, and canines, while posterior contacts included the first molars and second premolars. The total occlusal contacts were determined by summing the anterior and posterior contact counts.
Measurement of VAS for patient acceptability
Subjects marked a vertical line on the Visual Analogue Scale (VAS) for each parameter, which was then measured using a metallic ruler from right to left. Marks closer to the left indicated a more favorable response, while those near the right indicated a less favorable one.
Result
The age distribution of the study population revealed no statistically significant difference between the two groups. The mean age in Group I was 16.30?±?2.75 years, while in Group II it was 16.04?±?3.56 years, indicating comparable age profiles. In terms of gender distribution, Group I demonstrated a relatively balanced representation of males (52.2%) and females (47.8%). In contrast, Group II had a higher proportion of females (68.2%) compared to males (31.8%). The kappa statistic for intra-examiner reliability was 0.97 (p?=?0.00000023), indicating excellent agreement, while the inter-examiner reliability was 0.88 (p?=?0.00017), also reflecting a high level of consistency and agreement between observers.
Table 1: Intergroup comparison of changes in maxillary arch width measurements from T1-T0, T2-T1 and T2-T0 between Group I and Group II using Unpaired t test
|
Parameters |
TIME PERIOD |
Group I (HR) |
Group II (VFR) |
P- Value |
|
ICW |
T1-T0 |
0.250 |
0.413 |
0.00000000378 |
|
T2-T1 |
0.360 |
0.124 |
0.00000218 |
|
|
T2-T0 |
0.611 |
0.538 |
0.0000000991 |
|
|
IPMW |
T1-T0 |
0.134 |
0.480 |
0.000000000086 |
|
T2-T1 |
0.066 |
0.289 |
0.00000000108 |
|
|
T2-T0 |
0.200 |
0.77 |
0.0000000644 |
|
|
IFMW1 |
T1-T0 |
0.287 |
0.555 |
0.000000000517 |
|
T2-T1 |
0.131 |
0.166 |
0.00000177 |
|
|
T2-T0 |
0.418 |
0.721 |
0.000000000316 |
|
|
IFMW2 |
T1-T0 |
0.411 |
0.44 |
0.0075 |
|
T2-T1 |
0.111 |
0.05 |
0.000463 |
|
|
T2-T0 |
0.522 |
0.49 |
0.00528 |
P<0.05 considered as statistically significant
Table 1 shows an inter-group comparison of maxillary arch width changes between Group I and Group II across the various time intervals i.e, T1–T0, T2–T1, and T2–T0 . Statistically significant differences for all four measurements i.e Intercanine Width (ICW), Interpremolar Width (IPMW), Interfirst Molar Width 1 (IFMW 1), and Interfirst Molar Width 2 (IFMW 2) were found between the two groups. Group II consistently showed greater mean differences than Group I during the T1–T0 interval, suggesting more substantial arch width changes in the early retention period. Although significant differences were also observed during the T2–T1 and T2–T0 intervals, no consistent pattern of increase or decrease in arch width was evident within either group across all time intervals.
Table 2 : Intergroup comparison of changes in mandibular arch width measurements from T1-T0, T2-T1 and T2-T0 between Group I and Group II using Unpaired t test
|
Parameters |
TIME PERIOD |
Group I (HR) |
Group II (VFR) |
P- Value |
|
ICW |
T1-T0 |
0.390 |
0.06 |
0.00000253 |
|
T2-T1 |
0.052 |
0.13 |
0.000177 |
|
|
T2-T0 |
0.443 |
0.20 |
0.00000194 |
|
|
IPMW |
T1-T0 |
0.073 |
0.85 |
0.0000000187 |
|
T2-T1 |
0.035 |
1.06 |
0.00000000616 |
|
|
T2-T0 |
0.108 |
1.91 |
0.00000000645 |
|
|
IFMW1 |
T1-T0 |
0.13 |
0.23 |
0.000385 |
|
T2-T1 |
0.12 |
1.39 |
0.0000000102 |
|
|
T2-T0 |
0.253 |
1.62 |
0.00000000195 |
|
|
IFMW2 |
T1-T0 |
0.255 |
0.42 |
0.0000091 |
|
T2-T1 |
0.064 |
0.84 |
0.0000000187 |
|
|
T2-T0 |
0.32 |
0.41 |
0.000385 |
P<0.05 considered as statistically significant
Further inter-group comparisons of mandibular arch width changes are shown in Table 2. Statistically significant differences between the two groups for all four mandibular arch width measurements i.e T1–T0, T2–T1, and T2–T0 were found. As with the maxillary arch, the majority of measurements displayed higher mean differences in Group II compared to Group I, suggesting greater dimensional changes in the Vacuum-Formed Retainer group. However, similar to the maxillary arch, no uniform pattern of change was observed within either group.
