Clinical, Etiological, Therapeutic and Evolutionary Study of Upper Gastrointestinal Bleeding in the Democratic Republic of Congo
Clinical, Etiological, Therapeutic and Evolutionary Study of Upper Gastrointestinal Bleeding in the Democratic Republic of Congo
Mungwete Josue B *1,2,5, Byabene Aline K 2,5, Mugisho Mastaki 1,2,5, Mukwege Lisa B 2,5,
Baraka Jeanne D'arck 5, Alumeti Desiré 3, 5, Van Gossum Marc 4.6
1. Hepato-gastroenterology and digestive oncology department.
2. Internal Medicine Department of Panzi General Reference Hospital.
3. Panzi General Referral Hospital Surgery Department.
4. Gastroenterology department of the Saint Pierre University Clinic in Brussels.
5. Evangelical University in Africa.
6. Free University of Brussels.
*Correspondence to: Dr Mungwete Josué, Hepato-Gastroenterologist, Head of department of Gastroenterology and Digestive Oncology at Panzi General Reference Hospital, Teacher of Medicine at the Evangelical University in Africa.
Copyright
© 2023 Dr Mungwete Josué. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 26 August 2023
Published: 01 September 2023
Abstract
Problematic: Upper gastrointestinal bleeding remains a major health problem, given their potential seriousness and the urgency they create both diagnostically and therapeutically. In developing countries, morbidity and mortality remains high due to delayed diagnosis, care, financial problems and inaccessibility to emergency endoscopy.
Objective: To study the clinical, endoscopic, etiological, therapeutic and evolutionary aspects of upper gastrointestinal bleeding in the Department of Gastroenterology of the General Reference Hospital of Panzi/Bukavu.
Methods: This was a descriptive and analytical retrospective study of 133 patients admitted for upper gastrointestinal bleeding in the Gastroenterology department of the Panzi General Reference Hospital over a period from April 1, 2014 to April 30, 2022. A tertiary hospital located in Bukavu, in the province of South Kivu, in the Democratic Republic of Congo. Cases were collected from registers and/or patient files in archives. The data collected was analyzed using SPSS 20 software . We analyzed the epidemiological characteristics, in particular age, sex, origin; clinical, endoscopic and therapeutic characteristics using SPSS 20 software. Interpretation of results in the form of percentages and P-value, with statistical significance if p < 0.05.
Results: We noted a prevalence of 8.5%, the age group between 46 – 60 years is predominant (37%), with an average age of 47.9 ±17.5 . The male gender is predominant with 61.6% of cases with a sex ratio of 1.6. The first etiology is the rupture of esophageal varices in 43% of cases, the most used endoscopic treatment in 60.1% of cases and the evolution is favorable in 93.2% of cases. There is a correlation between hematemesis and VO rupture with a P-value of 0.0359 but also between portal hypertension with cirrhosis with P-value at 0.0112.
Conclusion: Upper gastrointestinal bleeding is one of the most common digestive emergencies. Hematemesis is the main mode of externalization, rupture of esophageal varices the first cause and the advent of interventional endoscopy is a major asset in the management.
Clinical, Etiological, Therapeutic and Evolutionary Study of Upper Gastrointestinal Bleeding in the Democratic Republic of Congo
Introduction
Upper gastrointestinal bleeding (HDH) is bleeding occurring upstream of the duodenojejunal angle or the angle of Treitz, representing 80 to 90% of gastrointestinal bleeding worldwide [ 1]. However, they constitute a major health problem in the world, given their potential seriousness and the urgency they create both diagnostically and therapeutically. In France, the incidence of upper gastrointestinal bleeding is 65,000 cases per year with hospital mortality of 14% [8].
In developing countries, morbidity and mortality remains high due to delayed diagnosis, care, financial problems and inaccessibility to emergency endoscopy. This is a reason for recourse to emergencies whose main etiologies are portal hypertension, ulcerative disease and acute gastritis. In about 10% of cases, a rarer cause (Mallory-Weiss, acquired vascular malformations, etc.) is responsible [2, 3].
