Correlation between Body Mass Index and Intraocular Pressure in North Indian Population
Correlation between Body Mass Index and Intraocular Pressure in North Indian Population
Fareha Husain*1 Mohd Aslam2 Sangeeta Singhal3 Abdul Waris4
1.Senior Resident;
2,3.Professor, Department of Physiology, JNMC, AMU, Aligarh
4.Associate Professor, Department of Ophthalmology, JNMC, AMU, Aligarh.
*Correspondence to: Fareha Husain, Senior Resident.
Copyright
© 2023 Fareha Husain. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 06 September 2023
Published: 13 September 2023
Correlation between Body Mass Index and Intraocular Pressure in North Indian Population
Introduction
The pressure inside the eye which is known as Intraocular pressure is the result of difference between the rate of aqueous production inside the eye and rate of aqueous outflow (Kanski’s clinical ophthalmology, 8th edition1). The normal range of intraocular pressure is between ten to twenty-one mmHg (Hashemi Het al., 20052, Pooranee, 9 Oct 20153). The intraocular pressure may fluctuate up to +/- 3.5 mmHg for twenty-four hours cycle and it is known as diurnal variation. It is very important to know the risk factors that can affect the level of intraocular pressure because increased intraocular pressure may lead to ocular hypertension and Glaucoma. Numerous studies concluded that obesity is an independent risk factor for increased intraocular pressure and there is a positive relationship with intraocular pressure (Gherghel et al., 20014, Kohli et al., 20145, Baisakhiya et al., 20156). Body mass index (BMI) could be a factor that can affect intraocular pressure.
Body mass index (BMI)- It is calculated by dividing the person’s weight in kilograms by the square of his height in meters (kg/m2) (WHO 20207).
The International Classification of Adult underweight, overweight, and obese according to BMI
Classification of Body Mass Index
- Obese person is defined with a body mass index of 30 or more (WHO definition of obesity 20207).
- Obesity is associated with numerous ocular diseases such as decreased visual acuity (Bergman et al., 20048), cataract (Caulfield et al., 19999, Oster PJ et al., 200310, Glynn RJ et al., 199511, Jacques et al., 200312, Klein BE et al ., 200113), age-related maculopathy (Schaumbarg DA et al., 200114, Seddon JM et al., 200315), diabetic retinopathy (Ballard DJ et al., 198616, Caturvedi Net al., 200117, Henricsson M et al., 200318, Klein r et al., 198419, Schoenfeld ER et al., 199320, Van leiden HA et al., 200221) and glaucoma (Gasser P et al., 199922, Leske MC et al., 199523, Zang EA et al., 199424).
- The relationship has been reported between obesity and ocular diseases such as cataract, glaucoma, and age-related macular degeneration.
- According to many studies the intraocular pressure is affected by obesity, but an exact scientific correlation has yet to be determined (Hyung-Deok Jang et al., 201425, Mori K et al., 200026).
- Obesity results in increased intra orbital adipose tissue causing increased episcleral pressure. This leads to decreased drainage of the aqueous humour (Nyamdorj R et al., 200827).
- Various studies have shown that obesity is an independent risk factor for increased intraocular pressure and there is a positive relationship with intraocular pressure (Gherghel et al., 20014, Kohli et al., 20145, Baisakhiya et al., 20156).
This study is aimed to establish a relationship between intraocular pressure (IOP) and body mass index (BMI). Some studies have been done to corelate BMI with raised IOP, and we want to further enhance those findings.
Material and Methods:
Inclusion Criteria: Informed consent, both male and female, Age 30 to 70 years.
Exclusion Criteria: Subjects <30 and >70 years, known case of ocular hypertension and glaucoma, patients on medication affecting IOP, ocular disease affecting normal corneal thickness, patients with diabetic and hypertensive.
BMI Measurement by Bodystat 1500 MDD-- It provides a fast and effective measurement body composition using modern technology that is ideal for use in clinical settings. Bodystat works on principle of Bio-Electrical Impedance Analysis, which provides complete body analysis of body fat, lean weight, optimal total body weight range and body water level. All results are instantly displayed on the liquid crystal display (LCD) screen.
1.Pre-requisite for the examination:
- NO eating or drinking 4 to 5 hours prior to the test.
- NO exercise 12 hours prior to the test.
- NO alcohol or caffeine consumption 24 hours prior to the test.
- Relaxed and cooperative subject.
- Proper posture.
- Two main cable leads of the instrument (each lead is to be inserted to the connectors at the rear of the unit.
