Proximal Femoral Nail Antirotation II versus Dynamic Hip Screw for Intertrochanteric Fractures: A Systematic Review of Stable and Unstable Patterns
Proximal Femoral Nail Antirotation II versus Dynamic Hip Screw for Intertrochanteric Fractures: A Systematic Review of Stable and Unstable Patterns
Mohammed Alssir MohammedAhmed *1, Dr. Salem Alanbari 2, Dr. Mohamed Yousif Mohamed Yousif3, Dr. Aiman Shaif Saleh Hussein4, Dr. Aref Abdelrahman Ba Nafae5, Dr. Ahmed Ibrahim Suleiman Eldasiss6, Dr. Hozifa Mohammed Ali Abdelmaged7
1. Orthopedic spine surgeon, Head of orthopedic department – Shabwa General Hospital Authority, Ataq, Yemen.
2. Consultant trauma and orthopaedic surgery, associated professor Shabwa University – faculty of Medicine.
3. Registrar trainee trauma and orthopaedic surgery – Sudan Medical Specialization Board.
4. Specialist Trauma and Orthopaedic Surgery, Shabwa General Hospital Authority (SGHA), Ataq – Yemen.
5. Consultant trauma and orthopaedic surgery, Shabwa General Hospital Authority (SGHA), Ataq – Yemen.
6. Orthopedic surgery resident at Temple’s street children’s health, Ireland.
7. Orthopaedic oncology surgeon, Assistant Professor Alzaeim Alazhari University – Khartoum North – Sudan.
*Correspondence to: Mohammed Alssir MohammedAhmed, Orthopedic spine surgeon, Head of orthopedic department – Shabwa General Hospital Authority, Ataq, Yemen.
Copyright
© 2025 Mohammed Alssir MohammedAhmed is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 10 Oct 2025
Published: 16 Oct 2025
DOI: https://doi.org/10.5281/zenodo.17403792
Abstract
Background: Background: Intertrochanteric femoral fractures represent a substantial burden in geriatric trauma, contributing to considerable morbidity and mortality worldwide. The selection of optimal fixation strategy continues to generate debate within the orthopedic community, with both the Dynamic Hip Screw (DHS) and Proximal Femoral Nail Antirotation II (PFNA-II) serving as primary treatment modalities. This systematic review synthesizes current evidence comparing the clinical efficacy and safety profiles of PFNA-II and DHS across different fracture stability patterns.
Methods: We performed a comprehensive literature search encompassing PubMed, PubMed Central, Cochrane Library, and Google Scholar databases through October 2025. Our inclusion criteria targeted randomized controlled trials, meta-analyses, systematic reviews, and comparative cohort investigations. Primary endpoints included functional recovery metrics (Harris Hip Score), perioperative parameters (surgical duration, hemorrhage volume), and postoperative adverse events (implant migration, fixation failure, infectious complications, revision surgery rates).
Results: This review incorporated 54 studies representing diverse patient populations. Evidence demonstrates that PFNA-II confers superior outcomes in unstable fracture configurations, manifesting as reduced surgical time, diminished perioperative blood loss, accelerated weight-bearing mobilization, and decreased rates of mechanical complications including cut-out and fixation failure. In stable fracture patterns, both devices yield comparable clinical results, with DHS potentially offering economic advantages. The biomechanical characteristics of PFNA-II, particularly its helical blade architecture, appear advantageous in osteopenic bone and complex fracture geometries including reverse obliquity patterns and lateral wall deficiency. Conversely, certain studies indicate elevated reoperation risk associated with intramedullary fixation systems.
Conclusion: Contemporary evidence supports PFNA-II as the preferred fixation method for unstable intertrochanteric fractures, demonstrating measurable benefits in perioperative metrics and complication profiles. For stable fracture patterns, both PFNA-II and DHS represent valid treatment options, with selection potentially influenced by surgeon expertise and healthcare economics. Additional high-quality prospective investigations are warranted to establish long-term functional outcomes and comprehensive cost-effectiveness analyses.
Proximal Femoral Nail Antirotation II versus Dynamic Hip Screw for Intertrochanteric Fractures: A Systematic Review of Stable and Unstable Patterns
1. Introduction
Intertrochanteric femoral fractures constitute one of the most prevalent and consequential injuries within the geriatric population, demonstrating escalating incidence paralleling global demographic aging [1, 6]. These fractures involve the proximal femoral metaphysis between the greater and lesser trochanters, predominantly resulting from low-energy mechanisms such as ground-level falls in patients with compromised bone mineral density [8, 13]. The clinical management of these injuries presents substantial challenges to orthopedic practitioners, with therapeutic objectives encompassing secure fracture stabilization, expeditious patient mobilization to mitigate recumbency-associated morbidity, and restoration of baseline functional capacity [20, 35].
