Spheroidal Degeneration: A Case Report
Spheroidal Degeneration: A Case Report
Zineb Algouti *1, Oumayma El Mansouri 2, Houssaine Ait Lhaj 3, Mohamed Kriet 4, Fouad Elasri 5
1. Department of ophthalmology of Avicenna Military Hospital Marrakesh 40000,
Faculty of Medicine and pharmacy, University Caddi Ayyad.
2. Department of ophthalmology of Avicenna Military Hospital Marrakesh 40000.
Faculty of Medicine and pharmacy, University Caddi Ayyad.
3. Department of ophthalmology of Avicenna Military Hospital Marrakesh 40000.
Faculty of Medicine and pharmacy, University Caddi Ayyad.
4. Department of ophthalmology of Avicenna Military Hospital Marrakesh 40000.
Faculty of Medicine and pharmacy, University Caddi Ayyad.
5. Department of ophthalmology of Avicenna Military Hospital Marrakesh 40000.
*Correspondence to: Zineb Algouti, Department of ophthalmology of Avicenna Military Hospital Marrakesh 40000, Morocco.
Copyright
© 2023 Zineb Algouti. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 17 August 2023
Published: 01 September 2023
Spheroidal Degeneration: A Case Report
Key Words: Spheroidal degeneration, Climatic droplet keratopathy, Fisherman’s keratopathy, corneal degeneration.
Description of the case: An 80-year-old man was admitted to our hospital for progressive bilateral degradation of visual acuity in both eyes, and a history of foreign body sensation and chronic lacrimation. The patient worked outdoors for 25 years, in the desert.
His best-corrected visual acuity was hand motion in the right eye, and 4/10 in the left.
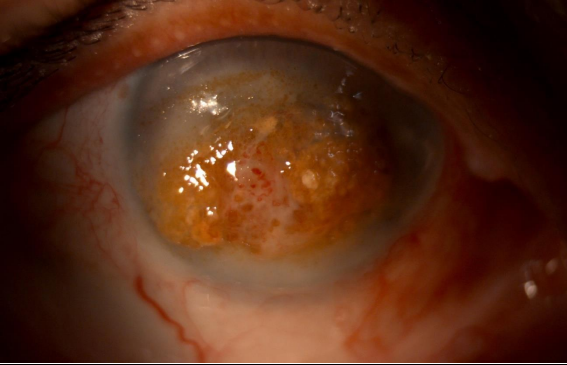
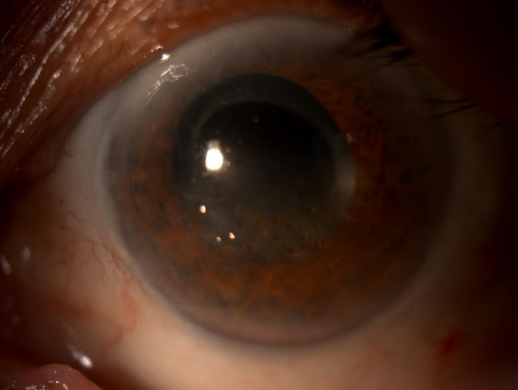
Slit lamp examination showed a dense, band-shaped, yellow-colored plaque of elevated nodules across the central cornea extending horizontally within the palpebral fissure in the right eye (Fig1). In addition, translucent, golden yellow, droplets located in the subepithelium of the left (Fig 2).
The patient was addressed for corneal transplantation, and was lost to follow up.
Spheroidal degeneration also called Climatic droplet keratopathy (CDK), Fisherman’s keratopathy (1), is an acquired and potentially handicapping corneal degenerative disease that is highly prevalent in certain areas with high exposure to ultraviolet light, low humidity, high wind, and presence of sand(2).
Reference
1. Meyer JJ. Climatic Droplet Keratopathy (Spheroidal Degeneration). In: Schmidt-Erfurth U, Kohnen T, éditeurs. Encyclopedia of Ophthalmology. Berlin, Heidelberg: Springer Berlin Heidelberg; 2014
2. Elhusseiny AM, El Sheikh RH, Jamerson E, Swaify IY, Araissi AB, Saad AA. Advanced spheroidal degeneration. Digit J Ophthalmol. 22 déc 2019; 25(4):68?71.