Smile Width in Orthodontic Treatment: A Clinical Review of Expansion and Interproximal Reduction Approaches.
Smile Width in Orthodontic Treatment: A Clinical Review of Expansion and Interproximal Reduction Approaches.
Michael B. Guess *
*Correspondence to: Michael B. Guess, DDS, MS, MA, El Dorado Hills, CA Private Practice.
Copyright.
© 2025 Michael B. Guess, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 25 Sep 2025
Published: 01 Oct 2025
ABSTRACT
Background: The desire for broader, more attractive smiles drives much of contemporary orthodontic treatment demand. Understanding the evidence surrounding smile width enhancement helps clinicians make informed decisions about treatment approaches.
Objective: To review the current literature on smile width assessment and compare the effectiveness of arch expansion versus interproximal reduction (IPR) for enhancing smile aesthetics.
Methods: This clinical review examines orthodontic literature from major databases, focusing on studies that provide quantitative or qualitative data on smile aesthetics, buccal corridors, arch expansion outcomes, and interproximal reduction results.
Results: Research consistently demonstrates preference for broader smiles with reduced buccal corridors. Arch expansion reliably increases transverse dimensions but requires careful attention to long-term retention. IPR effectively creates space for alignment without enhancing smile width. Treatment success varies significantly between adolescent and adult patients.
Conclusions: Both expansion and IPR serve important roles in orthodontic treatment, but their applications for smile enhancement differ considerably. Expansion directly addresses smile width concerns when combined with appropriate retention protocols, while IPR remains valuable for space management without aesthetic width benefits.
Clinical Significance: This review helps clinicians understand when and how to apply different treatment modalities to optimize smile aesthetics while maintaining realistic expectations about outcomes and stability.
Smile Width in Orthodontic Treatment: A Clinical Review of Expansion and Interproximal Reduction Approaches.
Introduction
Walk into any orthodontic practice today, and you'll quickly notice that patient concerns have evolved. While traditional issues like crowding and bite problems remain important, an increasing number of patients specifically request "a wider smile" or express dissatisfaction with their "narrow smile." This shift toward aesthetic-driven treatment has pushed clinicians to better understand the relationship between orthodontic procedures and smile width.
The concept of smile width, typically assessed through buccal corridor evaluation, has gained significant attention in recent years. Yet despite its importance in treatment planning, many practitioners remain uncertain about which treatment approaches most effectively address smile width concerns and how stable these changes prove over time.
This review examines the current evidence on smile width assessment and treatment, comparing the effectiveness of two primary approaches: arch expansion and interproximal reduction. Rather than presenting definitive answers to complex clinical questions, this discussion aims to help clinicians navigate the available evidence and make informed decisions about treatment selection.
Literature Review Approach
The literature on smile aesthetics spans several decades and includes diverse study designs, from preference surveys to long-term stability analyses. This review focuses on studies that provide meaningful data for clinical decision-making, with particular attention to those offering quantitative outcomes or validated assessment methods.
Key areas examined include aesthetic preference studies, arch expansion outcomes, interproximal reduction results, and long-term stability data. While the heterogeneity of study designs limits direct comparisons, consistent patterns emerge across the literature that inform clinical practice.
Image 1 Buccal Corridor Attractiveness( Fig 5)
More Attractive Less Attractive
Smile Aesthetics and Buccal Corridor Preferences
What Patients and Professionals Prefer
The foundational work by Moore and colleagues in 2005 demonstrated that laypeople consistently preferred broader smiles over narrower ones when evaluating digitally modified photographs (2). Their study found that smiles with minimal buccal corridors (around 2%) were rated more attractive than those with larger corridors (15% or more) (Image 1). This preference appeared consistent across both male and female evaluators.
Figure 1: Both laypeople and professionals consistently rated broader smiles (2-10% buccal corridors) as most attractive, with preferences declining significantly as corridor width increased beyond 15%.