Table 3 : Intergroup comparison of changes in anterior, posterior and overall occlusal contact points from T0 and T1 between Group I and Group II using Unpaired t test
|
Parameter |
Time Interval |
Group I(HR) |
Group II(VFR) |
P Value |
|
Anterior Contact points |
T1-T0 |
1.65 |
0.59 |
0.0000000211 |
|
Posterior Contact points |
T1-T0 |
2.87 |
0.59 |
0.000000000987 |
|
Total Contact points |
T1-T0 |
4.48 |
1.27 |
0.00000000251 |
P<0.05 considered as statistically significant
Table 3 presents the inter-group comparison of mean differences in occlusal contact points between T1 and T0 for both groups. The results demonstrate that Group I exhibited a significantly higher mean difference than Group II for anterior, posterior, and total contact points. These findings suggest superior occlusal settling in patients with Hawley Retainers compared to those with Vacuum-Formed Retainers during the initial three months of retention.
Table 4 : Intergroup Comparison of parameters assessed using VAS Scale between Group I and Group II using Unpaired t test
|
PARAMETER |
GROUP I(HR) MEAN+SD |
GROUP II(VFR) MEAN+SD |
P Value |
|
Appearance |
7.18± 2.57 |
8.74±1.32 |
0.0147* |
|
Teeth biting |
8.03± 2.31 |
7.84± 1.80 |
0.762 |
|
Durability |
8.05± 1.76 |
8.80± 0.84 |
0.0812 |
|
Self Esteem |
7.70±1.85 |
8.90±1.14 |
0.0129* |
|
Fitting of Retainer |
8.22±1.81 |
8.83± 1.32 |
0.207 |
|
Gum Irritation |
7.86±2.11 |
8.41±1.81 |
0.353 |
|
Oral hygiene |
8.10±2.03 |
8.61±1.72 |
0.363 |
|
speech |
7.21±2.73 |
8.73± 1.49 |
0.0271* |
|
swallowing |
7.79±2.45 |
8.75±1.03 |
0.0964 |
|
Overall comfort |
8.26±1.40 |
8.87±1.20 |
0.125 |
P<0.05 considered as statistically significant
Table 4 showed comparision of various parameters assessed using the Visual Analogue Scale (VAS) at T1 between Group I and Group II. The assessments were carried out for ten parameters based on the patients' acceptance towards retainers.
A statistically significant difference was observed for the parameter of appearance, with Group II showing a significantly higher mean VAS score compared to Group I (p = 0.0147), indicating greater aesthetic satisfaction. Similarly, the self-esteem scores were significantly higher in Group II (p = 0.0129), suggesting a more positive psychosocial response to VFRs. The parameter assessing speech also demonstrated a statistically significant difference, with higher VAS scores reported by Group II subjects (p = 0.0271), reflecting better speech-related adaptation.
For the parameters of retainer fitting, gum irritation, oral hygiene, swallowing, and overall comfort, no statistically significant differences were observed between the two groups. However, mean VAS scores for all these parameters were marginally higher in Group II, suggesting a slight preference toward VFRs, though not statistically significant.
The only parameter where Group II reported a lower mean VAS score was teeth biting, but this difference was also statistically insignificant, indicating comparable performance of both retainer types in this regard.
