A Case of Type A Acute Aortic Dissection with a Normal D-dimer
A Case of Type A Acute Aortic Dissection with a Normal D-dimer
Le Grice K1, Patel R2, Tregidgo L3, Kavidasan A4*
1. Department of Chest Medicine and Interventional Pulmonology, Croydon University Hospital, UK.
Correspondence to: Dr Aji Kavidasan, Department of Chest Medicine and Interventional Pulmonology, Croydon University Hospital, UK.
Copyright
© 2025 Dr Aji Kavidasan. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 18 Sep 2025
Published: 01 Oct 2025
A Case of Type A Acute Aortic Dissection with a Normal D-dimer
Introduction
Acute aortic dissection is an uncommon, but potentially fatal condition, in which early recognition is vital to reduce mortality.
Acute aortic dissection has an incidence of around 7-10 per 100,000 in the UK (1), and type A dissections, which involve the ascending thoracic aorta, have a mortality of around 50% in the first 24 hours if untreated (2). Treatment requires emergency surgical intervention, which can reduce one month mortality from 90 to 30% (3), however 50% of patients die prior to receiving surgery (4). Although the main symptom of acute aortic dissection is typically described as sudden onset tearing chest pain, it is well documented that patients often present with non-specific or atypical features (5-7), and its recognition can therefore be challenging. A number of surrogate markers have been suggested as an aid towards diagnosis, and multiple studies and meta-analysis have shown a positive d-dimer as a highly specific positive predictor for aortic dissection (8-11). However here we present a case of type A aortic dissection with a normal d-dimer.
Case Report
A 54 year old electrician was brought to A&E following sudden onset chest pain at rest associated with a total loss of consciousness. He described feeling sweaty and dizzy and was then seen to lose consciousness for around 70 seconds. On regaining consciousness he described a severe, central, non-radiating chest pain, associated with breathlessness and sweats.
He was otherwise fit and well, his only past medical history a hip replacement secondary to a previous fall, and he had no regular medications. Both his parents had Ischaemic heart disease in their early 40s. He drank minimal alcohol and was a never smoker.
ECG in the ambulance showed T wave inversion in leads V4-6, and he was treated with GTN and aspirin prior to arrival at the hospital.
On arrival in A&E he had ongoing chest pain, albeit improving. On assessment he was alert, with normal observations including blood pressure of 143/85. Examination was unremarkable, however radio-radial delay nor blood pressure in both arms were documented at the time of initial assessment. Repeat ECG showed non-dynamic changes, and blood tests were unremarkable, other than a mildly raised troponin of 21. D-dimer was normal at 139. Chest x-ray was documented as unremarkable.
He was diagnosed with an NSTEMI and admitted under the medical team, with a plan for ACS treatment, serial ECGS and a repeat troponin.
The patient had ongoing chest pain overnight, not relieved by GTN. On assessment by the medical consultant the next morning, he had ongoing chest pain and was sweaty and clammy, and on examination he looked unwell. There was no radio-radial or radio-femoral delay, but blood pressure was elevated at 188/98. Blood pressure in both arms was not documented but was requested. Repeat troponins were static and there were no dynamic ECG changes. An urgent cardiology review and CT aortogram were requested.
Fig 1
CT aortogram showed Stanford A thoraco-abdominal dissection with pre-existing abnormal ascending aorta. Unfortunately, shortly after returning from CT the patient deteriorated and suffered a cardiac arrest. Despite a prolonged resuscitation including an attempted pericardiocentesis, the patient did not survive.
Discussion
This case, the patient was treated for a suspected ACS but sadly died the day following admission from a type A thoraco-abdominal aortic dissection. He was treated for ACS based on chest pain with total loss of conscious, on a background of a family history of MI, with non-dynamic ECG changes, static troponins and normal d-dimer. He was not initially hypertensive, did not have radio-radial or radio-femoral delay and had a normal chest x-ray, but he did have ongoing chest pain despite GTN.
It is well documented that aortic dissection can present with non-specific findings, but most cases of aortic dissection reported are shown to have a raised d-dimer. The ADvISED study (12) looked at >1800 patients with aortic dissection and only 8 of these were shown to have a negative d-dimer. When combined with risk stratification tool this dropped to only 4 patients. The patient in our case would have fallen into this group, despite the significant extent of his dissection. It is therefore important to recognise that even severe thoraco-abdominal cases can have normal biochemical markers, and aortic dissection should be considered in cases of chest pain with loss of consciousness, atypical chest pain or where pain is out of keeping with other clinical findings, even when other parameters are within the normal range.
