Cognizance of Emergency Contraception, is it Enough?
Cognizance of Emergency Contraception, is it Enough?
Shailja Verma *1, Sheila Radhakrishnan 1
1. Specialty Doctor, Royal Free Hospital, London, U.K.
2. Consultant, Royal Free Hospital, London, U.K.
*Correspondence to: Shailja Verma, Specialty Doctor, Royal Free Hospital, London, U.K.
Copyright
© 2023 Shailja Verma. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 22 August 2023
Published: 08 September 2023
DOI: https://doi.org/10.5281/zenodo.12075879
Abstract
Objective
Emergency contraception cognizance in women presenting for termination of pregnancy in a teaching hospital.
Study design
Prospective study of 157 women presenting at the Community gynecology department of Royal Free Hospital, UK, over ten months period (June 2019 to March 2020).
Result
- Overall, fifteen percent of women were completely unaware of emergency contraception.
- Out of 133 women who were aware of these methods, less than one-sixth used emergency contraception (EC) to prevent current unwanted pregnancy.
- Most women used oral EC (Levonelle) as their choice of EC. But reason of failure of EC was its use during mid-cycle, possibly post ovulation, despite being taken within 72 hours of unprotected sex.
- Around two-thirds of women were not using any ongoing contraception at the time of presentation to the TOP clinic. Twenty-five per cent used condoms for contraception.
Conclusion
There is a need to educate women on contraceptive options available at every opportunity, including information on emergency contraception and how it can be accessed.
Also, women accessing any services for emergency contraception should be correctly assessed and offered complete information on different methods available to them, including copper coil insertion.
Keywords: Emergency contraception, abortion, awareness, termination of pregnancy.
Cognizance of Emergency Contraception, is it Enough?
Introduction
Women make up half of England’s population.[1] Of these, almost three-quarters at any one time want to either prevent [1] or achieve pregnancy, and therefore contraception is a practical population approach to meet these needs. 12 % of these women are using no contraception at any one time. 6 out of 10 women reach out to the GPs, making them the most popular source, followed by sexual health and community clinics, particularly younger and more disadvantaged populations. The remaining women who cannot reach existing contraceptive services end up receiving opportunistic contraceptive advice, like after taking emergency hormonal contraception (EHC), having an abortion or a baby, or when they are in contact with health services for other issues or conditions.[1]
Emergency contraception (EC), both oral and intrauterine methods, owns a unique position amongst contraceptives in that it can be used after sex to prevent pregnancy.[2] Access to oral EC has changed dramatically in the UK in the last 15 years.[3] Significant changes were facilitated by developing a progestogen-only formulation containing levonorgestrel, which is safe to use and has no significant contraindications. Consequently, the levonorgestrel formulation was deregulated and became available over the counter (OTC) from pharmacies without a prescription in the UK in 2001. Furthermore 2009, ulipristal acetate, a selective progesterone receptor modulator, was licensed for EC use. Its efficacy was demonstrated up to 120 hours after unprotected sexual intercourse or contraceptive failure.[4] However, it became accessible only on prescription in the UK from April 2015.[5] Emergency copper intrauterine devices continue to be available free at the point of access through community family planning and general practice clinics, and although significantly more reliable compared with pills,[6] are less accessible as they require insertion by a healthcare practitioner, with same day insertion being an additional challenge.
As per the government's Sexual Health Framework, around 50% of all our pregnancies are unplanned. The Framework also concludes that "emergency contraception is a safe & an effective way of preventing unwanted pregnancy when regularly used methods have failed or have not been used."[7] One of the studies done in Scotland on unintended pregnancy and contraceptive use showed that under 12% of women attending for abortion had used EHC.[8] EHC has been available free of charge from pharmacies in Scotland from the end of 2008, and a small decrease in abortions has been observed there.[9]
Women presenting for EHC indicate that they do not wish to become pregnant and this is despite being at risk of pregnancy following unprotected sexual intercourse (UPSI). They are a population that presents into the healthcare system at risk of having an unintended pregnancy that could be avoided.[10] In this article, we wish to study the awareness of emergency contraception amongst women presenting at the termination of pregnancy clinic in a teaching hospital in northwest London. We want to establish the importance of proper education and assessment, which goes a long way in the success of emergency contraception as a backup option to prevent unintended pregnancy.
Study Design
From June 2019 to March 2020, we recorded 210 requests for termination of pregnancy. A considerable proportion is high-risk cases with underlying medical comorbidities. Besides routinely offering them essential STI screening and treatment, ultrasound scan assessment, baseline blood investigations, and contraceptive advice are also provided.