Discussion
Significant differences in arch width changes were observed between the two retainer groups across all time intervals (T0–T1, T1–T2, and T0–T2), with Group II exhibiting higher mean difference, particularly from T0 to T1. This suggests that the Group II experienced more noticeable changes in maxillary arch width during the retention period. Similar patterns were observed in the mandibular arch, where Group II also showed greater changes in most measurements compared to Group I, indicating that Group II had lowered arch width stability.Previous studies, such as those by Rowland et al.7 and Demir et al.8 reported minimal or statistically insignificant differences between HR and VFR in terms of arch width changes. However, the present findings suggest that VFR may allow more dimensional variation over time, while HR demonstrated better long-term arch width maintenance. Ramazanzadeh et al.1 also found minimal changes with both types of retainers, though differences in retention protocols may account for the discrepancies between studies.Overall, both retainers are clinically effective, but HR may offer slightly greater arch width stability during prolonged retention.
In this study, anterior, posterior, and total occlusal contact points were assessed at T0 and T1 in patients using HR and VFR. On comparing the two groups, Group I demonstrated statistically significant increases in the anterior, posterior, and total contact points than group II. Our findings align with studies of Sauget et al.9 who similarly observed increased contact points in the anterior teeth after 3 months of retention with Hawley retainers. Additionally, Durbin DS and Sakowsky C10 reported a notable increase in posterior contact points with the use of Hawley retainers, further supporting the robustness of our findings. Sauget et al.9 found that VFR did not show an increase in anterior, posterior, or total occlusal contact points. Presence of retainer material between the teeth could have inhibited complete occlusal settling.
Patient acceptability was assessed using a 10-cm Visual Analogue Scale (VAS), which has been widely used in research due to its sensitivity in detecting changes in patient satisfaction and retainer acceptance. In the present study,with regard to appearance showed a statistically significant difference between Group I and Group II was found, with VFRs rated as more aesthetically pleasing. This finding aligns with previous studies by Hichens et al.,11 Saleh et al.,9 and Rowland et al.7 The transparent nature of VFRs contributes to their higher aesthetic acceptance. However, Pratt et al.12 reported no significant difference, possibly due to the retrospective design of the study and longer follow-up periods.
Regarding speech, our study found a statistically significant difference between the two groups, with Group II reporting higher VAS scores than Group I . These results are consistent with the findings of Hichens et al.11 and Saleh et al.9 who also observed better speech comfort with VFRs. The minimal palatal coverage of VFR likely reduces tongue interference during speaking, leading to greater patient satisfaction.
Additionally, self-esteem was significantly higher in Group II, with a higher VAS score compared to Group I, which is consistent with the findings of Saleh et al.9 Better effects with VFR may be attributed to the clear appearance of VFRs, reduced visibility, and less impact on speech when the retainer is in place.
No significant differences were found for biting ability, although the VAS score was higher in Group I than in Group II. In terms of durability, while the difference was not statistically significant, the VAS score was slightly higher in Group II compared to Group I. Hichens et al.11 reported more frequent breakage with HRs, whereas Saleh et al.,9 Pratt et al.,12 and Ashari et al.13 found VFR to be more prone to damage.For fitting, no statistical difference was observed, although the VAS score was higher in Group II than in Group I. These results are supported by Saleh et al.9 and Ashari et al.13 Similarly, gum irritation and oral hygiene showed no significant differences, although Group II had slightly higher scores in both categories. Saleh et al.9 also observed less gingival irritation with VFR, likely due to the absence of retentive wire. No statistically significant difference in overall comfort was found between the two groups, although Group II showed a slightly higher VAS score than Group I. These findings align with Ashari et al.13 and Hichens et al.,11 while Saleh et al.9 reported significantly greater comfort with VFR.
Conclusion
The findings of this study suggest that both HR and VFR are effective in maintaining post-treatment arch width. However, when compared, HR demonstrated better arch width stability than VFR during the initial 3-month period. In terms of occlusal contact, HR demonstrated a statistically significant increase in anterior, posterior, and total contact points compared to VFR, indicating better occlusal settling with HR.
VFR showed statistically significant higher VAS scores for appearance, self-esteem, and speech, indicating better patient acceptance compared to Hawley retainers. VFR showed higher, though not statistically significant, VAS scores compared to HR in fit, gum irritation, oral hygiene, swallowing, and overall comfort, indicating slightly better acceptance.
References
1. Ramazanzadeh B, Ahrari F, Hosseini ZS. The retention characteristics of Hawley and vacuum-formed retainers with different retention protocols. Journal of clinical and experimental dentistry. 2018 Mar 1;10(3):e224. DOI: 10.4317/jced.54511.
