Partial Joint Prosthesis following Hemi-Mandibulectomy in a Case of Recurrent Okc
Partial Joint Prosthesis following Hemi-Mandibulectomy in a Case of Recurrent Okc
K. Pawar1*, V. Ebenzer2 , R. Balakrishnan3
1,2,3. Sree Balaji Dental College and Hospital, Velachery Rd, VGP Rajesh Nagar, Pallikaranai, Chennai, Tamilnadu, Pincode- 600100.
*Correspondence to: K. Pawar, Sree Balaji Dental College, Pallikaranai, Chennai.
Copyright
© 2023 K. Pawar. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 30 August 2023
Published: 05 September 2023
Abstract
This abstract discusses the application of PJP in managing ROKC post-hemimandibulectomy. PJP aims to restore mandibular integrity, joint stability, and facial harmony. The prosthesis, usually consisting of custom-made condylar and fossa components, facilitates smooth articulation and proper occlusion. These implants are designed to withstand masticatory forces and facilitate physiological movement, enhancing patient quality of life.
Studies reveal favorable outcomes with PJP post-hemimandibulectomy, highlighting improved masticatory efficiency and psychological well-being. However, challenges include surgical complexity, risk of infection, and prosthesis-related complications. Patient selection, thorough preoperative evaluation, and precise surgical technique are imperative for success.
In conclusion, PJP implementation post-hemimandibulectomy for ROKC offers a functional and aesthetic solution, reinstating oral competence and facial balance. Further research is warranted to refine techniques, optimize outcomes, and address long-term efficacy.
Partial Joint Prosthesis following Hemi-Mandibulectomy in a Case of Recurrent Okc
Introduction
Recurrent odontogenic keratocyst (ROKC) is a perplexing pathological entity characterized by its aggressive and infiltrative growth pattern, resulting in extensive bone destruction. Its propensity for recurrence, even after seemingly successful treatments, has led to the exploration of innovative surgical approaches, such as partial joint prosthesis (PJP) usage, to address the functional and aesthetic challenges that arise following aggressive resections like hemimandibulectomy. This paper introduces the concept of utilizing PJP in cases of ROKC post-hemimandibulectomy, discussing its significance, surgical considerations, and potential benefits.
Significance of the Problem: ROKC poses a significant clinical challenge due to its high recurrence rate and potential for causing significant facial deformities and functional impairments. Hemimandibulectomy, often considered as a radical surgical intervention, is commonly employed to eradicate the lesion. However, such extensive resections result in substantial loss of mandibular bone, leading to compromised masticatory function, facial asymmetry, and psychological distress for patients. Reconstructive solutions that restore both function and aesthetics are paramount in such cases.
Partial Joint Prosthesis (PJP): PJP, a surgical approach originating from the field of maxillofacial prosthetics and orthopedic joint replacement, has gained attention as a potential solution for the functional rehabilitation of patients following hemimandibulectomy for ROKC. PJP involves the implantation of a custom-designed prosthetic joint that mimics the temporomandibular joint's structure and function. It consists of components resembling the condyle and glenoid fossa, promoting smooth articulation and restoring proper occlusion. Also, the implant prosthesis helps to provide dental rehabilitation once the healing period is completed. PJP enables mandibular movement, thereby addressing the masticatory impairment caused by extensive bone loss.
Surgical Considerations: The implementation of PJP in ROKC cases necessitates meticulous planning and execution. Precise preoperative assessment is vital, involving thorough radiographic evaluation, three-dimensional imaging, and assessment of occlusion. Customization of the prosthesis based on the patient's anatomy ensures optimal fit and function. Surgical placement demands expertise to ensure proper alignment, stability, and minimal disturbance to adjacent structures. Integration of PJP with the remaining native bone and soft tissues is crucial for long-term success.
Potential Benefits: The utilization of PJP in ROKC cases offers a range of potential benefits. Firstly, it restores mandibular continuity, facilitating improved masticatory efficiency and oral competence. Secondly, PJP contributes to the reestablishment of facial symmetry, positively impacting patients' aesthetic and psychological well-being. Thirdly, it allows patients to regain a semblance of normalcy in their daily lives, enhancing their overall quality of life. Furthermore, the development of minimally invasive techniques and advancements in biomaterials has contributed to enhancing PJP outcomes and reducing complications.
Case Report
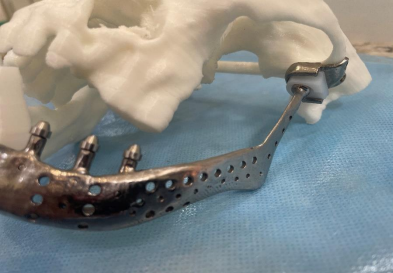
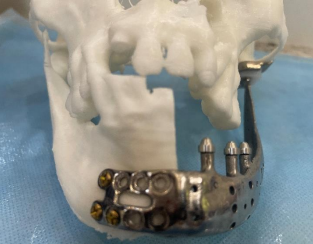
A patient reported to the OPD of Department of Oral and Maxillofacial surgery at Sree Balaji Dental College and Hospital, Chennai. The patient had a previous history of OKC operated back in 2012. She was also a known diabetic and was under medications for thyroid for the past 5 years. On examination there was a extra oral fistula with purulent pus discharge and multi-locular radiolucency in the subcondylar and condylar region indicating recurrent OKC and infection of the plate. Routine blood investigations were done and fitness was obtained under ASA 3. Keeping in mind the systemic co-morbidities, a hemi-mandibulectomy followed by a custom partial joint prosthesis was planned. The custom prosthesis was planned to restore the facial symmetry and functionality using 3 implant abutments for future dental rehabilitation. The patient recovery took about 1 week and passive mouth excercises began on the 5th day of the surgery. After 1 month of surgery the active mouth opening was found to be 33 mm which is almost satisfactory.
