Paediatric Museum as A Teaching Tool
Paediatric Museum as A Teaching Tool
Vineetranjan Gupta 1*, Sunil Natha Mhaske 2
1. Paediatrician.
2. Professor and Dean DVVPF’s Medical college and Hospital, Ahmednagar, - 414111, Maharashtra, India.
*Correspondence to: Dr. Vineetranjan Gupta, MBBS, DNB (Paediatrics), MNAMS DCH, PGPN. Consultant Paediatrician.
Copyright
© 2023: Dr. Vineetranjan Gupta. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 26 August 2023
Published: 01 September 2023
Abstract
In the classroom, educators can present information to students many ways, whether via lecture, video, or readings. A lecture is the most widely used teaching method. Learning by lecture is a passive practice. Many pioneering techniques have been used to motivate students to have active attitude toward learning. In our method we are using museum as an innovative teaching-learning method. Aim and Objectives: To reduce the burden on teachers for academics and to have a better understanding of the Paediatric subject through this student-centred learning method. Material and methods: 98 undergraduate students of final MBBS from our Medical College were evaluated by dividing them into 2 groups of 49 students each. In 8th semester Group 1 was sent to the Paediatric Museum. Group 2 was taught through the traditional board-chalk and Power Point presentation method for an hour. The knowledge and understanding of the subject were then assessed through a written test and viva at the end of the 15-lecture series which was covered over 1 month. In next semester, the groups were exchanged and group 1 was sent to Paediatric Museum. After both groups were taught by both the methods, feedback was taken from all the students. Conclusion: Students who had attended the museum had a better understanding of the Paediatric subject and could reproduce the knowledge gained by them in a better way as compared to the students taught through the traditional method.
Keywords: Museum, Paediatric, Learning, Teaching
Abbreviations: MBBS (Bachelor of Medicine and Bachelor of Surgery).
Paediatric Museum as A Teaching Tool
Introduction
In this era, where medical education plays the most important role in shaping up of a doctor’s knowledge and ability to treat patients, the teacher’s duties are being more and more scrutinized [1]. Several teaching methods have been present since ancient times. For almost all the teaching methods present, presence of a well explaining, learned teacher is a must [2]. Effective medical education should be viewed as a continuum, integration of basic science and clinical medicine should occur throughout the curriculum and self-directed, lifelong learning should be emphasized [3]. One of the first natural history museums of the Ottoman Empire was established as a part of the Faculty of Medicine, est. 1827 in Istanbul where many of the leaders of the Young Turks movement were educated [4]. A concept “medical museum” as a sociocultural phenomenon is an institution or structural unit of the organization that uses exhibition, accounting stock, cultural, educational and research technologies to shape attitudes of the target audience towards life and health as the greatest social values and knowledge about scientific and practical activities for the preservation and strengthening of health, about the historical and modern diagnostic tools, treatment and prevention of diseases[5-6]. Paediatric museum has been designed to teach the students in a way which would enable their hearing and visual impressions to gain access to knowledge according to their own, individual understanding and grasping power [7].
Materials and Method:
98 undergraduate students of final MBBS from our Medical College were evaluated by dividing them into 2 groups of 49 students each. In 8th semester Group 1 was sent to the Paediatric Museum. Group 2 was taught through the traditional board-chalk and Power Point presentation method. The knowledge and understanding of the subject were then assessed through a written test and viva at the end of the 15-lecture series which was covered over 1 month. In next semester, the groups were exchanged and group 1 was sent to Paediatric Museum. After both groups were taught by both the methods, feedback was taken from all the students.