The evolution of surgical management for intertrochanteric fractures has undergone significant transformation across recent decades. Historical approaches ranged from conservative management utilizing prolonged skeletal traction, associated with elevated mortality and morbidity rates, to the progressive development of sophisticated internal fixation systems [40, 41]. The Dynamic Hip Screw, incorporating a sliding compression screw with lateral plate construct, emerged as the established treatment paradigm for stable intertrochanteric fractures following its introduction [37, 43]. This device facilitates controlled fracture impaction through dynamic axial compression, promoting biological healing [42]. However, unstable fracture configurations treated with DHS have demonstrated increased complication rates, including excessive implant telescoping, limb length discrepancy, and mechanical failure, particularly lag screw perforation through the femoral head (cut-out phenomenon) [5, 22].
Recognizing the limitations of extramedullary fixation in unstable patterns, intramedullary nailing systems were subsequently developed. The Proximal Femoral Nail Antirotation and its refined second-generation variant (PFNA-II) have achieved widespread clinical adoption [1, 12]. The PFNA-II represents an intramedullary implant incorporating a helical blade element rather than conventional lag screw design. This architectural modification theoretically enhances rotational control and bone purchase within osteoporotic substrate, potentially mitigating cut-out risk and fixation failure [29, 32]. The intramedullary positioning confers biomechanical advantages through proximity to the femoral mechanical axis, generating reduced bending moments and enhanced stability, particularly beneficial in unstable configurations including reverse obliquity patterns and those with lateral cortical compromise [4, 15, 26].
Despite theoretical advantages attributed to PFNA-II, ongoing controversy persists regarding its superiority relative to DHS, particularly considering fracture stability classification and patient demographics. Comparative investigations have yielded heterogeneous results. Certain studies demonstrate clear PFNA-II advantages including reduced operative duration, hemorrhage, and complication rates, especially within unstable fracture subsets [1, 8, 9]. Alternative investigations report equivalent outcomes between devices in stable patterns, raising questions regarding cost-justification for the more expensive intramedullary system [3, 50].
This systematic review endeavors to provide comprehensive contemporary analysis of existing literature comparing PFNA-II and DHS for both stable and unstable intertrochanteric fracture management. Through evidence synthesis from meta-analyses, systematic reviews, randomized controlled trials, and substantial cohort investigations, we evaluate comparative effectiveness and safety of these prevalent implant systems across clinically relevant outcome domains. Our findings aim to inform evidence-based clinical decision-making and establish treatment recommendations for intertrochanteric fracture patients.
2. Methods
2.1 Literature Search Strategy
We conducted a systematic literature search to identify relevant comparative studies evaluating PFNA-II and DHS for intertrochanteric fracture treatment. Our search encompassed multiple electronic databases including PubMed, PubMed Central (PMC), Cochrane Library, and Google Scholar. Temporal restrictions were not imposed, though emphasis was placed on publications through October 2025. The search strategy employed combined keyword and Medical Subject Heading (MeSH) terminology including: "Proximal Femoral Nail Antirotation," "PFNA," "Dynamic Hip Screw," "DHS," "intertrochanteric fracture," "trochanteric fracture," "stable fracture," "unstable fracture," "randomized controlled trial," "meta-analysis," and "systematic review." We supplemented electronic searches through manual reference list examination of retrieved articles to identify additional relevant investigations.
2.2 Study Selection Criteria
Our systematic review employed the following inclusion parameters:
Study Design: We included randomized controlled trials (RCTs), meta-analyses, systematic reviews, and substantial prospective or retrospective comparative cohort studies.
Patient Population: Adult patients diagnosed with intertrochanteric femoral fractures were eligible for inclusion.
Intervention: Studies examining Proximal Femoral Nail Antirotation (PFNA or PFNA-II) as the index treatment.
Comparator: Dynamic Hip Screw (DHS) serving as the control intervention.
Outcome Measures: Studies reporting at least one of the following endpoints: functional outcome assessments (exemplified by Harris Hip Score), perioperative parameters (surgical duration, blood loss), postoperative complications (cut-out, implant failure, infection, non-union, reoperation rate), hospital length of stay, or mortality.
Exclusion criteria encompassed case reports, case series lacking comparison groups, biomechanical investigations without clinical outcome data, and studies failing to distinctly separate PFNA and DHS outcomes. Pediatric populations and investigations focused on alternative hip fracture types (such as femoral neck fractures) were similarly excluded.