The management of HD requires an etiological diagnosis without delay in order to ensure a specific treatment. The use of digestive endoscopy has nowadays become frequent and regularly essential in its etiological diagnosis and its management whatever the age. [4]. The management of HD is multidisciplinary and calls on the skills of resuscitators, gastroenterologists, radiologists and surgeons. Nevertheless, mortality remains heavy, as some studies report: 5.4% in Benin [5]; 11.8% in Abidjan [6]; 5 to 20% in a European series [7], despite advances since the widespread use of endoscopy.
In the Democratic Republic of Congo, very few data are available on digestive bleeding, but none have been carried out in the east of the country. We therefore thought it useful to carry out such a study in order to take stock of digestive haemorrhages, in their epidemiological, clinical, therapeutic and evolutionary aspects.
Method
This was a descriptive and analytical retrospective study of 211 patients admitted for upper gastrointestinal bleeding in the gastroenterology department of the Panzi General Reference Hospital, over a period from April 1, 2014 to April 30. 2022, i.e. a period of 8 years. This hospital is located in Bukavu, in the province of South Kivu, in the Democratic Republic of Congo. Overall, the study involved 211 patients admitted for upper gastrointestinal bleeding out of a total of 374 patients admitted for general digestive bleeding and 2476 fibroscopies performed in the department during this study period.
Cases were collected from patient records in archives , hospital records, and/or the endoscopy register. We analyzed the epidemiological characteristics, in particular age, sex, origin; clinical, paraclinical and therapeutic characteristics using SPSS 20 software. Interpretation of results in the form of percentages and P-value, with statistical significance if p < 0.05.
Results
The socio-demographic characteristics of the study population include 66.3% men and 33.7% women. The age group of 31 – 60 years is the most represented with a prevalence of 60.1% of cases. Statistically, men are more likely to present with gastrointestinal bleeding than women (p=0.000) and upper digestive bleeding is more found in patients under 60 years of age (p=0.0175). Table 1.
The results recorded in Table 2 indicate that upper gastrointestinal bleeding was statistically related to history of taking NSAIDs, known ulcerative diseases, known cirrhosis and history of known portal hypertension (p < 0.0001) .
The observation of table 3 highlights the following findings: clinically, patients presented hematemesis as the main manifestation of HDH, p-value=0.030 (58.9%).
In 58.8% of cases the hemorrhage was moderately heavy, and this amount was statistically associated with patients who came for upper gastrointestinal bleeding (p=0.040). On descriptive analysis, conjunctiva staining was not predictive of upper gastrointestinal bleeding (p=0.392). However, among the signs portal hypertension found on physical examination, ascites was statistically found in patients with upper gastrointestinal bleeding (p=0.000), i.e. 100% of patients who had ascites on physical examination also presented the signs of upper gastrointestinal bleeding.
The results reported in Table 4 indicate that upper gastrointestinal bleeding was statistically related to esophageal varices, (p=0.000), and the primary method of management was variceal ligation, (p=0.0056).
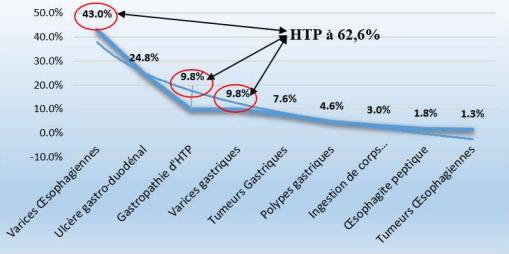
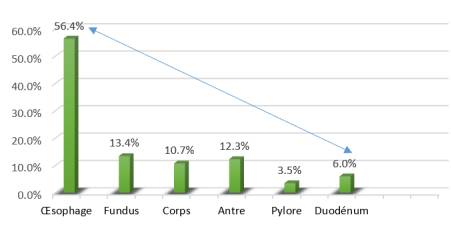
Figure 1 shows us in the abscissae the proportion of etiologies in percentage and in the ordinates, there are the etiologies of the upper digestive hemorrhages, of this figure it is necessary to specify that 62.6% of the etiologies are of portal hypertensive origin, (Figure 1) . Regarding the location of the lesion, 56.4% are found in the esophagus ( Figure 2) .