2. Hawely CA. A removable retainer. Int J Orthod Oral Surg 1919;2:291-8. DOI: 10.1016/S1072-348X(19)80039-6.
3. Sheridan JJ, Ledoux W, Mcminn R. Essix retainers: fabrication and supervision for permanent retention.J Clin Orthod 1993;27:37-45. PMID: 8478438
4. Ba?çiftçi FA, Uysal T, Sari Z, Inan O. Occlusal contacts with different retention procedures in 1-year follow-up period. American journal of orthodontics and dentofacial orthopedics. 2007 Mar 1;131(3):357-62. DOI: 10.1016/j.ajodo.2005.05.052
5. Tarman KE, Jazaldi F, Latief AA, Soegiharto BM. Difference in acceptance and satisfaction perception on the use of Hawley and vacuum-formed retainers among post-orthodontic patients. APOS Trends in Orthodontics. 2024 Jul 5:1-8. DOI:10.25259/APOS_60_2024
6. Kalaydzhieva M, Krasteva S, Stoilova-Todorova M, Todorova-Plachyiska K, Georgiev K. Assessment of the effectiveness of two different orthodontic retention protocols. Folia Medica. 2023 Aug 31;65(4):644-50. DOI: 10.3897/folmed.65.e85525
7. Rowland H, Hichens L, Williams A, Hills D, Killingback N, Ewings P, Clark S, Ireland AJ, Sandy JR. The effectiveness of Hawley and vacuum-formed retainers: a single-center randomized controlled trial. American Journal of Orthodontics and Dentofacial Orthopedics. 2007 Dec 1;132(6):730-7. DOI: 10.1016/j.ajodo.2006.06.019
8. Barlin S, Smith R, Reed R, Sandy J, Ireland AJ. A retrospective randomized double-blind comparison study of the effectiveness of Hawley vs vacuum-formed retainers. The Angle Orthodontist. 2011 May 1;81(3):404-9. DOI: 10.2319/072610-437.1
9. Sauget E, Covell Jr DA, Boero RP, Lieber WS. Comparison of occlusal contacts with use of Hawley and clear overlay retainers. The Angle Orthodontist. 1997 Jun 1;67(3):223-30. DOI: 10.1043/0003-3219(1997)067<0223:COOCWU>2.3.CO;2
10. Durbin DS, Sadowsky C. Changes in tooth contacts following orthodontic treatment. American journal of orthodontics and dentofacial orthopedics. 1986 Nov 1;90(5):375-82. DOI: 10.1016/0889-5406(86)90003-x
11. Hichens L, Rowland H, Williams A, Hollinghurst S, Ewings P, Clark S, Ireland A, Sandy J. Cost-effectiveness and patient satisfaction: Hawley and vacuum-formed retainers. The European Journal of Orthodontics. 2007 Aug 1;29(4):372-8. DOI: 10.1093/ejo/cjm039
12. Pratt MC, Kluemper GT, Lindstrom AF. Patient compliance with orthodontic retainers in the postretention phase. American Journal of Orthodontics and Dentofacial Orthopedics. 2011 Aug 1;140(2):196-201. DOI: 10.1016/j.ajodo.2010.02.035.
13. Ashari A, Xian L, Syed Mohamed AM, Wahab RM, Kit YC, Tata MD, Sinnasamy S, Kuppusamy E. One-year comparative assessment of retention of arch width increases between modified vacuum-formed and Hawley retainers: A multicenter randomized clinical trial. The Angle Orthodontist. 2022 Mar 1;92(2):197-203. DOI: 10.2319/050921-363.1.
