Esophageal Duplication Cyst Presenting as Severe Abdominal Pain.
Esophageal Duplication Cyst Presenting as Severe Abdominal Pain.
Manjakkollai P. Veerabagu, MD1*, Leila Kutob, MD2, Adam Beall, MD3, and Paul Frassinelli, MD4
1. AnMed, Anderson, South Carolina, Affiliate Associate Professor of Medical University of South Carolina, Division of Gastroenterology, Charleston, SC.
2. AnMed, Anderson, South Carolina, Department of Pathology.
3. Department of Surgery, AnMed, Anderson, South Carolina.
4. AnMed, Anderson, SC Assistant Professor of Medical University of South Carolina, Department of Surgery, Charleston, SC
*Correspondence to: Manjakkollai P. Veerabagu, AnMed, Anderson, South Carolina, Affiliate Associate Professor of Medical University of South Carolina, Division of Gastroenterology, Charleston, SC.
Copyright
© 2025 Manjakkollai P. Veerabagu, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 30 Sep 2025
Published: 08 Oct 2025
Esophageal Duplication Cyst Presenting as Severe Abdominal Pain.
Introduction
Esophageal duplication cysts are rare congenital malformations involving the foregut during early weeks of embryonic development. Most of the duplication cysts are asymptomatic. Occasionally they present with symptoms later in life. Dysphagia, food impaction, cough and chest pain are some of the clinical presentations. We present a rare case of esophageal duplication cyst presenting with severe abdominal pain.
A 28-year-old healthy gentleman with no prior medical history presented to the emergency room with sudden onset of severe right upper quadrant and epigastric abdominal pain associated with nausea and vomiting. Liver enzymes and lipase were normal. CBC showed mild leukocytosis (12.24 K/microL). Cross-sectional imaging revealed a well-circumscribed soft density lesion adjacent to the gastroesophageal junction (Fig. 1). Ultrasound evaluation did not show any cholecystitis or gall stones. Esophagogastrostomy did not show significant changes in the esophagus or in the gastroesophageal junction or in the stomach. Endoscopic ultrasound evaluation showed a well encapsulated lesion measuring 3 cm not arising from the muscularis propria of the esophagus but close to the GE junction with both liquid and solid contents (Fig. 2). Needle aspiration showed mucinous material suggesting possible esophageal duplication cyst. Laparoscopy was performed ,revealing a pedunculated cystic lesion at the gastroesophageal junction (Fig. 3). It was stapled at its origin, with a bougie in the esophagus to minimize the risk of narrowing the esophageal lumen (Fig. 3). Histopathological examination confirmed it was indeed an esophageal duplication cyst (Fig. 4,5 &6). The inner lining of the cyst was ciliated columnar epithelium (Fig. 4). Interestingly double layer of smooth muscle was noted (Fig. 6). Following surgical removal, the pain completely resolved and on follow up the patient was feeling completely normal.
Figure 1. CT scan showing the lesion adjacent to the GE junction
Figure 2. Endoscopic Ultrasound evaluation showing solid cystic lesion near GE junction
Figure 3. Laparoscopic removal of the esophageal duplication cyst
Figure 4. High power view (40 x) of an H&E stained section of the cyst lining demonstrating the ciliated columnar epithelium
Fig. 5. Low Power view (4x) of an H&E stained section of showing cystic structure with a well-developed smooth muscle layer forming the wall and lined by ciliated columnar epithelium. No cartilage identified.
Fig. 6. Another low power view (4x) of an H&E stained section of the esophageal duplication cyst demonstrating well-developed double smooth muscle layer.
Esophageal duplication cysts are typically asymptomatic, but they can cause symptoms later in life, despite being congenital abnormalities. The incidence of esophageal duplication is 1 in 8200 (1). They are thought to form between 4th and 8th week of development as a result of failure of intrauterine vacuolization of the esophagus (2). They constitute 0.5% to 2.5% of all esophageal masses (2,3). They are more common in males, with a male to female ratio of 2:1. They are often discovered incidentally on upper endoscopy evaluation seen as a submucosal bulge. Duplication cyst should be distinguished from leiomyoma, lipoma and gastrointestinal stromal tumors (4). If they are symptomatic, the usual symptoms are dysphagia, chest pain and cough. Our patient presented with severe upper abdominal pain. The lesion was pedunculated and we postulated that torsion or bleeding could have caused the patient’s symptoms. Symptomatic esophageal duplication cysts are removed mostly by surgery. Some esophageal duplication cysts could be treated by endoscopic fenestration using endoscopic ultrasound but in our patient that was not possible due to its peduncular morphology and location near the GE junction (5).