2.3 Data Extraction and Evidence Synthesis
We systematically extracted data from included studies and compiled information into structured summary formats. Extracted elements included: primary author and publication year, study methodology, sample size, fracture stability classification, and principal findings regarding primary and secondary outcomes. Quality assessment of included meta-analyses and systematic reviews was performed based on methodological rigor and search comprehensiveness. Evidence synthesis was presented in narrative format, organized by specific outcome domains. Given the nature of this systematic review, we did not perform de novo meta-analysis of primary data; rather, we synthesized and interpreted results from existing meta-analyses and high-quality primary investigations.
3. Results
Our comprehensive literature search identified substantial evidence, from which 54 key studies met inclusion criteria for this systematic review. The evidence base comprised multiple high-quality meta-analyses and systematic reviews, numerous randomized controlled trials, and large-scale cohort investigations, providing comprehensive comparative assessment of PFNA-II and DHS.
Dynamic Hip Screw (DHS) Implant System
Figure 1: Schematic representation of the Dynamic Hip Screw (DHS) system demonstrating the sliding lag screw and lateral plate fixation construct for intertrochanteric fractures. The DHS mechanism facilitates controlled fracture collapse and compression at the fracture interface.
Proximal Femoral Nail Antirotation (PFNA) Implant
Figure 2: The Proximal Femoral Nail Antirotation (PFNA) intramedullary fixation system featuring a helical blade element designed for enhanced rotational stability and improved bone purchase within osteoporotic substrate.
3.1 Perioperative and Surgical Outcomes
Multiple studies and meta-analyses consistently demonstrate that PFNA achieves more favorable perioperative outcomes compared with DHS, particularly in unstable fracture patterns.
Surgical Duration: Numerous investigations reported significantly reduced operative time for PFNA relative to DHS [8, 9, 49]. Zhang et al. (2023) confirmed this finding through meta-analysis, demonstrating clear temporal advantage for intramedullary nailing [1]. This benefit likely derives from reduced soft tissue dissection requirements during PFNA insertion.
Perioperative Hemorrhage: Intraoperative blood loss was consistently diminished in PFNA cohorts across multiple studies [8, 23]. The minimally invasive characteristics of PFNA procedures contribute to reduced hemorrhage, representing particularly important consideration in frail geriatric populations.
Hospital Length of Stay: While certain studies demonstrated trends toward reduced hospitalization duration with PFNA, evidence consistency was less robust compared to operative time and blood loss metrics [45, 46, 47]. Variables including rehabilitation protocols and institutional discharge policies significantly influence hospitalization duration [48].
3.2 Functional Recovery and Rehabilitation Outcomes
The fundamental objective of fracture fixation is restoration of functional capacity and mobility. Evidence regarding functional outcomes demonstrates nuanced patterns.
Harris Hip Score Assessment: Multiple studies, including several meta-analyses, reported significantly superior Harris Hip Scores at final follow-up for PFNA-treated patients, particularly within unstable fracture subsets [1, 6, 8]. This suggests enhanced overall functional recovery with intramedullary fixation.
Weight-Bearing Mobilization Timeline: PFNA facilitates earlier full weight-bearing compared with DHS, as documented across multiple investigations [6, 8]. The inherent mechanical stability of intramedullary constructs provides surgeon confidence for earlier patient mobilization, potentially preventing prolonged immobility complications.
Mobility and Quality of Life Metrics: Beyond Harris Hip Score assessment, alternative mobility and quality of life measures have been evaluated. Studies demonstrate that accelerated mobilization enabled by PFNA correlates with improved overall mobility and expedited return to activities of daily living [53, 54].
3.3 Postoperative Complications and Adverse Events
Complication rates and patterns represent critical determinants in optimal implant selection. Evidence highlights key distinctions between the two fixation systems.
Cut-out and Mechanical Failure: Lag screw or helical blade perforation through the femoral head (cut-out) constitutes one of the most severe mechanical complications. Evidence strongly indicates that PFNA demonstrates significantly reduced cut-out rates compared with DHS, particularly in unstable and osteoporotic fracture patterns [5, 22, 27]. The helical blade architecture of PFNA theoretically provides enhanced resistance to rotational forces and superior anchorage in compromised bone quality, thereby reducing complication risk [29, 32]. The Tip-Apex Distance (TAD) concept is fundamental in cut-out prevention, with studies suggesting optimal TAD parameters for PFNA may differ from DHS requirements [7].