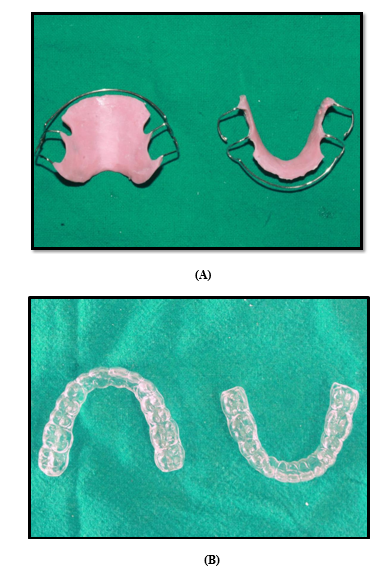
Figure 1

Figure 2
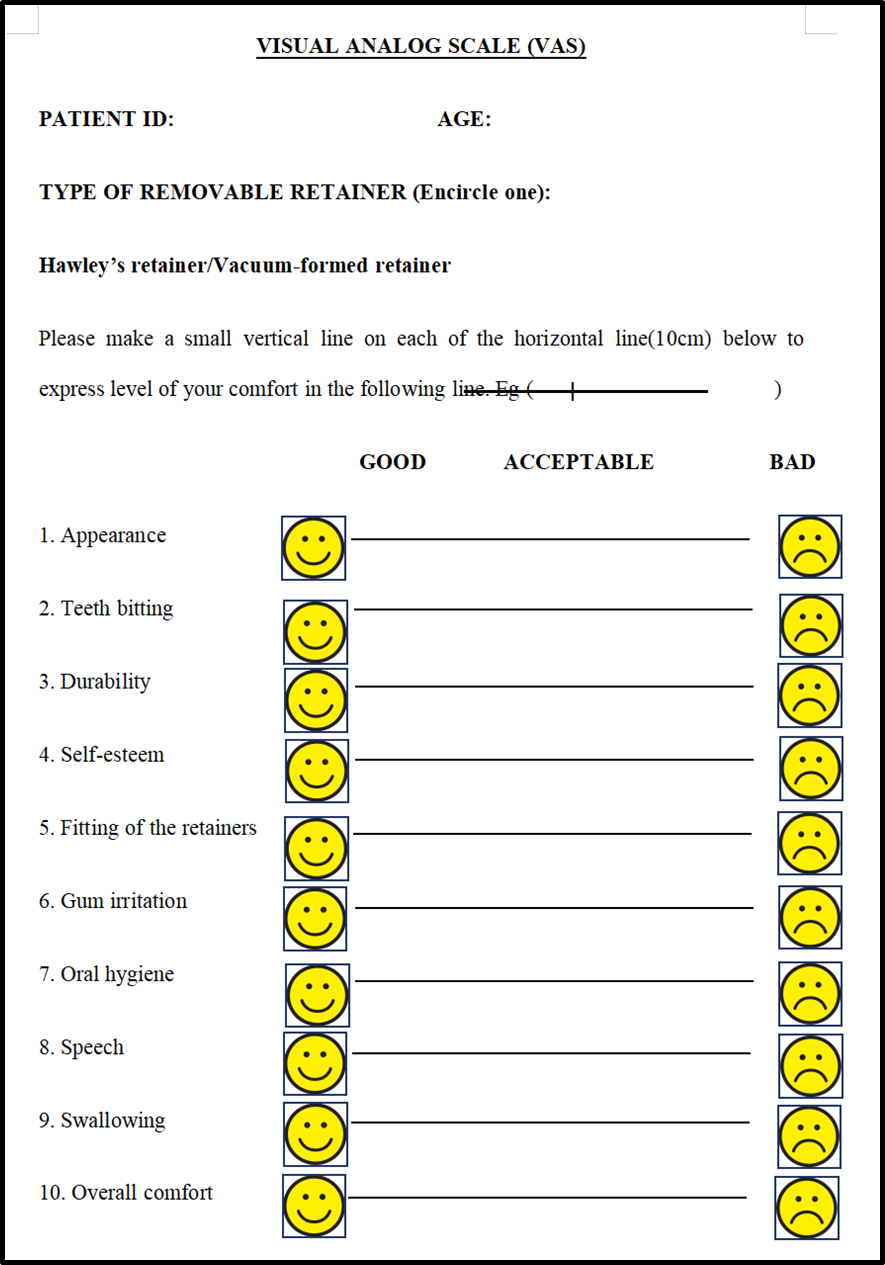
Figure 3
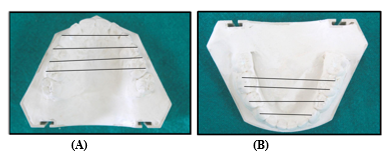
Figure 4