Neonate with Subpial Hemorrhage
Neonate with Subpial Hemorrhage
Amna Kashgari, MD.*1
*Correspondence to: Amna Kashgari, MD, King Saud bin Abdulaziz University for Health Science KSAU-HA. Medical Imaging Department, King Abdullah Specialized children's hospital (KASCH), Ministry of National Guard Health Affairs, Riyadh, Saudi Arabia.
Copyright
© 2023: Amna Kashgari, MD. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 16 August 2023
Published: 01 September 2023
Neonate with Subpial Hemorrhage
Introduction
A full-term male newborn was born at 38 w by normal vaginal delivery. He was born with low Apgar scores of 4 and 8 at 1 and 5 minutes. He developed repeated attacks of cyanosis admitted to NICU and required intubation. He developed seizure in the second day of life.
On examination, He was hypotonic and found to have right sided cleft lip and palate. There was no history of birth trauma, however, meconium liquor was recorded. Initial investigation included neonatal metabolic screening was negative. The CBC, coagulation profile, renal and liver function tests were normal. Abnormal waves were confirmed on electroencephalography (EEG). Supportive treatment and anticonvulsants were initiated.
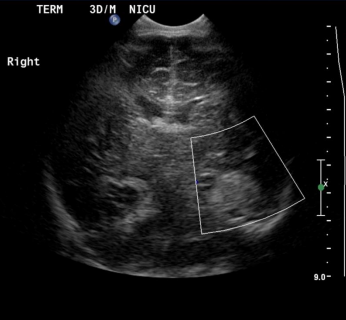
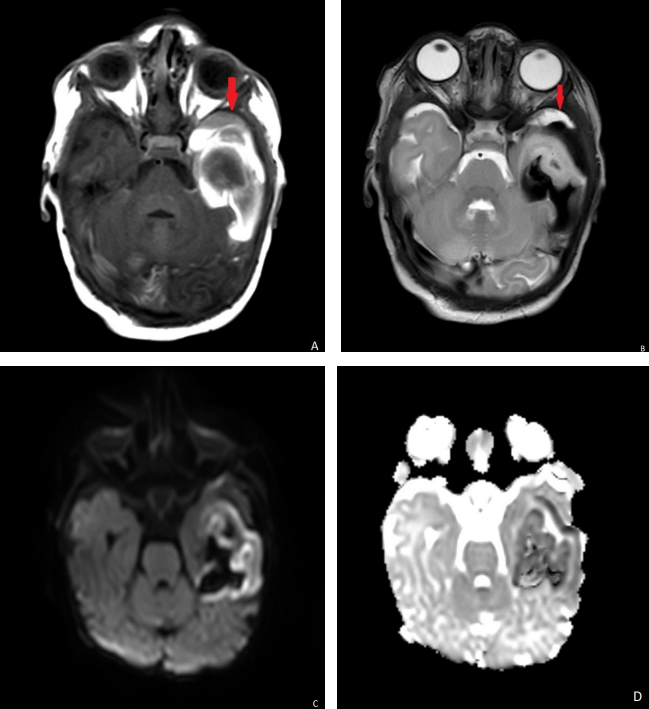
Ultrasound head showed left temporal lobe increased echogenicity with loss of normal gray-white matter differentiation with no flow on Doppler interrogation most likely represent hemorrhage. (Fig. 1). MRI scan was done on day 6 showed extra axial hemorrhage with high signal intensity on T1-weighted images and low signal intensity on T2-weighted images in the left temporal lobe opposing the underlying sulci and separate from the adjacent CSF (Fig. 2A and B). It showed mass effect on the adjacent cortex with cortical high signal intensity on T1 and T2-weighted images with evidence of diffusion restriction (Fig2 C, D). The final diagnosis was subpial hemorrhage with adjacent cortical hemorrhagic infarction.
Discussion
The subpial space defined as the potential space bordered externally by the pia mater and internally by the external glial limiting membrane of the neocortex. Subpial hemorrhage defined as intracranial hemorrhage subtype recently recognized because of the advancement in MRI imaging. The incident is not known yet.
The pathophysiology assumed to be related to external force is applied to the pterion of the sutures which lead to spontaneous superficial parenchymal and leptomeningeal hemorrhage with subsequent venous congestion and infarction (1)
Subpial hemorrhage could be idiopathic. Nevertheless, there are many risks factors for subpial hemorrhage including birth trauma, venous sinus thrombosis, asphyxia, clotting abnormality, and increase intracranial pressure (2,3). Some authors suggested perinatal fetal distress as a mechanism for subpial hemorrhage (4).
The clinical presentation includes neonatal seizure, seizures, encephalopathy and hypotonia.
Imaging criteria described as extra axial hemorrhage along the margin of the cerebral parenchyma extending into the cerebral sulci under the pia matter. The adjacent cortes show venous congestion or infarction in most of the cases.
The appearance of the hemorrhage described by Assis Z (1) as Yin-yang symbol with hypointense subpial hemorrhage and the underlying hyperintense cerebral cortex on T2-weighed image. The most common location of the hemorrhage is temporal lobes, followed by the frontal, parietal and occipital lobes. (5)
The clinical outcome varies according to the extent of the injury, Cole et al study showed that 44% of patients with subpial hemorrhage showed neurological deficit in follow up. (3)
Reference
1. Assis Z, Kirton A, Pauranik A, Sherriff M, Wei XC. Idiopathic neonatal subpial hemorrhage with underlying cerebral infarct: imaging features and clinical outcome. Am J Neuroradiol 2021;42(1):185–93. doi:10.3174/ajnr.A6872…
2. Armstrong-Wells J, Johnston SC, Wu YW, Sidney S, Fullerton HJ. Prevalence and predictors of perinatal hemorrhagic stroke: results from the kaiser pediatric stroke study. Pediatrics. 2009;123(3):823-828.
3. Cole L, Dewey D, Letourneau N, Kaplan BJ, Chaput K, Gallagher C, et al. Clinical characteristics, risk factors, and outcomes associated with neonatal hemorrhagic stroke: a Population-Based Case-Control Study. JAMA Pediatr. 2017;171:230–238. doi: 10.1001/jamapediatrics.2016.4151.
4. Cain D, Dingman A, Armstrong J, et al. Subpial Hemorrhage of the Neonate. Stroke. 2020;51:315-318. doi: 10.1161/STROKEAHA.119.02598
5. Barreto A, Carrasco M, Dabrowski A et al. Subpial Hemorrhage in Neonates: What Radiologists Need to Know. AJR 2021; 216:1056–1065. doi.org/10.2214/AJR.20.22999..
6. Braimbridge VM, Keith IH. Oesophago-bronchial fistula in the adult. Thorax. 1965;20:226–33.