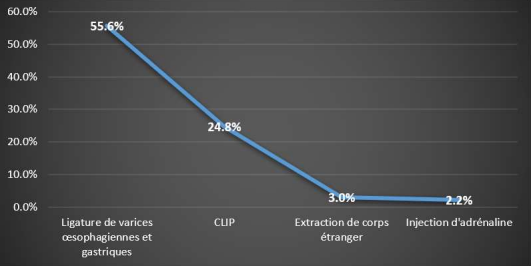
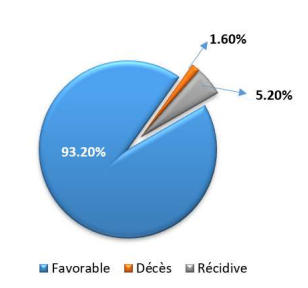
It should be noted that the ligation of the varices was the most used treatment in 55.6% of the cases and in 93.2% of the cases the evolution of the patients was favorable . (Figures 3 and 4).
Table 1. Sociodemographic characteristics of the study population.
Table 2. Patient history.
Table 3. Parameters clinics of the patients.
Table 4. Endoscopic data and management.
(Please refer to the attched pdf to view tables)
Figure 1. Etiologies of upper gastrointestinal bleeding.
Figure 2. Differences localisations de la lésion
Figure 3. Endoscopic treatments performed
Figure 4. Evolution of patients
Discussion
Prevalence
Of the total of 2476 endoscopies performed in the department during our study period, 211 were performed for upper gastrointestinal bleeding, ie a prevalence of 8.52%. Our results are close to those found by Mariam G KOUMARE and All in Mali in 2019 [11], who found a prevalence of 5.5%. However, they are far from those found by KONATE et al in Bamako [9], DIARRA et al [10], who respectively found a prevalence of 2.5% and 1.6%.
These results can be explained by the difficulties of access to care, due to a lack of financial means, the absence of medical supervision resulting in a lot of pathology, in particular . chronic liver diseases are not diagnosed in time.
Sociodemographic characteristics
Age
By observing the table above, we find that the age group between 31 and 60 years old was more affected with a number of 135 out of 211 patients admitted for upper gastrointestinal bleeding, i.e. 63.9%, with an average age of 47.9 ±17.51 and the extreme age groups between 11 and 85 years old. A statistical association was found between upper gastrointestinal bleeding, this age group and age less than or equal to 30 years, P-value successively of 0.014 and 0.021.
These results are close to those reported by ZARHOUNI in Bordeaux [12], who found that the average age was 64 years. and those of Mariam G KOUMARE in Mali [11], who found that the patient whose age is less than 46 ± 15 years was the most predominant in Bamako.
Sex
The results of our study show us that the male sex was the most affected with a number of 130 out of 211 cases or 61.6% and only 38.4% for the female sex. A statistically significant link was found between male gender and upper gastrointestinal bleeding (P-value < 0.0001).
Our results converge with those of RAZAFIMAHEFA et al in Madagascar [13], who found a high male prevalence of 67.5%.
The same findings were made by the different series, A. El Mekkaoui and All in Morocco, with 63.5% of men and P-value < 0.0000001 [24]. KONATE and Mariam G KOUMARE [11, 9] have similarly found male prevalence. This prevalence, which could be explained by the more frequent exposure of men to risk factors for the onset of cirrhosis and therefore of its hemorrhagic complications.
Background
In our series, we find that the majority of our patients had a history of either regular NSAID intake (76.7%), or known portal hypertension (61.6%) or chronic vomiting (72.9%). ). Nevertheless, a statistical link was found between HDH and the history of multiple transfusions, taking NSAIDs, known PH, known ulcer disease as well as patients with known cirrhosis with a P-value < 0.0001 in all cases. These results are close to those found by Rita SLIM, César YAGHI and All in France [23], who found that the history of taking nonsteroidal anti-inflammatory drugs was dominant in patients with HDH in 45.8% of cases. . These same results were found in the series of A. El Mekkaoui · I. Mellouki and All in Morocco, in which the antecedent of known ulcerative pathologies, notion of multiple transfusions and taking NSAIDs was statistically associated with upper gastrointestinal bleeding , (P-value < 0.0001.). [24]. However, our results diverge from those found by OUEDRAOGO J and All in Ouagadougou [16], who in their series had a history of peptic ulcer in 23.1% of cases. and those found by BOUR B [17], who found that cirrhosis was the main antecedent found in patients with HDH.