It is a retrospective study. Data collection involved reviewing all patient notes in the study period and screening them individually for documentation on emergency contraception. Ethical committee approval was not sought for this study. Questions like the inquiry of awareness of emergency contraception, use of EC, type of EC used, period, and wherein the menstrual cycle woman when she used it were included in this study.
During our routine consultation, we educate women (including one with a language barrier) on different forms of EC available, how they can access them and what to expect. We also provided leaflets on EC and invited them for further discussion in our family planning clinic for contraceptive choices.
Throughout the service provision, women can opt out of any consultation component freely; some might decide otherwise and continue with the pregnancy, so they self-refer to GP and get booked for antenatal care. A few of them might need a referral to an emergency gynaecology unit for pregnancy of unknown location (PUL), suspected ectopic pregnancy, or miscarriage; very few might choose an alternate service based on their need and convenience. However, most of our women went ahead with the termination. During the study period, we included 157 out of 210 women coming to us as the remaining did not continue with the services for one of the above reasons.
Results
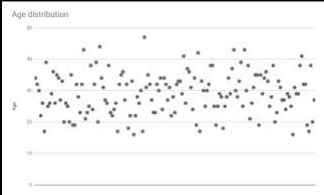
The age distribution pattern of women presenting for TOP shows 85.4 % of them belong to the 20-40 years age-group, 8.9 % are teenage pregnancies and approx. 5% are more than 40 years age-group.
Figure 1
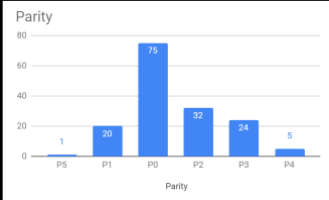
In regards to parity, nearly half of the women were nulliparous (47.8 %). The remaining was with parity of two or more (39.5 %), including grand multipara (more than 4).
Figure 2
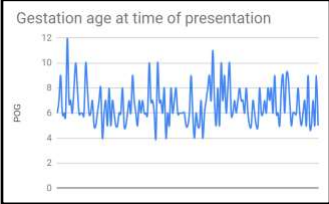
Gestation age distribution at presentation to the clinic was predominately between six to 10 weeks (73.9 %). One-fifth were less than six weeks at first presentation, including about four weeks pregnant. Five per cent of them were beyond ten weeks of gestation at the presentation time.
Figure 3
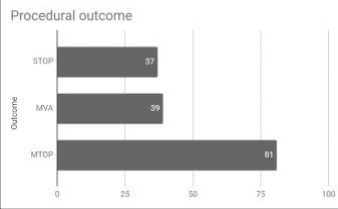
Eighty-one women opted for medical TOP, making it the most common choice amongst women presenting to our clinic. The surgical option was used in seventy-six women, with manual vacuum aspiration slightly more preferred than surgical TOP under general anaesthesia (thirty-nine verses thirty-seven cases).
Figure 4
Around two-thirds of women were not using any ongoing contraception at the time of presentation to the TOP clinic. Of the remaining one-third, twenty-five per cent used condoms for contraception, others used pills and patches, and one had an implant.
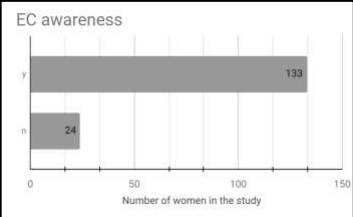
Regarding EC use, approximately fifteen per cent of these women were utterly unaware of emergency contraception, although most were aware.
Figure 5
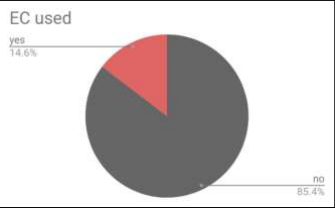
Out of 133 aware women, less than one-sixth only made use of emergency contraception (EC). Most of the others who did not use EC were not expecting to get pregnant and did not think of using it.
Figure 6
Oral EC (Levonelle) was the preferred choice, and in almost all cases, it was used during their mid-cycle, i.e., after ovulation; hence, oral EC failed to prevent unwanted pregnancy.
Discussion
Most women presenting to our services were not using any form of contraception at the time of presentation. Barrier contraception has been the common contraceptive choice in the remaining women, and very few relied on pills and patches. In addition, most abortion seekers were young adults between 20 to 40, as expected and presented in the first trimester. Thus, our EC users are no different from abortion seekers with a similar demographic profile.
None of our EC users are in the above 40 y age group, but also, they make up only 5 % of the population profile in this study. Similarly, amongst teenagers, making up 9% of our cases in this study, only one managed to use emergency contraception.