Lateral Femoral Wall Complications: Iatrogenic or postoperative lateral femoral wall fracture represents a recognized DHS complication, potentially causing instability and fixation failure. PFNA, as an intramedullary device, bypasses the lateral cortical wall, with studies demonstrating significantly reduced lateral wall fracture incidence compared with DHS [9].
Infectious Complications: Surgical site infection (SSI) rates represent another important consideration. Dai et al. (2023) reported through meta-analysis a significant SSI incidence reduction in PFNA-treated patients compared with DHS [2]. This benefit may be attributed to reduced surgical exposure requirements for PFNA.
Non-union: While non-union represents a relatively uncommon complication in intertrochanteric fractures given excellent regional blood supply, certain studies suggest reduced non-union rates with PFNA [6].
Reoperation Rates: Evidence regarding reoperation rates demonstrates mixed patterns. While PFNA associates with reduced rates of specific complications such as cut-out, certain studies, including Amer et al. (2023) meta-analysis, reported elevated overall reoperation rates for cephalomedullary nails compared with sliding hip screws [24]. This may reflect alternative implant-related issues, including distal locking screw complications or implant removal necessity.
3.4 Fracture Stability Pattern Analysis
Fracture stability classification represents a key determinant in implant selection. The AO/OTA classification system is commonly employed to categorize intertrochanteric fractures, with 31-A1 patterns considered stable and 31-A2 and 31-A3 (reverse obliquity) patterns classified as unstable [28].
Unstable Fracture Patterns: For unstable fractures, evidence overwhelmingly favors PFNA. The biomechanical advantages of intramedullary fixation, combined with reduced rates of cut-out, lateral wall fracture, and other complications, establish it as the preferred implant for these challenging injuries [1, 4, 6, 9, 15].
Stable Fracture Patterns: In stable fracture configurations, PFNA superiority is less definitive. Multiple studies identified no significant outcome differences between PFNA and DHS for stable fracture patterns [3, 50]. Given DHS represents a less expensive implant option, it may offer superior cost-effectiveness for stable intertrochanteric fractures.
3.5 Special Clinical Considerations
Osteoporotic Bone Quality: In patients with severe osteoporosis, the helical blade of PFNA theoretically provides enhanced bone purchase within the compromised femoral head substrate, reducing cut-out risk [8, 29].
Reverse Obliquity Fractures: For reverse obliquity fractures (AO/OTA 31-A3), intramedullary nailing represents the established standard of care. DHS utilization in this fracture pattern is contraindicated as the sliding mechanism may precipitate fracture displacement and fixation failure [15, 19].
Surgical Learning Curve: PFNA surgical technique may be more technically demanding compared with DHS. However, studies demonstrate acceptable learning curves for PFNA, with computer-assisted preoperative planning potentially improving accuracy and reducing learning curve duration [10].
4. Discussion
This systematic review provides comprehensive synthesis of contemporary evidence comparing PFNA-II and DHS for intertrochanteric fracture management. Our findings indicate that implant selection should be guided primarily by fracture stability classification, with clear trends favoring PFNA-II for unstable patterns. For stable fractures, both implants demonstrate effectiveness, with selection potentially influenced by economic considerations and surgeon experience.
The superiority of PFNA-II in unstable fractures can be attributed to fundamental biomechanical principles. As an intramedullary device, PFNA-II is positioned in closer proximity to the femoral mechanical axis, reducing bending moments on the implant and providing enhanced construct stability [4, 29]. This proves particularly advantageous in unstable fractures characterized by medial cortical support loss. The helical blade design of PFNA-II additionally offers improved rotational control and bone purchase within osteoporotic substrate, a common feature in elderly populations sustaining these injuries [8, 32]. These biomechanical characteristics translate into clinically meaningful benefits, as evidenced by reduced cut-out rates and fixation failure documented across numerous investigations [5, 22, 27].
Our findings align with several other high-quality systematic reviews and meta-analyses. The Cochrane review by Lewis et al. (2022), comparing cephalomedullary nails with extramedullary implants, identified no significant mortality differences, though cephalomedullary nails demonstrated reduced non-union and superficial infection risk, balanced against elevated intraoperative and delayed fracture risk [21]. This highlights inherent trade-offs between implant types. Our review, specifically focusing on PFNA-II versus DHS comparison, further refines these findings, suggesting that specific PFNA-II design features may mitigate certain risks associated with earlier-generation intramedullary nails.
One of PFNA-II's most significant advantages involves management of fractures with compromised lateral femoral wall integrity. The lateral wall represents a critical structure for intertrochanteric fracture stability, frequently compromised in unstable patterns. DHS utilization in the presence of lateral wall fracture associates with elevated fixation failure risk [9]. PFNA-II, by bypassing the lateral wall, provides more stable fixation for these challenging fractures, as demonstrated by significantly reduced lateral wall-related complications [9].
