Cluster Headache Associated with Oculomotor Nerve Paresis: A Case Report and Review of Article
Ibrahim Krenawi*1, Shady Samy Georgy2
- Consultant Physician, Burjeel Royal Hospital, Al Ain, UAE.
- Specialist Neurologist, Burjeel Royal Hospital, Al Ain, UAE.
*Correspondence to: Ibrahim Krenawi, Consultant Physician, Burjeel Royal Hospital, Al Ain, UAE.
Copyright
© 2025 Ibrahim Krenawi, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 14 October 2025
Published: 01 November 2025
Abstract
Cluster headaches are known for their various ocular features, yet involvement of the extraocular muscles is rare. We present a case involving a 65-year-old man who experienced acute cluster headache accompanied by uniocular diplopia due to oculomotor nerve palsy. This condition responded well to oral steroids. Given the rarity of this presentation, it should be included in the differential diagnosis by both ophthalmologists and neurologists. A brief course of oral prednisolone can be beneficial in managing such cases.
Keywords: Cluster headache, treatment of cluster headache, extraocular muscles, oral prednisolone, third nerve palsy, trigeminal cephalalgias, unilateral headache, differential diagnosis of unilateral headaches.
Cluster Headache Associated with Oculomotor Nerve Paresis: A Case Report and Review of Article
Case Presentation
The patient is a 65-year-old male, non-smoker with a medical history of diabetes mellitus, arterial hypertension, and moderate depression. He is currently on oral anti-diabetic medication, insulin, a beta-blocker, and SSRIs. He presented with an acute, severe headache on the left side, described as sharp and stabbing, located around and behind the left eye and frontotemporal region. This was accompanied by vomiting, dizziness, loss of appetite, and autonomic symptoms, including an ipsilateral red, watery eye and a drooping eyelid on the affected side. He experienced between 3 to 8 attacks daily, each lasting from 15 minutes to 3 hours. He denies having an aura, any history of chronic headaches, or previous history of diplopia.
Initially, he took various medications including Paracetamol, Ibuprofen, Anapam, and Rimegepant, but these medications did not alleviate his symptoms. A concurrent treatment with Verapamil, with a gradual dose increase, was also ineffective. The pain initially responded well to oral sumatriptan, but this effect diminished over the following days. Subsequently, he developed uniocular diplopia, prompting his admission to the emergency room, where he received 100% oxygen inhalation via a mask at a flow rate of at least 10 liters per minute, which provided significant relief. However, in the following days, neither sumatriptan nor oxygen therapy continued to be effective.
Imaging studies, including a native CT scan of the brain, MRI of the brain, and MRI of the orbit without contrast, revealed no pathological findings. Additionally, laboratory tests, including a complete blood count, erythrocyte sedimentation rate, C-reactive protein, fasting blood sugar, glycated hemoglobin, thyroid function tests, kidney function tests, B12 levels, blood glucose, and blood pressure, were all within normal ranges. Following a neurological consultation, he was diagnosed with cluster headache associated with oculomotor nerve palsy.
In this case, diabetic oculomotor nerve palsy was considered as a possible differential diagnosis; however, due to the classic symptoms of cluster headache and the fact that the MRI did not show any signs of inflammation or thickening of the oculomotor nerve in the cavernous sinus—characteristic of microvascular damage caused by diabetes—this differential diagnosis is unlikely.
Initially, steroid therapy was avoided due to the patient's diabetes and arterial hypertension, as there were concerns about possible exacerbating these conditions. However, after observing a negative progression of headache symptoms, he was advised to keep the affected eye closed and was started on a low dose of daily 50 mg of oral prednisolone for one week, with a gradual reduction of 10 mg per day. He exhibited gradual improvement in ocular symptoms, along with fewer attacks, shorter durations, and lower intensity of headaches during the first week. Throughout the treatment with oral steroids, the oculomotor nerve palsy resolved, and there were no recurrences of cluster headaches. After completing the course of oral prednisolone, the patient continued on verapamil at a dose of 80 mg three times a day, with no reported episodes of cluster headaches since starting the Verapamil about three months ago.
Discussion
Cluster headache is a primary headache disorder classified under trigeminal autonomic cephalalgias. It is characterized by severe unilateral pain lasting from 15 to 180 minutes, usually at night, but can occur multiple times a day and is often described as "boring" or "piercing," and typically affects individuals aged 20 to 40, with a higher prevalence in males. The attacks can occur in cycles lasting weeks to months, with periods of remission. Some attacks may last for several years, with chronic cases showing no remission for at least a year.
Risk and trigger factors include smoking, medications (as histamine, nitroglycerin), high altitudes, alcohol use, changes in the environment, daily rhythms, switching sleep patterns from REM to non-REM, alterations in mental or physical activities, and a family history of the condition.
The pain is accompanied by autonomic symptoms such as rhinorrhea, eyelid swelling, and miosis, which help differentiate cluster headaches from other conditions like migraines and trigeminal neuralgia. While our case aligns with cluster headache criteria, the presence of oculomotor nerve palsy complicates the diagnosis, as this combination is uncommon.