Clinics
In our study, the main manifestation of upper gastrointestinal bleeding was hematemesis (53.55%); of medium abundance (28.43%), thus ascites was the main associated sign (19.9%). The association between these signs and upper gastrointestinal bleeding was statistically significant with a P-value successively of 0.030; 0.040 and < 0.0001. Our result agrees with those of ES-SABIR in Marrakech [14] and AMAL [15] who had found hematemesis first as the mode of externalization of hemorrhage with respectively 68% and 71.5% of cases. . The series of R. Sombié · A. Tiendrébéogo and Al in Burkina Faso , identified a statistically significant relationship between hematemesis and upper gastrointestinal bleeding (P-value = 0.02; 95% CI) [25] . Nevertheless, our data disagree with those of Patrice Emery Itoudi Bignoumba in Libreville [22], who had found melena to be the main mode of revelation in 39% of cases.
Endoscopic data
Etiologies
In 62.6% of cases, the etiologies of upper gastrointestinal bleeding were secondary to the consequences of portal hypertension (oesophageal varices, gastropathy from portal hypertension and gastric varices); followed by 24.8% of cases of upper gastrointestinal bleeding related to gastroduodenal ulcers. A statistically significant link was found between esophageal varices and upper gastrointestinal bleeding (P-value < 0.001). These results are similar to those found by A ESSAID EL FEYDI and All in Morocco, who in his study would have found that gastroduodenal ulcers and esophageal varices are the main causes of HDH in 40% of cases. [18], and M. DIARRA, et al in Mali where the main etiology was esophageal varices in 55.2% of cases. [21]. However, our results diverge from those found by Salomé Ouazana1 at Sorbone [19], who found peptic ulcers to be the main cause in 36% of cases.
Location of the lesion
In our study, the esophageal localization of the lesion was predominant in 56.4% of cases, then at the level of the Fundus in 13.4% of cases. A statistically significant link was found between upper gastrointestinal bleeding and the esophageal location of the lesion (P-value = 0.019). Our results are similar to those reported by JR IBARA, B. MOUKASSA, et al in Brazaville [20] , who found that the esophageal location was involved in 41.81% of cases.
Supported.
55.6% of our patients benefited from ligation of esophageal and gastric varices. However, only ligation of esophageal varices was statistically associated with endoscopic management of upper gastrointestinal bleeding (P-value = 0.0056). Our results are similar to those reported by Rita SLIM, César YAGHI, Khalil HONEIN and All in France [23], in whom ligation of esophageal varices was the second most common endoscopic treatment performed in 25% of cases after the injection of diluted adrenaline in 43.75% of cases. A. El Mekkaoui. I. Mellouki and Al in Morocco, also found similar results with 72% of patients having benefited from ligation of esophageal varices [24] .
Evolution
The results of our study show that the majority of our patients had a favorable evolution in 93.2 % of cases and that 1.6% died. These results are close to those reported by M. DIARRA, et al in Mali [21], who found the outcome favorable in 77.6% of cases. But they are far from those found by Mariam G KOUMARE in Bamako [11], who in her study found a high mortality rate of 23.4% of cases.
Conclusion
Digestive hemorrhage by rupture of VO is one of the most formidable complications of portal hypertension frequently encountered in hospital settings. It is mainly manifested by hematemesis of moderate abundance, with a generally favorable evolution in the presence of early endoscopic management. This demonstrates the importance of the advent of interventional endoscopy in the management of gastrointestinal bleeding.
Reference
1. Mr. KIDA ABOUBACAR and All, digestive haemorrhages in children in the Pediatrics Department of the CHU GABRIEL TOURE, Original Thesis, Bamako, 02/07/2020.
3. X. Dray, N. Carbonell and All: Upper gastrointestinal bleeding, digestive endoscopy unit, digestive pole, Saint-Antoine hospital, 184, Rue du Faubourg-Saint Antoine, 75012 Paris, France. 2016
4. AROULANDOM J, LEMALE J, CHAPPUY H. Diagnosis of gastrointestinal bleeding in infants and children. Emergency Medicine 2018; 13(3):1-10
5. KODJOH. N, HOUNTONDJI.A, ADDRA.B. Contribution of endoscopy to the diagnosis of esogastroduodenal affections in tropical environment. Beninese experience about 930 exams. Ann. Gastroenterology. Hepatology .1991;21:261-
6. ATTIA Y., GAUDET D., CARSUZA M. Assessment of 15 months of upper digestive endoscopy at the University Hospital of Cocody. Rev. CI Med, 1981;54:16-22.