Oral EC was the only method used as most of them availed of this service from local pharmacies. As they presented for termination of pregnancy service, we retrospectively enquired on the timings of taking the EC pill to look for the cause of medication failure. In almost all our cases, women remembered taking the EC pill somewhere during their mid-cycle. Therefore, the possibility of them already ovulating despite taking EC within 24-48 hours of UPSI is highly likely. We noticed a lack of appropriate discussion and evaluation as to the best choice of emergency contraception, probably at the time of offering EC, and this was further obvious as most of them were completely unaware of the Copper coil as an option. On this occasion, they were educated more about the mechanism of action for different forms of EC and the leaflets provided.
Our more striking result was that approximately 84 % of abortion seekers were aware of EC, but only very few used it. It might be the unawareness of the risk of pregnancy that led to this unwanted outcome.
As we provide a hospital-based TOP service, we predominantly get referrals to specialist services from BPAS (British Pregnancy Advisory Services), which involves women with medical comorbidities. Around 10 of our cases had underlying cardiovascular conditions varying from open-heart surgery for congenital heart disease, supraventricular tachycardia undergoing ablation surgery, mechanical heart valve on warfarin, hypertension, and recent pulmonary embolism. The most commonly noted was asthma, seen in 14 cases varying from mild to severe. The other 10 cases had endocrinological problems like Type 1 or 2 diabetes mellitus, thyroid abnormalities, or autoimmune problems like Crohn’s disease or rheumatoid arthritis.
We even encountered rare conditions like congenital mal-rotation of the gut (surgically corrected), Inherited plasminogen deficiency, Ehler-Danlos syndrome, and a few others. It is quite possible that owing to the flooding of medications and care they received already, contraception gets completely missed and leads to unintended pregnancies.
Owing to the multidisciplinary care provided to our cases, we could offer medical TOP to most of these high-risk cases, and the remaining were managed predominantly using MVA (manual vacuum aspiration). However, approximately one-fifth of our cases were managed with surgical TOP, mainly due to patient preference or advanced gestation.
Our services also offer STI screen, women’s health counselling, and family planning clinics. We see the importance of offering holistic care to these patients and keeping hospital-based SRH services intact and running. The primary outcome of our study is that the recognition of the need for EC by the patients seeking an abortion is strikingly deficient, despite reasonable awareness of this method. Another aspect is that gaining information from reliable sources (education, healthcare providers, and media campaigns) was an essential factor in promoting good knowledge about the management of EC use.
Conclusion
The onus lies not in one hand but has to be a combined effort coming from all directions to make contraception service provision effective, accessible, and accurate for women. In addition, awareness of emergency contraception needs improvement by highlighting through various channels like media, talks, leaflets and opportunistic discussions.
Future studies can be done with involvement of EC providers in an area and establishing a referral pathway for copper coil insertion for EC. Also, a web-based app can be used by women to understand their need for EC and locations of how it can be quickly and safely accessed.
We also need to study whether there is any change in this number during the COVID situation and its different impacts on emergency contraception awareness.
References
1.Public Health England Health Matters: Reproductive Health and pregnancy planning. 2023 [2023, Aug 26]. Available from: https://www.gov.uk/government/publications/health-matters-reproductive-health-and-pregnancy-planning/health-matters-reproductive-health-and-pregnancy-planning
2. Cleland K, Zhu H, Goldstuck N, Cheng L, Trussell J. The efficacy of intrauterine devices for emergency contraception: a systematic review of 35 years of experience. Human Reproduction 2012;27(7):1994–2000.
3. Schenk KD. Emergency contraception: lessons learned from the UKBMJ Sexual & Reproductive Health 2003;29:35-40.
4. British National Formulary (BNF). Joint Formulary Committee, British National Formulary. 2013, London: BMJ Group, RCPCH Publications Ltd and the Royal Pharmaceutical Society of Great Britain.
5. Black, KI, Geary, R, French, R, Leefe, N, Mercer, CH, Glasier, A, Macdowall, W, Gibson, L, Datta, J, Palmer, M, Wellings, K. Trends in the use of emergency contraception in Britain: evidence from the second and third National Surveys of Sexual Attitudes and Lifestyles. BJOG 2016; 123: 1600– 1607.
6. Wu S, Godfrey EM, Wojdyla D, et al. Copper T380A intrauterine device for emergency contraception: a prospective, multicentre, cohort clinical trial. BJOG 2010;117(10):1205?1210.
7. Department of Health. A framework for sexual health improvement in England. 2013
8. Lakha F, Glasier A. Unintended pregnancy and use of emergency contraception among a large cohort of women attending for antenatal care or abortion in Scotland. Lancet 2006;368:1782–7
9. Glasier A. Emergency contraception: clinical outcomes. Contraception 2013;87:309–13
10. Thomas CM, Cameron S. Can we reduce costs and prevent more unintended pregnancies? A cost of illness and cost-effectiveness study comparing two methods of EHC. BMJ Open 2013;3:e003815.