References
1. Anderson MC, Silverman WW, Shields TW. Duplications of the alimentary tract in the adult Arch Surg 1962;85: 94-108.
2. Arbona JL, Fazzi JG, Mayoral J. Congenital esophageal cysts. Case report and review of literature. Am J Gastroenterol 1984;79: 177-82.
3. Whitakeer JA, Deffenbaugh LD, Cooke AR. Esophageal duplication cyst. Case report. Am J Gastroenterol 1980;73: 329-32
4. Bhatia V, Tajka M, Rastogi A. Upper gastrointestinal submucosal lesions-clinical and endosonographic evaluation and management. Trop Gastroenterol 2010;31: 5-29.
5. Radhika Chavan, Zaheer Nabi, Sukrit Sud et al. Advanced endoscopic techniques for esophageal duplication cyst treatment: beyond surgery. GIE 10;6:326-332.

Figure 1

Figure 2
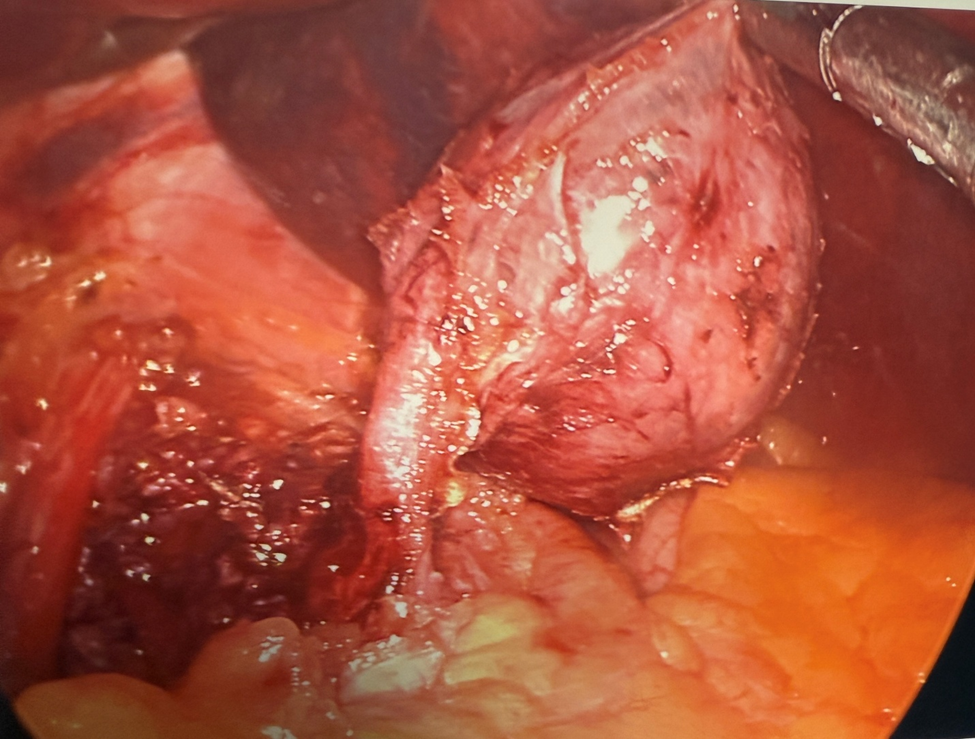
Figure 3
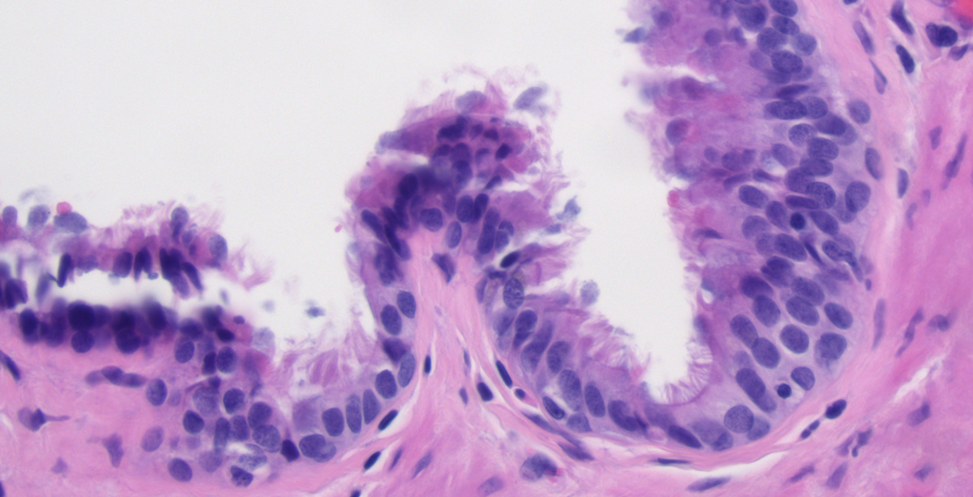
Figure 4
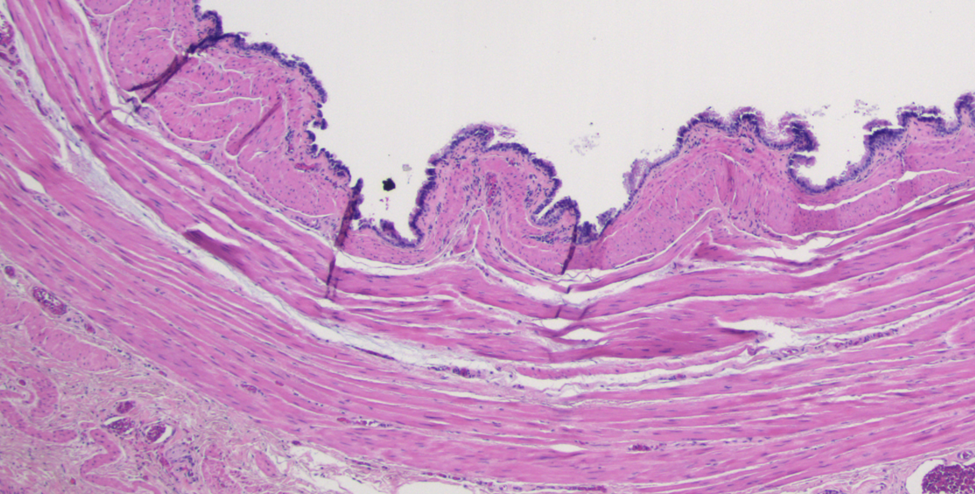
Figure 5
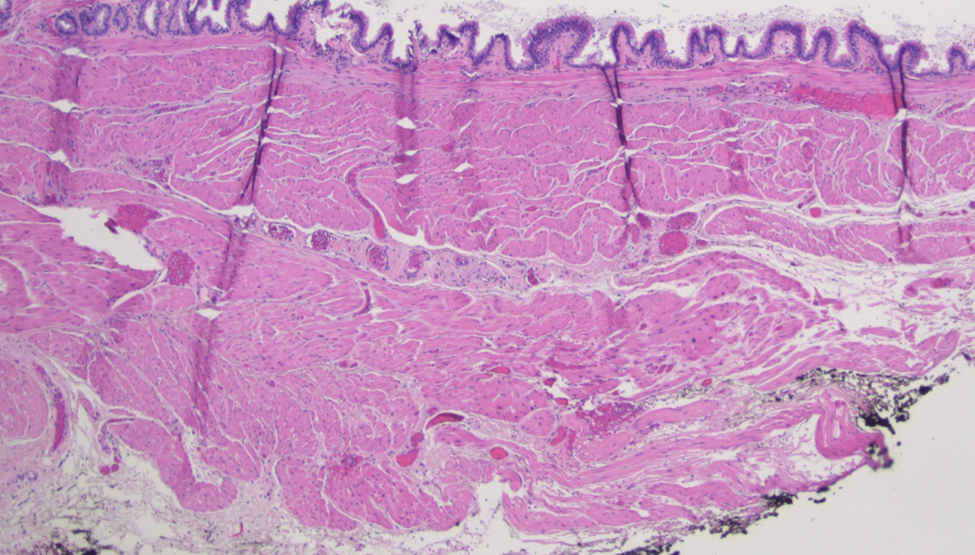
Figure 6