Giant Cystic Degeneration of a Nasal Pterygium
Giant Cystic Degeneration of a Nasal Pterygium
Dr Farah Benlkadri *1, Dr Basma Ouidani 2, Dr El Mehdi El Filali 3, Dr Youssef Bennouk 4,
Pr Hussein Ait Lhaj 5, Pr Mohamed Kriet 6, Pr Fouad Elasri 7
1. Military Hospital of Marrakech, Ophthalmology Department University Cadi Ayad, Marrakech.
*Correspondence to: Dr Farah Benlkadri, Military Hospital of Marrakech, Ophthalmology Department University Cadi Ayad, Marrakech.
Copyright
© 2023 Dr Farah Benlkadri. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 23 August 2023
Published: 01 September 2023
Giant Cystic Degeneration of a Nasal Pterygium
Pterygium is a degenerative condition of unknown origin and pathogenesis, which presents as fleshy mass of the bulbar conjunctiva usually triangular in shape into the cornea.[1] Pathologically it is a proliferation of the subconjunctival tissues as vascularized granulation which has a tendency to involve stroma of the cornea.[2]
Usually, it is a benign disease, but sometimes its stroma can show cystic degenerative change and even worse, malignant transformation can be seen in epithelium. [2]
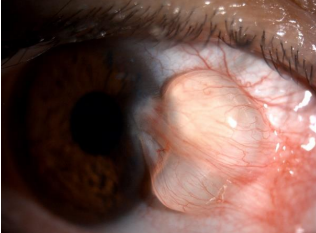
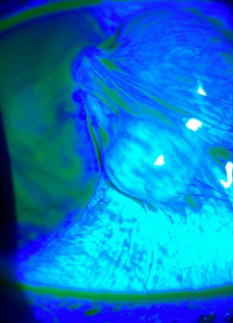
The patient was a 39 year old male, presented foreign body sensation in right eye without any history of surgery or trauma. Nasal pterygeum along with a horizontally oval cystic swelling in the body of pterygium was noted (Figure1,2).
The cyst was stationary in its size without any signs of inflammation during 3 months of follow-up.
In view of the patient's discomfort and the ocular dryness caused by the dellen effect due to the cystic pterygium, surgical excision was performed with a hitopathological analysis.
Microsocopic examination revealed that the wall of conjunctival cyst consisted of non-keratinizing stratified squamous epithelial cells. Signs of elastotic degeneration were present without signs of malignancy or inflammatory reaction surrounding the cyst.
The inflammatory origin of cystic degeneration of the pterygium is the most supported [3], the absence of inflammatory stigmata in the histology suggests a degenerative origin in our case.
Figure 1. Front view image showing cystic swelling in the body of pterygium
Figure 2. Slit Lamp image with fluorescein instillation showing cystic swelling in the body of pterygium
References
1. Peckar C.O. (1972). The aetiology and histo-pathogenesis of pterygium. A review of the literature and a hypothesis. Doc. Ophthalmol. 31, 141-157.
2. Duke-Elder, S, and Leigh, A.G., 1965, Sys. Of Ophtha, 3, 573.
3. Kapoor S, Sood G C, Aurora A L, Kapoor MS, Cystic degeneration of pterygeum. Indian J Ophthalmol 1977; 25:37-8. 3wsz