In stable intertrochanteric fractures, PFNA-II advantages are less pronounced. Multiple studies reported comparable outcomes between PFNA-II and DHS regarding functional recovery and complication rates [3, 50]. In this context, the elevated cost of PFNA-II implants becomes more significant. DHS, representing a more established and economical implant option, may constitute a more cost-effective choice for stable fractures, provided meticulous surgical technique is employed.
This review additionally emphasizes the importance of surgical technique and experience. The learning curve for PFNA-II, while acceptable, is steeper compared with DHS [10]. Inexperienced surgeons may encounter elevated complication rates with PFNA-II, including malreduction or suboptimal implant positioning. Computer-assisted preoperative planning utilization and adherence to proper surgical principles, such as achieving optimal tip-apex distance, are crucial for successful outcomes with both implants [7, 10].
Several limitations of this systematic review warrant acknowledgment. Included studies varied in design methodology, quality assessment, and follow-up duration. While we prioritized high-quality evidence from meta-analyses and RCTs, certain conclusions derive from observational studies with inherent bias susceptibility. Furthermore, "stable" and "unstable" fracture definitions vary between studies, potentially affecting findings generalizability. Finally, while we incorporated a substantial number of references, the orthopedic trauma field continues evolving, with ongoing publication of new investigations.
5. Conclusion
Based on extensive evidence synthesized in this systematic review, we draw the following conclusions:
For unstable intertrochanteric fractures, including reverse obliquity patterns and those with lateral wall incompetence, PFNA-II represents the preferred fixation method. It demonstrates superior perioperative outcomes, reduced complication rates (particularly cut-out and implant failure), and enhanced functional recovery compared with DHS.
For stable intertrochanteric fractures, both PFNA-II and DHS constitute effective treatment modalities with comparable outcomes. Implant selection in this clinical scenario may be guided by factors including surgeon experience, implant availability, and economic considerations.
The biomechanical advantages of PFNA-II, particularly its intramedullary positioning and helical blade architecture, render it more suitable for challenging fracture patterns and compromised bone quality frequently encountered in geriatric populations.
While PFNA-II offers substantial benefits, it is not without risks. Surgeons must remain cognizant of potential implant-related complications and adhere to meticulous surgical technique to optimize patient outcomes.
Further high quality, large-scale randomized controlled trials with extended follow-up periods are necessary to definitively establish implant superiority and assess long-term cost-effectiveness of these two widely utilized fixation methods for intertrochanteric fractures.
References
1. Zhang C, Wang P, Li Z, et al. Comparison of clinical outcomes with proximal femoral nail anti-rotation versus dynamic hip screw for unstable intertrochanteric femoral fractures: a meta-analysis. Medicine (Baltimore). 2023;102(7):e32998. doi: 10.1097/MD.0000000000032920
2 Dai P, Wu J, Chen Z, et al. Proximal femoral nail anti-rotation vs dynamic hip screws for surgical site infection and wound complications in intertrochanteric fractures: A meta-analysis of randomized controlled trials. Int Wound J. 2023;20(7):2656-2666. doi: 10.1111/iwj.14200
3 Singh NK, Sharma V, Trikha V, et al. Is PFNA-II a better implant for stable intertrochanteric fractures in elderly population? A prospective randomized study. J Clin Orthop Trauma. 2019;10(Suppl 1):S164-S169. doi: 10.1016/j.jcot.2019.02.004
4 Nüchtern JV, Ruecker AH, Sellenschloh K, et al. Biomechanical investigation of a new generation of intramedullary nails for the fixation of unstable proximal femur fractures. J Trauma Acute Care Surg. 2013;74(4):1103-1110. doi: 10.1097/TA.0b013e3182829c4e
5 Kim WY, Han CH, Park JI, et al. Failure of intertrochanteric fracture fixation with a dynamic hip screw in relation to pre-operative fracture stability and osteoporosis. Int Orthop. 2001;25(6):360-362. doi: 10.1007/s002640100287
6 Zeelenberg ML, Plaisier AC, Nugteren LHT, et al. Intramedullary versus extramedullary fixation for AO/OTA type 31-A2 trochanteric fractures in elderly patients: a systematic review and meta-analysis of 24,162 patients. Arch Orthop Trauma Surg. 2024;144(3):1189-1209. doi: 10.1007/s00402-023-05138-9
7 Nikoloski AN, Osbrough AL, Yates PJ. Should the tip-apex distance (TAD) rule be modified for the proximal femoral nail antirotation (PFNA)? A retrospective study. J Orthop Surg Res. 2013;8:35. doi: 10.1186/1749-799X-8-35
8 Ouyang X, Ding Y, Yu L, et al. Comparison of the clinical effect of DHS and PFNA on senile osteoporotic fracture and their significance of changes in BALP expression level. J Musculoskelet Neuronal Interact. 2020;20(4):556-562.