Like cluster headache, other abnormalities can present with both pain and third nerve palsy such as recurrent ophthalmoplegic neuropathy, Tolosa–Hunt syndrome, vascular lesions, and inflammatory diseases. However, the clinical picture along with the history and normal investigations make cluster headache the most probable diagnosis. Cluster headache with ophthalmoplegia is a rare presentation. Nonetheless, few cases have been prescribed with the third cranial nerve palsies.
One theory suggests that the swelling of the internal carotid artery in the cavernous sinus directly affects the oculomotor nerve during these attacks. Similarly, Horner syndrome can occur when the sympathetic nerves adjacent to the swollen artery are involved.
Other differential diagnoses include temporal arteritis, paroxysmal hemicrania, SUNCT syndrome, migraines, tension headaches, and Raeder's paratrigeminal syndrome.
The diagnosis primarily relies on clinical evaluation, but misdiagnosis is common, often delaying accurate treatment for years. The International Classification of Headache Disorders outlines specific criteria for cluster headaches, emphasizing the need for thorough history-taking.
The exact pathophysiology behind cluster headaches remains elusive, but it is believed to involve vasodilation of cerebral blood vessels, with a complex interplay between neurovascular changes and the trigeminal-autonomic reflex, which is activated during attacks. This reflex pathway connects the trigeminal nerve to cranial autonomic functions, leading to characteristic symptoms such as lacrimation and nasal congestion. Oculomotor nerve involvement can result in varying degrees of muscle dysfunction, leading to symptoms of eye muscle dysfunction such as ptosis and varying degrees of palsy. The hypothalamus also appears to play a central role, with evidence suggesting that circadian rhythms and melatonin secretion correlate with cluster headache patterns.
Functional neuroimaging studies have shown activation of the posterior hypothalamus during attacks, further supporting its involvement. Treatment targeting this area through deep brain stimulation has shown promise, highlighting the need for continued research into the underlying mechanisms and effective therapies for cluster headaches.
Although medications like high-flow oxygen and sumatriptan can abort the attacks, prophylactic treatments such as verapamil, lithium, and corticosteroids, which are thought to reduce histamine levels and stimulate endorphin release, are often necessary to prevent future episodes. Recent studies indicate elevated levels of calcitonin gene-related peptide (CGRP) and decreased melatonin during attacks, suggesting a link to trigeminal activity and hypothalamic dysfunction.
Neuroimaging, such as Cranial MRI, is essential to rule out structural abnormalities, particularly in patients with symptoms resembling other headache types or conditions like pituitary tumors. Distinguishing cluster headaches from other trigeminal autonomic cephalalgias and primary headache disorders is crucial for appropriate management.
Overall, understanding cluster headaches requires a comprehensive evaluation and awareness of their unique presentation and mechanisms.
Conclusions
Involvement of the extraocular muscles is a rare manifestation of cluster headaches, and both ophthalmologists and neurologists should be aware of this possibility. A short course of oral steroids is effective in managing third nerve palsy associated with cluster headaches and can help alleviate pain while preventing further attacks. These findings suggest a potential underlying inflammatory mechanism. A regimen of oral prednisolone followed by low-dose verapamil (240 mg/day) can be an effective prophylactic treatment for patients with cluster headaches.
Ethics Approval and Patient Consent:
Written informed consent was obtained from the patient.
Consent for Publication:
The patient provided written informed consent for publication of this case report along with his images.
Declaration of Patient Consent:
The authors confirm that all necessary patient consent forms have been obtained. The patient has consented to the publication of his images and clinical information in the journal. He understands that his name and initials will not be published, and efforts will be made to maintain anonymity, although complete anonymity cannot be guaranteed.
Financial Support and Sponsorship:
Nil.
Conflicts of Interest:
There are no conflicts of interest.

Figure 1

Figure 2
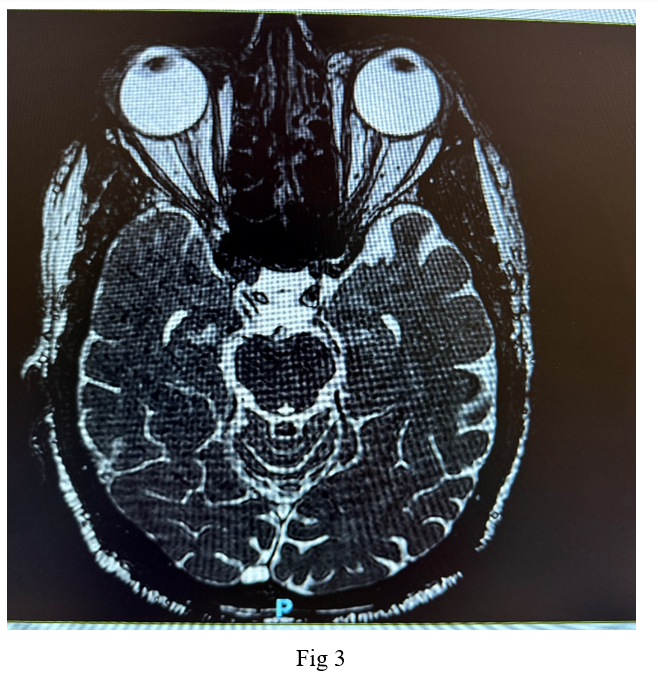
Figure 3