Subsequent studies have largely confirmed these findings. Parekh and colleagues extended this work by including both orthodontists and laypeople in their evaluations, finding remarkable agreement between groups regarding buccal corridor preferences (3). The sweet spot appears to be somewhere between 2-10% buccal corridor space, with attractiveness ratings declining as corridors become more prominent.
Cultural Considerations
Interestingly, some cultural variation exists in these preferences. Studies from Japan and Korea suggest somewhat greater tolerance for narrower smiles compared to Western populations, though even in these cultures, excessively narrow smiles receive lower attractiveness ratings (5). This cultural component reminds us that treatment planning should consider individual patient backgrounds and preferences rather than applying universal standards.
Clinical Assessment Challenges
While these preference studies provide valuable insights, translating them into clinical practice presents challenges. Standardized photography protocols become crucial for reliable assessment, and practitioners must consider that smile width preferences exist within broader facial aesthetic contexts. A smile that appears narrow in isolation might seem perfectly proportioned when viewed within an attractive facial frame.
Arch Expansion: Outcomes and Considerations
What Expansion Actually Achieves
When we talk about arch expansion in the context of smile width, we're primarily discussing its effect on transverse dimensions and the resulting changes in buccal corridor display. The literature on expansion outcomes shows relatively predictable dimensional changes, though the specific amounts vary based on appliance type, patient age, and treatment duration.
Studies examining rapid maxillary expansion typically report intercanine width increases in the range of 2-4 mm, with somewhat larger changes in the premolar and molar regions. These dimensional changes translate into measurable reductions in buccal corridor space, which aligns with aesthetic preferences identified in the preference studies.
Figure 2: Expansion produces significant arch width increases across all regions, while IPR provides space creation without smile width enhancement. This fundamental difference guides treatment selection for patients seeking broader smiles.
The Age Factor
One of the most important considerations in expansion treatment is patient age. The literature consistently demonstrates superior outcomes in younger patients, particularly those with patent midpalatal sutures. Adolescent patients typically show greater skeletal contribution to expansion and better long-term stability compared to adults.
Adult expansion tends to involve more dental tipping and less true skeletal change. This doesn't necessarily preclude expansion in adult patients, but it does require different expectations and retention protocols.
Stability Challenges
The most significant concern with expansion treatment relates to long-term stability. Studies with extended follow-up periods report significant relapse rates, particularly in the anterior region. The intercanine area appears most vulnerable to relapse, with some studies reporting return toward pre-treatment dimensions in a substantial percentage of cases.
Figure 3: Long-term stability varies by region, with the canine area showing highest relapse potential and the molar region demonstrating better stability. This pattern emphasizes the critical importance of permanent retention, particularly in the aesthetic zone.
This stability challenge doesn't invalidate expansion as a treatment option, but it underscores the critical importance of permanent retention. Fixed lingual retainers become essential for maintaining expansion results, particularly in the aesthetic zone where relapse would be most noticeable.
Modern Expansion Approaches
Recent literature has explored expansion through clear aligner systems, offering new possibilities for adult patients. While early studies suggest promise, the data on long-term stability and smile width enhancement through aligners remains limited. These approaches may prove valuable for mild expansion needs, but Marpe and traditional expansion methods likely remain superior for significant transverse deficiencies.
Image 2. Expansion of the 1st and 2nd bicuspid region achieved without flaring the lower incisors (Fig 6)
Expansion is most stable in descending order : 1st molar 2nd bicuspid, 1st bicuspid, canine and last incisors! Notice arch size is increased but minimal expansion in the cuspijd and incisor area.
Figure 4 Expansion vs IPR Treatment Outcomes
- Compares arch width changes between treatments
- Shows expansion produces significant changes while IPR doesn't affect width
Interproximal Reduction: Capabilities and Limitations
What IPR Does Well
Interproximal enamel reduction has gained significant acceptance in orthodontic practice, particularly for managing crowding in nonextraction cases. The literature on IPR safety and effectiveness is reassuring, with long-term studies by Zachrisson and others demonstrating minimal adverse effects when performed properly (4).