Result
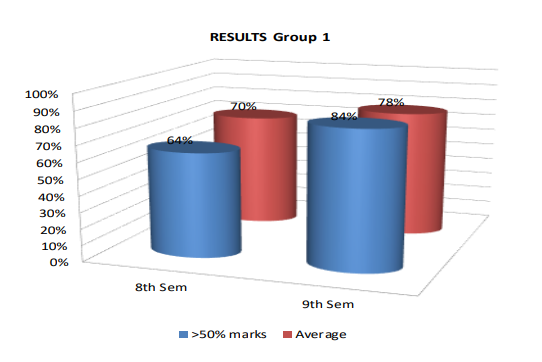
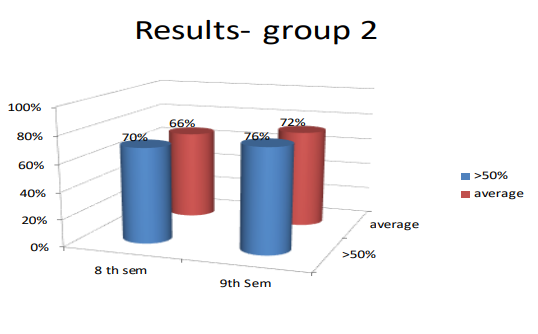
Group 1 scored 68% average marks and in that group 54% students got above 50%. While the average of group 2 which was taught in Paediatric Museum had an average of 84% and 68% scored over 50% marks.
To test the effectiveness of the method, we conducted a quasi-experimental study and then the students were asked to write their learning experiences in feedback form by a questionnaire method. A feedback form was prepared to take the input from the students regarding their experience during the interactive method, results of which are as follows:
Figure1,Figure 2, Table 1
Discussion
Medical education is an important factor in the progress of any country. Across the world, increasing attention is being given to the quality of teaching and learning in the medical colleges. Teaching is the noblest profession of all. A doctor is treated as equivalent to God who serves and saves the lives of the people. Our study showed that group 1 scored 68% average marks and in that group 54% students got above 50%. While the average of Group 2 which taught in Paediatric Museum had an average of 84% and 68% scored over 50% marks. The feedback showed that 99% of the students agreed or strongly agrees that learning and clearing their concepts was easier after visiting museum.
Students also strongly agreed that this method was time saving and helped them in memory retention. Teacher’s explanations enable students to understand the content and forging connections between what is known and what is new. Good teaching methods are open to change for effective teaching in the light of evidence collected [6]. There were few limitations of our study like small sample size and single centred study.
Although traditional medical education methods had produced thousands of well-known, efficient and successful doctors in both developed and developing countries there were increasing calls for fundamental changes in medical education to meet the needs of the community [7].
Conclusion
Students who had attended the museum had a better understanding of the Paediatric subject and could reproduce the knowledge gained by them in a better way as compared to the students taught through the traditional method. Various teaching and learning methods have been described in the literature and each of them have their own merits and demerits. To decrease the burden on teachers, the biases that can arise because of intrinsic individuality of the teachers and the learning capabilities of the students, the establishment of the innovative “Paediatric Museum as a learning tool” has proved to be worthy.
Reference
1.Minin Berg DT, et al. The art of death and dying: medical education in the Metropolitan Museum of Art’s Egyptian art galleries. Acad Med 2004;79(6):578-9.
2. Bardes CL, et al. Learning to look: Developing clinical observational skills at an art museum. Med Educ 2001;35(12):1157-61.
3. Haq C, et al. Integrating the art and science of medical practice: innovations in teaching medical communication skills. Fam Med 2004;36(Suppl): S43-S50.
4. Reinarz J. The age of museum medicine: The rise and fall of the medical museum at Birmingham’s School of Medicine. Soc Hist Med. 2005;18(3):419-437.
5.Bates, et al. Indecent and Demoralising Representations Public Anatomy Museums in Mid-Victorian England. Medical History. 2008; 52(1), 1-24.
6. Wojtczak, A. Glossary of Medical Education Terms. In MedEdWorld Glossary. (2003).
7. Sumera, A. Large Group Teaching, An Effective and Efficient Teaching Methodology. Journal of Asian Scientific Research, 2014; 4(1), 1–5.