A Case Report of Knee Stifnees as A Sequale of Elastic Nail Fixation for Femur Shaft Fracture in a Child
A Case Report of Knee Stifnees as A Sequale of Elastic Nail Fixation for Femur Shaft Fracture in a Child
Dr. Dinesh Kumar *1, Dr. Chandandeep Kaur 2
1,2. Senior Resident, Government Medical College, Amritsar.
*Correspondence to: Dr. Dinesh Kumar, Senior Resident, Government Medical College, Amritsar.
Copyright
© 2023 Dr. Dinesh Kumar. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 18 August 2023
Published: 01 September 2023
Abstract
As femur shaft fracture in paediatric population are managed by ESIN, to maintain length, rotation and alignment in both diaphyseal and metaphyseal fractures. But some time improper position of entry of ESIN may lead to uneventful condition. As we are discussing here about the entry of ESIN is anteriorly, which leads to stiffness of knee joint as a complication of ESIN fixation due to improper entry of nail.
Keywords: Femur Shaft fracture, Paediatric femur fracture, ESIN, Intramedullary nail.
A Case Report of Knee Stifnees as A Sequale of Elastic Nail Fixation for Femur Shaft Fracture in a Child
Background
As femur shaft fracture in paediatric population are managed by ESIN, to maintain length, rotation and alignment in both diaphyseal and metaphyseal fractures. But some time improper position of entry of ESIN may lead to uneventful condition. As we are discussing here about the entry of ESIN is anteriorly, which leads to stiffness of knee joint as a complication of ESIN fixation due to improper entry of nail.
Introduction
Elastic stable intramedullary nailing (ESIN) is primary definitive care for shaft fracture in paediatric orthopaedic practice.[1] In 1882 Mataizeau & his team from France developed and revolutionized the technique of flexible stable intramedullary pinning (FSIP) using titanium pins which is now popularly known as TENS has become the choice of operative management for paediatric femoral shaft fractures.[2]
History & Examination:
A 10-year-old male patient fell from a height and sustained a direct damage to the shaft of his femur, for which he underwent elastic nail fixation a year ago. He now complains of thigh pain, trouble walking, and knee stiffness for the past six months. On examination, the patient was critically stable, with no head, chest, or abdominal damage, and a normal hip and spine assessment. On local examination, there was swelling with a discharging sinus in the mid-thigh over the anterolateral aspect of 11x4.1 centimetres (superior to inferior and anterior to posterior), with two linear scar marks healed with primary intention over the distal thigh in the medial and lateral aspects, a temperature raised locally, and tendered swelling. Hip joint movements were within normal limits, and knee extension was normal.
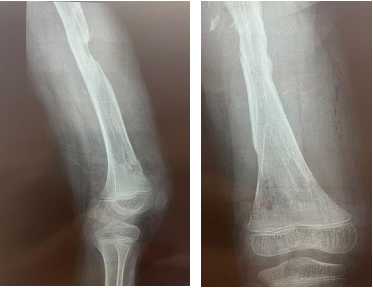
All routine investigations were ordered, including an X-ray of the thigh with knee AP and lateral views and an ultrasound for local swelling. On ultrasound, there was a swelling of 11x4.1 centimetres (superior to inferior and anterior to posterior) in the anterolateral part of the mid-thigh, connecting with a sinus measuring 4mm in diameter and not engaging any joint structure.
Intraoperative
After suitable painting and draping, an incision was made near the old scar mark on the medial side of the distal thigh under C-ARM control, after tissue dissection, the bone cortex of the medial side of the femur was pierced with a drill, and the end of the elastic nail was felt and retrieved with the use of a T handle. In the case of the lateral side of the elastic nail, an incision was made over the old scar mark, as deepening the incision revealed a collection of pus containing around 200-300 ml. The entire collection was drained and the elastic nail end was felt and retrieved using pliers and a hammer. Irrigation with normal saline and betadine was performed on both sides, and gentamycin was then administered locally. The wound was closed with silk and an antibiotic dressing was applied. Even after the elastic nails were removed, the knee remained stiff.