Figure 1
Figure 2
Figure 3
Discussion
The utilization of partial joint prosthesis (PJP) following hemi-mandibulectomy in cases of recurrent odontogenic keratocyst (ROKC) represents a significant advancement in the field of maxillofacial reconstruction. ROKC is known for its aggressive nature and high recurrence rates, often necessitating extensive surgical interventions such as hemi-mandibulectomy to ensure complete removal. However, such radical resections result in substantial loss of mandibular bone, leading to functional and aesthetic challenges for the patient. The integration of PJP addresses these challenges by providing a comprehensive solution that focuses on restoring both form and function.
PJP offers a tailored approach to post-hemi-mandibulectomy reconstruction. The prosthetic joint components, which replicate the anatomical structure of the temporomandibular joint, allow for proper mandibular movement and articulation. This is crucial in restoring masticatory function, speech, and overall oral competence that are compromised due to extensive bone loss. Additionally, PJP aids in the reestablishment of facial symmetry, contributing significantly to the patient's psychological well-being and self-esteem.
The success of PJP implementation in ROKC cases following hemi-mandibulectomy relies on several factors. Comprehensive preoperative evaluation, including detailed imaging and assessment of occlusion, is essential to customize the prosthesis according to the patient's specific anatomy. Surgical precision during prosthesis placement is paramount to achieve optimal alignment and stability. Furthermore, advancements in biomaterials and minimally invasive surgical techniques have further improved outcomes, reducing the risk of complications and enhancing patient recovery.
However, challenges persist in PJP usage, including the potential for infection, prosthesis-related complications, and the need for long-term follow-up. Patient selection and thorough consideration of their overall health status are crucial to minimize these risks. Additionally, the long-term durability and functional outcomes of PJP in ROKC cases warrant continued research and clinical studies.
Conclusion
In conclusion, the integration of partial joint prosthesis following hemi-mandibulectomy in cases of recurrent odontogenic keratocyst presents a promising avenue for addressing the functional and aesthetic challenges associated with extensive bone loss. This approach offers patients a chance to regain not only their masticatory function but also their confidence and overall quality of life. As the field of maxillofacial reconstruction continues to evolve, further research and collaboration between surgical and prosthetic disciplines will contribute to refining PJP techniques and improving patient outcomes.
Conflict of interest: There was no conflict of interest.
Consent: Both Informed and written consent were taken.
References
1.Lin, H., Zhong, X., Zhou, N. et al. Mandibular reconstruction after excision of recurrent odontogenic keratocyst using a novel mandibular distraction osteogenesis method– a case report. Head Face Med 19, 21 (2023). https://doi.org/10.1186/s13005-023-00367-0
2.Titinchi F. Novel recurrence risk stratification of odontogenic keratocysts: a systematic review. Oral Dis. 2021. https://doi.org/10.1111/odi.13931. Article PubMed Google Scholar
3.Nanjappa M, Natashekara M, Sendil Kumar C, Kumaraswamy SV, Keerthi R, Ashwin DP, Gopinath AL. “Transport distraction osteogenesis for reconstruction of mandibular defects”: our experience. J Maxillofac Oral Surg. 2011;10:93–100. https://doi.org/10.1007/s12663-011-0190-4.
Article PubMed PubMed Central Google Scholar
4.Neelakandan RS, Bhargava D. Transport distraction osteogenesis for maxillomandibular reconstruction: current concepts and applications. J Maxillofac Oral Surg. 2012;11:291–9. https://doi.org/10.1007/s12663-011-0329-3. Article CAS PubMed Google Scholar
5.Balaji SM. Total reconstruction of mandible by transport distraction after complete resection for benign and malignant tumors. Indian J Dent Res. 2016;27:205–12. https://doi.org/10.4103/0970-9290.183121.Article CAS PubMed Google Scholar
6.Li T, Man Y, Bi R, Jiang N, Li Y, Zhu S. Reconstruction of mandibular segmental detects using transport disk distraction osteogenesis. J Craniofac Surg. 2017;28:2088–92. https://doi.org/10.1097/SCS.0000000000004167.Article PubMed Google Scholar
7.Castro-Núñez J, González MD. Maxillary reconstruction with bone transport distraction and implants after partial maxillectomy. J Oral Maxillofac Surg. 2013;71:e137–42. https://doi.org/10.1016/j.joms.2012.08.030.Article PubMed Google Scholar
8.Warburton G, Shihabi A, Ord RA. Keratocystic Odontogenic Tumor (KCOT/OKC)-Clinical Guidelines for Resection. J Maxillofac Oral Surg. 2015;14:558–64. https://doi.org/10.1007/s12663-014-0732-7.Article PubMed PubMed Central Google Scholar
9.Fidele NB, Bing L, Sun Y, Wu T, Zheng Y, Zhao Y. Management of mandibular odontogenic keratocyst through radical resection: report of 35 cases. Oncol Lett. 2019;18:733–41. https://doi.org/10.3892/ol.2019.10367.Article PubMed PubMed Central Google Scholar
10.Al-Moraissi EA, Dahan AA, Alwadeai MS, Oginni FO, Al-Jamali JM, Alkhutari AS, et al. What surgical treatment has the lowest recurrence rate following the management of keratocystic odontogenic tumor?: a large systematic review and meta-analysis. J Craniomaxillofac Surg. 2017;45:131–44. https://doi.org/10.1016/j.jcms.2016.10.013.Article PubMed Google Scholar
11.Kolokythas A, Fernandes RP, Pazoki A, Ord RA. Odontogenic keratocyst: to decompress or not to decompress? A comparative study of decompression and enucleation versus resection/peripheral ostectomy. J Oral Maxillofac Surg. 2007;65:640–4