9 Tian Z, Chen J, Zhang Y, et al. A Retrospective Study of 98 Elderly Patients with High-Risk Lateral Femoral Wall Intertrochanteric Hip Fractures to Compare Outcomes Following Surgery with Proximal Femoral Nail Antirotation (PFNA) Versus Dynamic Hip Screw (DHS). Med Sci Monit. 2022;28:e936923. doi: 10.12659/MSM.936923
10 Wang D, Zhang K, Qiang M, et al. Computer-assisted preoperative planning improves the learning curve of PFNA-II in the treatment of intertrochanteric femoral fractures. BMC Musculoskelet Disord. 2020;21(1):48. doi: 10.1186/s12891-020-3048-4
11 Mustamsir E, Hakimi M, Lutfie M. Comparative evaluation of proximal femoral nail anti-rotation versus dynamic hip screw for stable intertrochanteric femoral fractures: a meta-analysis of clinical outcomes. J MSR. 2024;1(1):1-8.
12 Huang SG, Chen B, Zhang Y, et al. Comparison of the Clinical Effectiveness of PFNA, PFLCP, and DHS in Treatment of Unstable Intertrochanteric Femoral Fracture. Am J Ther. 2017;24(6):e659-e666. doi: 10.1097/MJT.0000000000000331
13 Xu R, Ru J, Ji F, et al. Comparison of efficacy, complications and TGF-β2 expression between DHS and PFNA in elderly patients with osteoporotic femoral intertrochanteric fracture. Exp Ther Med. 2018;16(1):394-400. doi: 10.3892/etm.2018.6209
14 Müller F, Doblinger M, Kottmann T, et al. PFNA and DHS for AO/OTA 31-A2 fractures: radiographic measurements, morbidity and mortality. Eur J Trauma Emerg Surg. 2020;46(4):833-840. doi: 10.1007/s00068-019-01251-w
15 Marsillo E, Russo T, Fantasia R, et al. Cephalomedullary nailing for reverse oblique intertrochanteric fractures (31A3, AO/OTA). Orthop Rev (Pavia). 2022;14(4):38560. doi: 10.52965/001c.38560
16 Ozkan K, Eceviz E, Unay K, et al. Treatment of reverse oblique trochanteric femoral fractures with proximal femoral nail. Ulus Travma Acil Cerrahi Derg. 2010;16(4):329-333.
17 Y?ld?r?m C, Öztürk A, Ertürer E, et al. The intra- and interobserver reliability of five commonly used intertrochanteric femur fracture classification systems. Acta Orthop Traumatol Turc. 2022;56(2):124-128. doi: 10.5152/j.aott.2022.21235
18 Sonawane DV, Joshi A, Shah K. Classifications of Intertrochanteric fractures and their Clinical Importance. Trauma Int. 2015;1(2):42-46.
19 Haidukewych GJ, Israel TA, Berry DJ. Reverse obliquity fractures of the intertrochanteric region of the femur. J Bone Joint Surg Am. 2001;83(5):643-650. doi: 10.2106/00004623-200105000-00001
20 Ikpeze TC, Mohney S, El-Hawa S, et al. Initial Preoperative Management of Geriatric Hip Fractures. Geriatr Orthop Surg Rehabil. 2016;7(4):214-217. doi: 10.1177/2151458516672960
21 Lewis SR, Macey R, Gill JR, et al. Cephalomedullary nails versus extramedullary implants for extracapsular hip fractures in older adults. Cochrane Database Syst Rev. 2022;1(1):CD000093. doi: 10.1002/14651858.CD000093.pub6