7. GRIMALDI CH., DELMONT JP. Gastrointestinal bleeding. EncyI. Med. Chir, Stomach-Intestine. 9006 A10, 1-1986, 14p
8. Arturt JP, Lesur G, Heresbach D and Al. Acute lower digestive haemorrhage, Acta endoscopica 2010; 40 (5): 379–383.
9. KONATE A, DIARRA MT, SOUKHO A, KATILE D, SOUMARE G, KALLE A ET AL. Digestive bleeding by rupture of esophageal varices, Mali Medical 2008; 23(3): 32-35 10.
10. DIARRA M, DIARRA S, DOLO M, TRAORE H, DIALLO A. Acute upper gastrointestinal bleeding: Experience from a rural setting. Acta Endoscopica 2017; 37(3):321-326
11. MARIAM GK, digestive hemorrhage by rupture of esophageal varices and prognostic value of blood transfusion in the hepato-gastroenterology department of CHU GABRIEL TOURE, Faculty of Medicine and Odonto-Stomatology, THESE, Mali Bamako, 2019,
12. HEIDI ZARHOUNI, Pre-hospital management of upper gastrointestinal bleeding at SAMU 33 in Bordeaux, Med Thesis, Bordeaux, 2014; 66
13. RAZAFIMAHEFA SH, RABENJANAHARY TH, RAKOTOZAFINDRAIBE R, Upper digestive bleeding: clinical, endoscopic and evolutionary aspects. About a series of 62 Malagasy patients, RMM2011;1(1):6-10
14. ES-SABIR E. Gastrointestinal bleeding in children. Thesis, Med, Marrakech, 2017
15. AMAL A. Upper gastrointestinal bleeding in children. Thesis, Med, Fez, 2013; 114/13
16. OUEDRAOGO.JAE Digestive bleeding in the Digestive Medicine Department of the CHNYO. Epidemiological, clinical and evolutionary aspects. Thesis Med. Ouagadougou, 2015, 108p
17. BOUR BMD Endoscopic treatment of upper gastrointestinal bleeding apart from portal hypertension. Gastrointestinal. Endosc, 2017.46: 27-32.
18. A ESSAID EL FEYDI and All,: endoscopic management of upper gastrointestinal bleeding, Morocco 2006
19. Salomé Ouazana1, Romain Leenhardt1: Management of upper gastrointestinal bleeding: did you say frequent and serious?, Sorbonne University, Digestive Endoscopy Department, Saint Antoine Hospital, APHP, 184 rue du Faubourg Saint-Antoine, 75012 Paris. 2021
20. Jr upper digestive pathology in the Congo about 2393 endoscopies performed at the Brazzaville teaching hospital. 2013
21. M. DIARRA (1), A. SOUCKO-DIARRA (1), M. DOLO (2), H. TRAORE (1), A. DIALLO (2) (1) Medical Service (2) Sikasso Regional Hospital (Mali) Acute Surgery Department, Acute upper gastrointestinal bleeding: Experience of a rural environment 2017.
22. Upper digestive haemorrhage at the University Teaching Hospital of Libreville: clinical aspects and real management of 210 patients. 2019
23. Rita SLIM, César YAGHI, Khalil HONEIN, Joseph BOU JAOUDÉ, Soha EL KHOURY, Raymond SAYEGH DIGESTIVE BLEEDING HIGH IDENTIFICATION OF PROGNOSTIC FACTORS France
24. A. El Mekkaoui · I. Mellouki · MA Berraho · K. Saâda · M. Elyousfi · N. Aqodad · M. El Abkari · C. Nejjari · A. Ibrahimi D. Benajah Epidemiology, etiology and outcome of acute upper gastrointestinal bleeding in the University Hospital of Fez, Morocco Epidemiology, etiology and outcome of acute upper gastrointestinal bleeding in the University Hospital of Fez, Morocco
25. R. SOMBIE A. TIENDREBEOGO ET AL ; Upper gastrointestinal bleeding: epidemiological aspects and prognostic factors in Burkina Faso (West Africa).