Discussion
Femoral shaft fracture is the most common major paediatric orthopaedic injury requiring hospitalization. It represents about 1.6% of all the bony injuries in children (Including sub-trochanteric & inter-trochanteric fractures). They are more common in boys than girls (2.6:1).[3][4]
The techniques and tips of better TENS Nail fixation for femur fracture evolved with time. The entry point of TENS Nail For the ascending technique, the insertion points on the femur are 1–2 cm proximal to the distal epiphyseal plate. In children, this is about one fingerbreadth proximal to the upper pole of the patella. Make the opposing medial and lateral skin incisions at the planned insertion points and cut distally for 3–4 cm, depending on the size of the child. On the lateral side especially, the incision of the fascia should be of the same length.[5]
The most common complication of Titanium elastic nail is entry site irritation and pain. Other complications include limb length discrepancy, angulation of fracture, refractures and infection. Entry site irritation was significantly associated with long and prominent nail end (>2 cm). Smaller and mismatch nail diameter that was incidentally used was associated with increased incidence of varus/valgus angulation.[6]
If it was open, where the soft tissue severely damaged. A large open femoral shaft fracture with adhered, retracted scar tissue is a sign of quadriceps adhesions to the femur, which crossed through the quadriceps and skin at the time of the injury.
There are two type of knee stiffness flexion and extension type and each type may have component of intraarticular or extraarticular type. In extra-articular: quadriceps adhesions to a femoral callus, femoral aponeurosis and intermuscular septum, retraction of the muscle due to scar tissue and skin adhesions in the deeper layers.
Injury to quadriceps may be the extraarticular component for knees stiffness.[7]
As a result of the femur shaft fracture, there was no involvement of the knee joint even after elastic nail fixation, no extension of the elastic nail distally, no scar mark over the knee, but on pre-operative x-ray, the medial side elastic nail was not medially but anteriorly. Quadriceps muscles are located anteriorly and are more prone to adhesion and contracture as a result of injury and inflammation. Because to long-term irritation of the vastus intermedialis muscle near the distal end of the medial side elastic nail, adhesion and contractures form, resulting in knee stiffness.
Reference
1. Marengo L, Nasto LA, Michelis MB, Boero S. Elastic stable intramedullary nailing (ESIN) in paediatric femur and tibia shaft fractures: Comparison between titanium and stainless steel nails. Injury. 2018 Nov;49 Suppl 3:S8-S11. doi: 10.1016/j.injury.2018.09.049. PMID: 30415674.
2. Metaizeau J.P. Osteosynthesis in children: techniques and indications (in French) Chir Pédiatr. 1983;69:495–511
3. Flynn JM, Hresko T, Reynolds RA, Blasier RD, Davidson R, Kasser J. Titanium elastic nails for pediatric femur fractures: A multicenter study of early results with analysis of complications. J Pediatr Orthop. 2001;21:4–8
4. Heybel1y M, Muratli HH, Çeleb L, Gülçek S, Biçimoglu A. The results of intramedullary fixation with titanium elastic nails in children with femoral fractures. Acta Orthop Traumatol Turc. 2004;38:178–87.
5. https://www.rch.org.au/uploadedFiles/Main/Content/ortho/TEN-Titanium_Elastic_Nail.pdf
6. Narayanan, Unni G. MD*; Hyman, Joshua E. MD‡; Wainwright, Andrew M. FRCS§; Rang, Mercer FRCSC||†; Alman, Benjamin A. MD||. Complications of Elastic Stable Intramedullary Nail Fixation of Pediatric Femoral Fractures, and How to Avoid Them. Journal of Pediatric Orthopaedics 24(4):p 363-369, July/August 2004.
7. Pujol N, Boisrenoult P, Beaufils P. Post-traumatic knee stiffness: surgical techniques. Orthop Traumatol Surg Res. 2015 Feb;101(1 Suppl):S179-86. doi: 10.1016/j.otsr.2014.06.026. Epub 2015 Jan 9. PMID: 25583236.