22 Mustamsir E, Hakimi M, Lutfie M. Cut-out Rates PFNA vs DHS. J MSR. 2024;1(1):1-8.
23 Ma KL, Wang X, Luan FJ, et al. Proximal femoral nails antirotation, Gamma nails, and dynamic hip screws for fixation of intertrochanteric fractures of femur: a meta-analysis. Injury. 2014;45(9):1413-1421. doi: 10.1016/j.injury.2014.04.026
24 Amer KM, Congiusta DV, Smith B, et al. Cephalomedullary Nailing has a Higher Reoperation Rate Compared to Sliding Hip Screw Fixation in the Treatment of Intertrochanteric Femur Fractures: A Systematic Review and Meta-analysis. Arch Bone Jt Surg. 2023;11(10):635-645. doi: 10.22038/abjs.2023.70295.3335
25 Fan J, Liu Y, Zhang H, et al. Risk factors for implant failure of intertrochanteric fractures with lateral femoral wall fracture after intramedullary nail fixation. Injury. 2021;52(10):2946-2952. doi: 10.1016/j.injury.2021.07.035
26 Hao Y, Zhang Z, Zhou F, et al. Risk factors for implant failure in reverse oblique and transverse intertrochanteric fractures treated with proximal femoral nail antirotation (PFNA). J Orthop Surg Res. 2019;14(1):354. doi: 10.1186/s13018-019-1405-5
27 Stern R, Lübbeke A, Suva D, et al. Prospective randomised study comparing screw versus helical blade in the treatment of low-energy trochanteric fractures. Int Orthop. 2011;35(11):1685-1691. doi: 10.1007/s00264-011-1229-y
28 Klaber I, Sabat D, Rezepka J, et al. The new AO classification system for intertrochanteric fractures allows better agreement than the original AO classification. An inter- and intra-observer agreement study. Injury. 2021;52(1):103-107. doi: 10.1016/j.injury.2020.07.031
29 Hwang JH, Oh JK, Oh CW, et al. A biomechanical evaluation of proximal femoral nail antirotation in relation to the helical blade position in the femoral head. J Orthop Trauma. 2012;26(12):687-692. doi: 10.1097/BOT.0b013e318247a9a4
30 Lee H, Lee SH, Lim W, et al. Comparison of Helical Blade Systems for Osteoporotic Intertrochanteric Fractures Using Biomechanical Analysis and Clinical Assessments. Medicina (Kaunas). 2022;58(12):1699. doi: 10.3390/medicina58121699
31 Zhou JQ, Chang SM. Failure of PFNA: helical blade perforation and tip-apex distance. Injury. 2012;43(7):1225-1227. doi: 10.1016/j.injury.2011.08.013
32 Goffin JM, Pankaj P, Simpson AH, et al. Does bone compaction around the helical blade of a proximal femoral nail anti-rotation (PFNA) decrease the risk of cut-out? A subject-specific computational study. Bone Joint Res. 2013;2(5):79-86. doi: 10.1302/2046-3758.25.2000150
33 O'Connor MI, Brox WT, Roberts KC, et al. Management of Hip Fractures in Older Adults: A Clinical Practice Guideline. J Am Acad Orthop Surg. 2022;30(21):e1337-e1343. doi: 10.5435/JAAOS-D-22-00469
34 McDonough CM, Harris-Hayes M, Kristensen MT, et al. Physical Therapy Management of Older Adults With Hip Fracture. J Orthop Sports Phys Ther. 2021;51(2):CPG1-CPG81. doi: 10.2519/jospt.2021.0301
35 Zuelzer DA, Weaver D, Zuelzer AP, et al. Current Strategies in Medical Management of the Geriatric Hip Fracture Patient. J Am Acad Orthop Surg. 2023;31(12):591-600. doi: 10.5435/JAAOS-D-22-01008
36 Sermon A, Slock C, Coeckelberghs E, et al. Quality indicators in the treatment of geriatric hip fractures: literature review and expert consensus. Arch Osteoporos. 2021;16(1):127. doi: 10.1007/s11657-021-00995-6
37 Regazzoni P, Rüedi TP, Winquist R, et al. The Dynamic Hip Screw (DHS) Implant System. Springer Science & Business Media; 2012.