- Self- adhesive disposable electrodes.
2.SUBJECT POSITION- After removing shoes and socks, subject was made to lie down flat with the arms and legs spread slightly. The self-adhesive disposable electrodes were attached to RIGHT hand and RIGHT foot. Bodystat 1500 has two sets of main leads which are then divided into a RED and a BLACK lead. The RED leads are connected to the electrodes just behind the finger and toe. The BLACK (measuring) leads are then connected to the electrodes on the right wrist and right ankle.
Switched BODYSTAT 1500MDD unit on, entered the subject data like gender, age, height, weight, and activity level, then connected the unit with all the four surface electrodes with the subject being in supine position, after that results were read from LCD monitor.
Intraocula Pressure Measurement--by Air Puff Non-Contact Tonopachy Nidek NT-530 P
To measure corneal thickness corrected intraocular pressure we used Tonopachy NT-530 P which is a combination of non-contact tonometer and pachymeter. It quickly and accurately measures the intraocular pressure using auto tracking and auto shot technology.
During IOP measurement was performed in sitting and relaxed position as explained to subjects. The subjects chin and forehead fixed on the tonometer bracket and instructed to look at the light source in the lens. To have good corneal exposure subjects were instructed to keep both eyes open naturally without squeezing. IOP was measured for each eye separately three times and the mean value was taken. All measurements were made in the order of right eye first and then left eye.
Results:
120 normal subjects were taken, both male and female were included in the study. Among them 60 were males and 60 were females. Mean age of males is 48.22 and mean age of female is 45.97. All subjects were married. Subjects were compared for IOP between different BMI groups.
Table 1: Age group and gender classification
|
AGE GROUP |
MALE |
FEMALE |
TOTAL |
|
31-40 |
18 |
23 |
41 |
|
41-50 |
16 |
18 |
34 |
|
51-60 |
20 |
14 |
34 |
|
61-70 |
6 |
5 |
11 |
|
TOTAL |
60 |
60 |
120 |
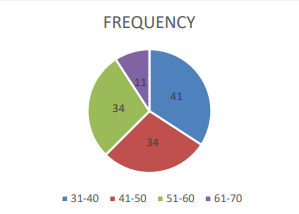
Subjects are aged between 30-70 years, out of these 18 males and 23 females are coming in age group of 31-40. In next age group 41-50 there are total 34 subjects, 16 are males and 18 females, in next age group 51-60 there are total 34 subjects and among them 20 males and 14 females. In last age group 61-70, there are total 11 subjects and among them 6 are males and 5 are females.
Figure 1: Showing Frequency Of Different Age Groups
Table 2: Comparison of mean age of male and female.
|
GENDER |
MEAN |
Sd ± |
|
MALE |
48.22 |
10.35 |
|
FEMALE |
45.97 |
9.42 |
|
TOTAL |
47.09 |
9.92 |
Subjects are selected between 30-70 years of age. Mean age of total subjects is 47.09 ± 9.92. Mean age of male subjects is 48.22 ± 10.35 and mean age of female subjects is 45.97 ± 9. 42 years.
Figure 2: Gender Distribution In Subjects
Table 3: Marital status of Subjects
|
|
MARRIED |
UNMARRIED |
|
MARITAL STATUS |
120 |
0 |
Among study group of 120 subjects all are married
Table 4: Number of subjects under different BMI grade
|
BMI grade |
Number |
|
Underweight (<18.5) |
8 |
|
Normal (18.5-22.9) |
22 |
|
Overweight (23-24.9) |
13 |
|
Obese class I (25- 29.9) |
65 |
|
Obese class II (>30) |
12 |
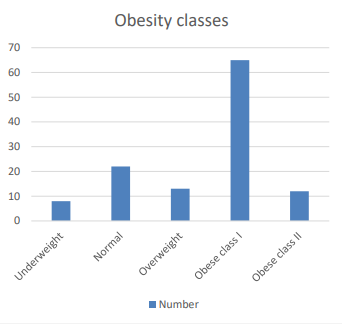
Obesity of the subjects was evaluated by BMI grading. Among 120 subjects’ maximum number of subjects (65) are of BMI between 25 to 29.9 i.e., class I obesity and least number of subjects (8) are of BMI <18.5 i.e., underweight. 22 subjects belong to normal BMI between 18.5 to 22.9. 13 subjects belong to overweight category BMI between 23 to 24.9. While12 subjects belong to class II obesity with BMI >30.