IPR reliably creates space for tooth alignment, typically providing 0.2-0.5 mm per treated surface. This space creation can be precisely calculated and predictably achieved, making IPR a valuable tool for treatment planning.
The Smile Width Reality
However, when it comes to smile width enhancement, IPR has significant limitations. Unlike expansion, IPR doesn't increase arch dimensions or reduce buccal corridors. While IPR can improve tooth alignment and create better smile harmony, it won't address complaints about narrow smiles or excessive buccal corridor display.
This distinction proves crucial in treatment planning. Patients seeking wider smiles won't achieve their goals through IPR alone, regardless of how expertly it's performed. Understanding this limitation helps set appropriate expectations and guides treatment selection.
Safety and Technique
The safety profile of IPR, when performed according to established protocols, appears excellent. The work by Zachrisson's group, following patients for more than 10 years after IPR, found no increase in caries incidence or periodontal problems (4). Proper technique, including adequate cooling during reduction and appropriate finishing procedures, appears critical for these positive outcomes.
Treatment Selection: Making Informed Decisions
Matching Treatment to Goals
The decision between expansion and IPR for cases involving smile width concerns ultimately depends on treatment objectives. For patients specifically seeking broader smiles and presenting with genuine transverse deficiencies, expansion offers the only direct solution. IPR, while valuable for many aspects of orthodontic treatment, doesn't address smile width concerns.
However, this doesn't mean expansion is always appropriate. Patient age, skeletal maturity, periodontal status, and willingness to maintain permanent retention all factor into treatment decisions. Some patients may benefit from combination approaches, using expansion to address width deficits while employing IPR for fine-tuning alignment.
Setting Realistic Expectations
Perhaps most importantly, clinicians must set realistic expectations about outcomes and maintenance requirements. Expansion can enhance smile width, but it requires lifelong retention in most cases. IPR can improve smile harmony and alignment but won't create broader smiles.
Patients often have unrealistic expectations about what orthodontic treatment can achieve, particularly regarding smile width changes. Clear communication about capabilities and limitations of different approaches helps ensure treatment satisfaction.
Current Research Trends and Future Directions
Digital Integration
Contemporary orthodontic research increasingly incorporates digital smile design and 3D analysis methods. These technologies offer potential advantages in treatment planning and outcome prediction, though their impact on long-term treatment success remains to be determined.
The integration of facial scanning, digital treatment planning, and virtual reality patient consultation represents an evolving area that may enhance our ability to predict and achieve desired smile width outcomes.
Outcome Measurement
Recent studies place greater emphasis on patient-reported outcomes and validated satisfaction measures. This trend toward patient-centered outcome assessment provides valuable insights into treatment effectiveness from the patient perspective, complementing traditional clinical measurements (6).
Long-term Studies
Perhaps most needed are extended follow-up studies that track smile width changes and patient satisfaction over decades rather than years. The current literature, while informative, often lacks the extended follow-up necessary to fully understand long-term stability and patient satisfaction with different treatment approaches.
Clinical Recommendations
Based on the available evidence, several clinical recommendations emerge:
For Patients Seeking Smile Width Enhancement:
- Evaluate for genuine transverse deficiency before recommending expansion
- Consider patient age and skeletal maturity in treatment planning
- Ensure patients understand retention requirements for expansion cases
- Set realistic expectations about achievable changes
For Treatment Planning:
- Use standardized photography protocols for smile assessment
- Consider cultural background in aesthetic evaluation
- Plan for permanent retention in expansion cases
- Recognize IPR limitations for smile width goals
For Long-term Success:
- Emphasize retention compliance in expansion cases
- Monitor for relapse in extended follow-up
- Consider retreatment protocols for significant relapse
- Maintain realistic expectations about aging changes
Limitations and Research Gaps
This review has several limitations. The heterogeneity of study designs and outcome measures limits direct comparisons between treatments. Many studies lack extended follow-up periods, and few randomized controlled trials compare different treatment approaches directly.