References
1. Booth K; Acute aortic dissection (AAD) – a lethal disease: the epidemiology, pathophysiology and natural history; Br J Cardiol. 2023; 30(1): 9
2. Akin I, Nienaber CA; Prediction of aortic dissection; Heart; 2020; 106 892-897
3. Ranasinghe AM, Strong D, Boland A, Bonser RS; Acute aortic dissection; BMJ; 2011; 343:4487
4. Thrumurthy SG, Karthikesalingam A, Patterson BO, Holt PJE, Thompson MM; The diagnosis and management of aortic dissection; BMJ; 2012; 344: 8290
5. Erbel R, Aboyans V, Boileau C et al; 2014 ESC Guidelines on the diagnosis and treatment of aortic diseases: Document covering acute and chronic aortic diseases of the thoracic and abdominal aorta of the adult. The Task Force for the Diagnosis and Treatment of Aortic Diseases of the European Society of Cardiology (ESC); Eur. Heart J; 2014, 35, 2873–2926
6. Hansen MS, Nogareda GJ, Hutchison SJ; Frequency of and inappropriate treatment of misdiagnosis of acute aortic dissection; Am J Cardiol; 2007; 99(6):852-6
7. Ayrik C, Cece H. Aslan O, Karcioglu O, Yilmaz E; e24Seeing the invisible: painless aortic dissection in the emergency setting; Emerg Med J; 2006; 23(3): e34
8. Cui J-S, Jing ZP, Zhuang S-J et al; D-dimer as a Biomarker for Acute Aortic Dissection : A Systematic Review and Meta-analysis; Medicine (Baltimore); 2015; 94(4): e471
9. Yao J, Bai T, Yang B, Sun L; The diagnostic value of D-dimer in acute aortic dissection: a meta-analysis; Journal of Cardiothoracic Surgery; 2021; 16: 343
10. Bima P, Pivetta E, Nazerian P et al; Systematic Review of Aortic Dissection Detection Risk Score Plus D-dimer for Diagnostic Rule-out Of Suspected Acute Aortic Syndromes; Acad Emerg Med; 2020; 27(10):1013-1027Published: 27 May 2016
11. Watanabe H, Horita N, Shibata Y et al; Diagnostic test accuracy of D-dimer for acute aortic syndrome: systematic review and meta-analysis of 22 studies with 5000 subjects; Scientific Reports; 2016; 6: 26893
12. Nazerian P, Mueller C, de Matos Soeiro A et al; Diagnostic Accuracy of the Aortic Dissection Detection Risk Score Plus D-Dimer for Acute Aortic Syndromes: The ADvISED Prospective Multicenter Study; Circulation; 2018; 137(3):250-258.
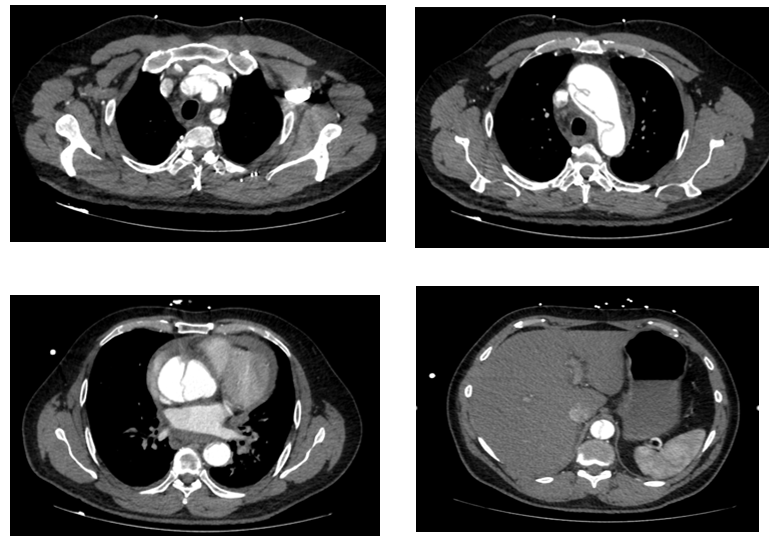
Figure 1