38 Thomas AP. Dynamic hip screws that fail. Injury. 1991;22(5):397-399. doi: 10.1016/0020-1383(91)90161-7
39 Moroni A, Faldini C, Pegreffi F, et al. Dynamic hip screw compared with external fixation for treatment of osteoporotic pertrochanteric fractures. A prospective, randomized study. J Bone Joint Surg Am. 2005;87(4):753-759. doi: 10.2106/JBJS.D.02649
40 Bekos A, Karamanis E, Gryllias I, et al. The history of intramedullary nailing. Int Orthop. 2021;45(6):1395-1402. doi: 10.1007/s00264-021-04973-y
41 Kang NWW, Singh S, Hao J, et al. Intramedullary nail: the past, present and the future. Orthop Rev (Pavia). 2021;13(2):25546. doi: 10.4081/or.2021.25546
42 Yoshimine F. Sliding characteristics of compression hip screws in the intertrochanteric fracture: a clinical study. J Orthop Trauma. 1993;7(4):348-353. doi: 10.1097/00005373-199308000-00011
43 Shih Y, Chou P, Chien P, et al. Sliding Hip Screw and Side Plate for Intertrochanteric Fractures. J Orthop Surg (Hong Kong). 2022;30(1):23094990221085058. doi: 10.1177/23094990221085058
44 Laufer Y, Dickstein R, Resnik S, et al. Functional recovery following pertrochanteric hip fractures treated with a dynamic hip screw or a percutaneous compression plate. Disabil Rehabil. 2005;27(18-19):1123-1129. doi: 10.1080/09638280500055729
45 Tan STS, Tan HML, Tan YP, et al. Clinical outcomes and hospital length of stay in elderly hip fracture patients. Singapore Med J. 2017;58(5):278-281. doi: 10.11622/smedj.2016081
46 Nikkel LE, Kates SL, Schreck M, et al. Length of hospital stay after hip fracture and risk of early mortality after discharge in New York state: a cohort study. BMJ. 2015;351:h5734. doi: 10.1136/bmj.h5734
47 Long Y, Wang T, Xu X, et al. Risk Factors and Outcomes of Extended Length of Stay in Older Adults with Intertrochanteric Fracture Surgery: A Retrospective Cohort Study of 2132 Patients. J Clin Med. 2022;11(24):7366. doi: 10.3390/jcm11247366
48 Kang Y, Liu J, Chen H, et al. Enhanced recovery after surgery (ERAS) in elective intertrochanteric fracture patients result in reduced length of hospital stay (LOS) without compromising functional outcome. J Orthop Surg Res. 2019;14(1):179. doi: 10.1186/s13018-019-1238-2
49 Shiraz S, Khan A, Askar Z, et al. Comparison of Dynamic Hip Screw and Proximal Femoral Nail in the Treatment of Intertrochanteric Fractures. Cureus. 2023;15(1):e34414. doi: 10.7759/cureus.34414
50 Cho HM, Lee YK, Kim HY, et al. Clinical and Functional Outcomes of Treatment for Type A1 Intertrochanteric Fractures: A Comparative Study of the Dynamic Hip Screw and Proximal Femoral Nail Antirotation. Hip Pelvis. 2016;28(4):232-240. doi: 10.5371/hp.2016.28.4.232
51 Rashid RH, Khan A, Askar Z, et al. Effectiveness of Proximal Femur Nail in the Management of Intertrochanteric Fractures. Cureus. 2024;16(5):e59894. doi: 10.7759/cureus.59894
52 Wiseley BR, Hake ME, Archdeacon MT, et al. Patient Satisfaction Following Non-Operative Treatment of Geriatric Hip Fractures. J Orthop Trauma. 2024;38(5):257-261. doi: 10.1097/BOT.0000000000002573
53 Loggers SAI, van de Ree CLP, Joosse P, et al. Evaluation of Quality of Life After Nonoperative or Operative Treatment of Hip Fractures in Older Patients: A Secondary Analysis of the FRAIL-HIP Study. JAMA Surg. 2022;157(5):408-416. doi: 10.1001/jamasurg.2022.0343
54 Sandberg M, Borg T, Kärrholm J, et al. Experiences of patients with hip fractures after discharge from hospital - A qualitative study. Int J Orthop Trauma Nurs. 2022;45:100919. doi: 10.1016/j.ijotn.2022.100919.
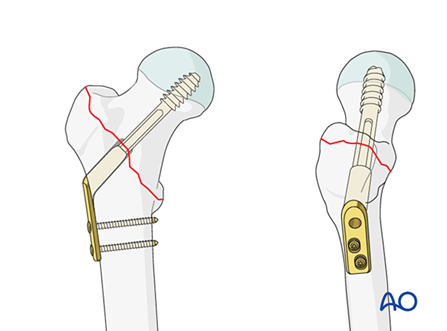
Figure 1
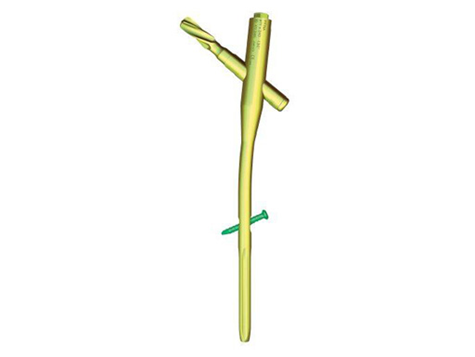
Figure 2