Figure 3: Bar-Chart Showing Obesity Classes
Table 5: BODY MASS INDEX
|
|
BMI |
|
MEAN |
25.57 |
|
STDEV |
4.31 |
|
MINIMUM |
16.50 |
|
MAXIMUM |
40.30 |
BMI was taken with the help of Bodystat -1500MDD. Mean of BMI is 25.57 ± 4.31. In our subjects BMI ranges between 16.50 to 40.30. Normal BMI between 18.5 to 22.9 kg/m2, Overweight BMI between 23.0–24.9 kg/m2, Obesity BMI ≥ 25.0 kg/m2
Table 6: Mean IOP of Right and Left eye
|
|
IOP (R) |
IOP (L) |
|
MEAN |
15.30 |
15.08 |
|
Sd ± |
2.99 |
2.61 |
Intraocular pressure was recorded by using Air Puff Non-Contact Tonopachy Nidek NT-530 in both eyes. Mean IOP of right eye is 15.30 ± 2.99 and Mean IOP of left eye is 15.08 ± 2.61 mmHg. IOP ranges between 10-21 mm Hg with a mean 15- or 16-mm Hg ± 3.5 mm Hg.
Table 7: CORRELATION between IOP and BMI
|
|
IOP (R) |
IOP (L) |
|
BMI |
Significant (r = 0.49) |
Significant (r = 0.46) |
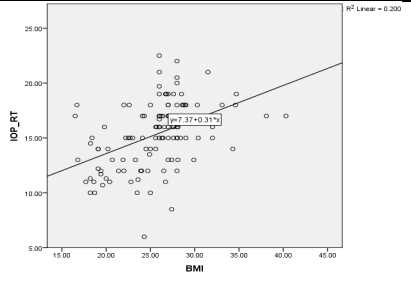
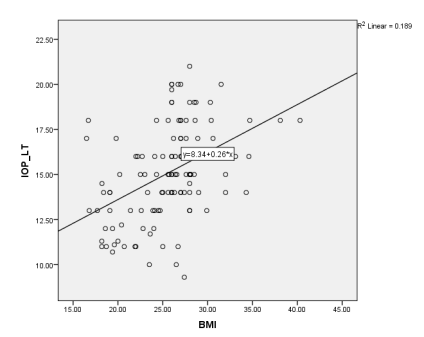
Correlation between BMI and IOP on both sides was done by Spearman correlation test. There is significant correlation between the IOP and BMI.
Figure 4: Showing Correlation between IOP right eye and BMI
Figure 5: Showing Correlation between IOP left eye and BMI.
Discussion:
Our study was completed over a period of 2 years and compared intraocular pressure (IOP) in men and women with respect to their body mass index (BMI). This study shows a positive association between BMI and IOP. In this study the mean IOP of right eye is 15.30 and mean IOP of left eye is 15.08. This study includes North-Indian subjects from, in and around Aligarh Uttar Pradesh, both males and females between the age group 30-70 years. In our study IOP increase is directly related to increase in body mass index.
BMI grading was done for all subjects included in our study and maximum number i.e., 65 out of 120 are in class I obesity with BMI between 25 to 29.9 and least number of subjects (8) are underweighted with BMI < 18.5. There are 22 subjects with normal BMI between 1.5 to 22.9. In overweight category, there are 13 subjects with BMI between 23 to 24.9, there are 12 subjects in class II obesity with BMI >30. The mean BMI in our study is 25.57 ± 4.31 kg/m 2.
In this study the Spearman correlation test shows a significant positive correlation between body mass index (BMI) and intraocular pressure (IOP) of right eye (r = 0.49) and left eye (r = 0.46).
Our study results are consistent with some previous studies showing a statistically significant positive correlation between body mass index and intraocular pressure. According to Adelola O etal.,28 increased body weight, BMI, and neck circumference are associated with increased intraocular pressure, which is a risk factor for glaucoma. 2022 Louisraj S et al., 201829 showed that in both sex increased BMI was positively associated with higher IOP and they said that BMI and IOP are definitely related, Di Zhao et al., 201630 did study to know the associations of change in adiposity markers such as body mass index (BMI), waist circumference, and percent fat mass with change in intraocular pressure (IOP) in Korean subjects and found positive association of adiposity with intraocular pressure.