Significant research gaps remain, including limited data on cultural preferences, insufficient long-term stability information, and minimal economic analysis of different treatment approaches. Future research should address these gaps through well-designed, long-term comparative studies.
Conclusions
The evidence on smile width and orthodontic treatment provides useful guidance for clinical practice, though significant questions remain unanswered. Broader smiles generally receive higher attractiveness ratings (1,2), and expansion can effectively reduce buccal corridors when properly applied and maintained.
However, expansion's stability challenges require careful consideration and lifelong retention commitment. IPR offers reliable space creation with excellent long-term safety but doesn't address smile width concerns directly.
Treatment selection should be based on careful assessment of patient goals, anatomical considerations, and maintenance capabilities. Setting realistic expectations and ensuring appropriate retention protocols remain crucial for successful outcomes.
As our understanding of smile aesthetics continues to evolve, practitioners must balance evidence-based treatment approaches with individual patient needs and preferences. The goal isn't to achieve perfect smiles according to research-based standards, but to help patients achieve their aesthetic goals within the bounds of biological and technical possibilities.
The future likely holds continued refinement of treatment approaches, better prediction of outcomes, and improved understanding of long-term stability. Until then, thoughtful application of current evidence, combined with honest communication about capabilities and limitations, serves our patients best.
References
1. Sarver DM. The importance of incisor positioning in the esthetic smile: the smile arc. Am J Orthod Dentofacial Orthop. 2001;120(2):98-111.
2. Moore T, Southard KA, Casko JS, Qian F, Southard TE. Buccal corridors and smile esthetics. Am J Orthod Dentofacial Orthop. 2005;127(2):208-213.
3. Parekh SM, Fields HW, Beck M, Rosenstiel S. Attractiveness of variations in the smile arc and buccal corridor space as judged by orthodontists and laymen. Angle Orthod. 2006;76(4):557-563.
4. Zachrisson BU, Nyøygaard L, Mobarak K. Dental health assessed more than 10 years after interproximal enamel reduction of mandibular anterior teeth. Am J Orthod Dentofacial Orthop. 2007;131(2):162-169.
5. Ioi H, Kang S, Shimomura T, Kim SS, Park SB, Son WS, Takahashi I. Effects of buccal corridors on smile esthetics in Japanese and Korean orthodontists and orthodontic patients. Am J Orthod Dentofacial Orthop. 2012;142(4):459-465.
6. Coppola G, Christopoulou I, Gkantidis N, Verna C, Pandis N, Kanavakis G. The effect of orthodontic treatment on smile attractiveness: a systematic review. Prog Orthod. 2023;24(1):4..
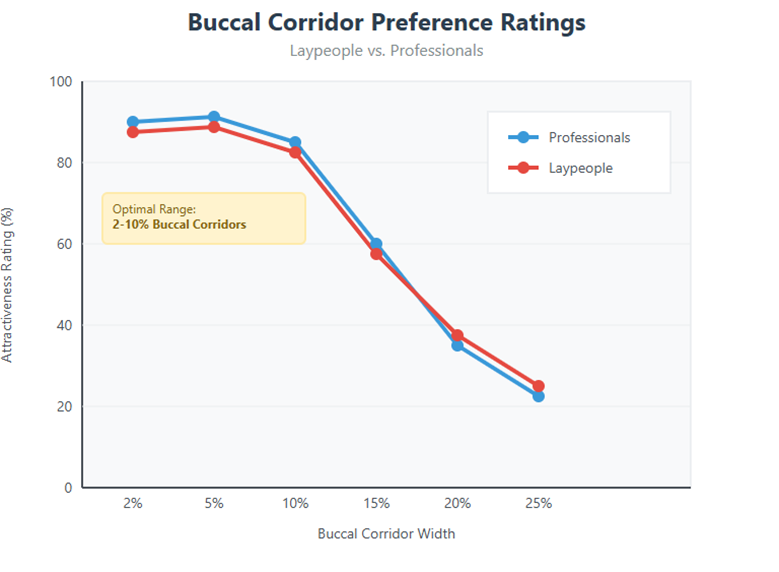
Figure 1
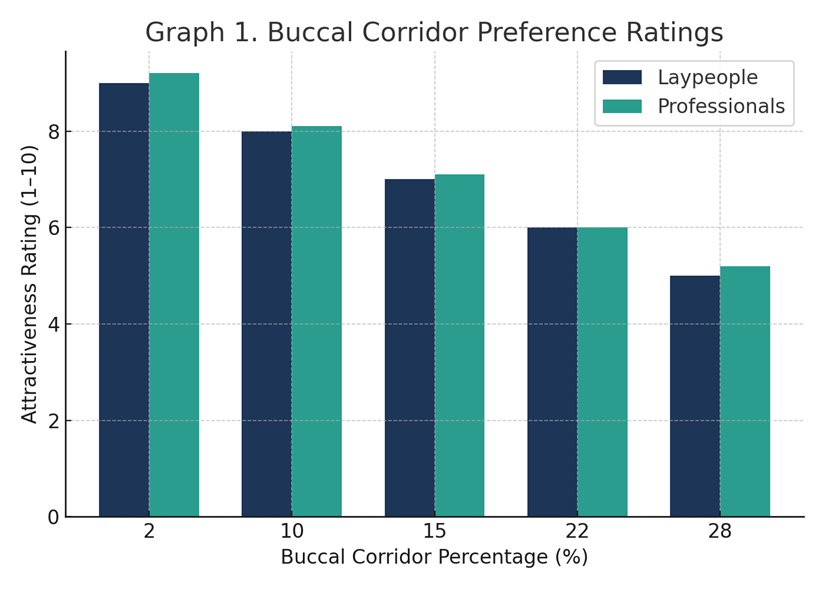
Figure 2
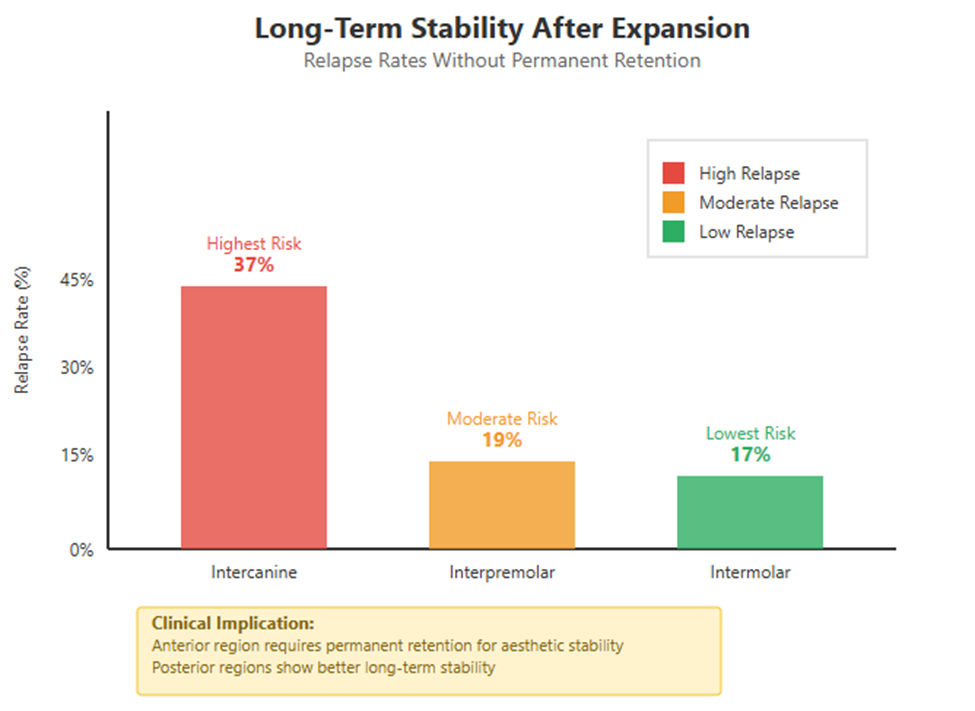
Figure 3
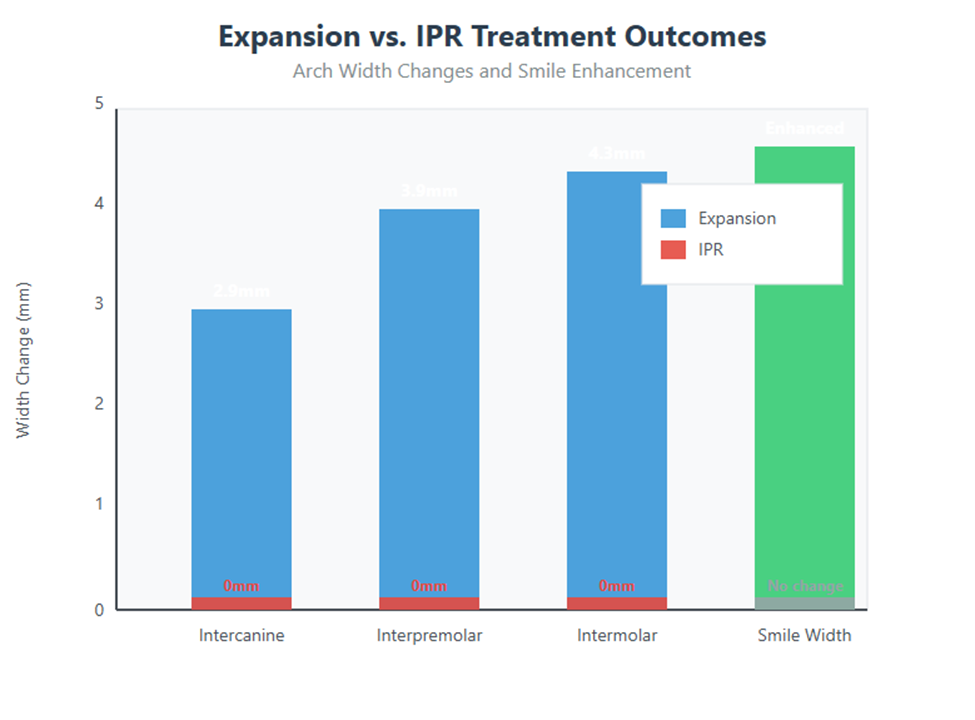
Figure 4
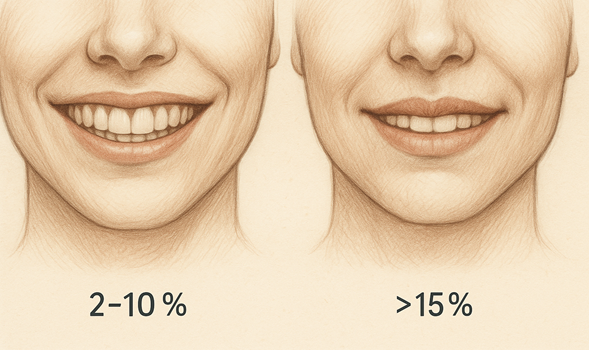
Figure 5
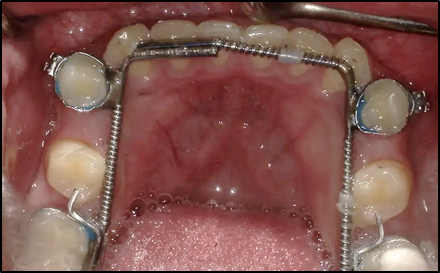
Figure 6