George GO et al., 201531 showed a significant positive relationship (p<0.001) between body mass index and intra-ocular pressure. Huma Zainab et al., 201432 conducted a cross-sectional comparative study to determine the relationship of intraocular pressure (IOP) with body mass index (BMI) and found a positive relationship. Mehak Mufti et al., 201933 showed a strong positive relationship between intraocular pressure and body mass index.
In study on Korean people Ja Kyun Lee et al., (2009)34 analyzed the relationship between intraocular pressure (IOP) and health parameters like body mass index. In another study Mori K et al., 200026 showed that obesity measured by body mass index was associated with increased intraocular pressure.
The proposed mechanism of elevated intraocular pressure is due to increased intra orbital fat mass which causes elevated episcleral venous pressure that leads to decreased aqueous outflow facility. Obesity also increases blood viscosity and due to sluggish outflow, there is increased outflow resistance, that cause increase in intraocular pressure. The excessive orbital fatty tissue causes decrease in aqueous humor outflow facility due to increased resistance on episcleral veins and ultimately increasing intraocular pressure (Z. Onaran et al., 201435).
Multicentric studies with larger number of subjects maybe needed to further support our findings that body mass index (BMI) could be a parameter to assess the risk of increased intraocular pressure and glaucoma.
Conclusion
Body mass index (BMI) is directly corelated to intra-ocular pressure in both eyes. So, by early detection and managing of increase in BMI we can control increasing intraocular pressure of eyes which is a very important risk factor for glaucoma. It could be used in the early screening of glaucoma. We can advise general population to keep BMI under normal limits, which will be helpful to stop rise in intra-ocular pressure (IOP) of eyes.
References
1.Kanski's Clinical Ophthalmology 8th-2016.
2. Hashemi H, Kashi AH, Fotouhi A, Mohammad K (June 2005). "Distribution of intraocular pressure in healthy Iranian individuals: the Tehran Eye Study". BrJOphthalmol. 89 (6):6527. doi:10.1136/bjo.2004.058057. PMC 1772663. PMID 15923494.
3. Pooranee 9 October 2015. "Do you know about Intra Ocular Pressure?". Health Education Bureau, Information and Communication Technology Agency, Sri Lanka. Retrieved 4 November 2015.
4. Gherghel D, Orgul S, Gugleta K, Flammer J. Retrobulbar blood flow in glaucoma patients with nocturnal over-dipping in systemic blood pressure. Am J Ophthalmol.2001,132, 641-7
5. Kohli PG, Kaur H, Maimi S. Relation of body mass index with intraocular pressure. Indian J of Basic and Applied Medical Research , 2014;3:679-81
6. BaiSakhiya S, Surjit Singh, Prafulla Manjhi. Journal of Clinical and Diagnostic Research. 2016 Dec, Vol-10(12): CC05-CC08 www.jcdr.net
7. World Health Organization (2000). Technical report series 894: Obesity: Preventing and managing the global epidemic (PDF). Geneva: World Health Organization. ISBN 978-92-4-120894-9
8. Bergman B, Nilsson-Ehle H, Sjöstrand J. Ocular changes, risk markers for eye disorders and effects of cataract surgery in elderly people: a study of an urban Swedish population followed from 70 to 97 years of age. Acta Ophthalmol Scand. 2004; 82:166–74.
9. Caulfield LE, West SK, Barrón Y, et al. Anthropometric status, and cataract: the Salisbury Eye Evaluation project. Am J Clin Nutr. 1999; 69:237–42
10. Oster PJ, Wong TY, Machin D, et al. Risk factors for nuclear, cortical, and posterior subcapsular cataracts in the Chinese population of Singapore: The Tanjong Pagar Survey. Br J Ophthalmol. 2003; 87:1112–20
11. Glynn RJ, Christen WG, Manson JE, Bernheimer J, Hennekens CH Arch Ophthalmol. 1995 Sep; 113(9):1131-7.
12. Jacques PF, Moeller SM, Hankinson SE, et al. Weight status, abdominal adiposity, diabetes, and early age-related lens opacities. Am J Clin Nutr. 2003; 78:400–5
13. Klein BE, Klein R, Lee KE, et al. Measures of obesity and age-related eye diseases. Ophthalmic Epidemiol. 2001; 8:251–62
14. Schaumberg DA, Christen WG, Hankinson SE, et al. Body mass index and the incidence of visually significant age-related maculopathy in men. Arch Ophthalmol. 2001; 119:1259–65
15. Seddon JM, Cote J, Davis N, et al. Progression of age-related macular degeneration: association with body mass index, waist circumference, and waist-hip ratio. Arch Ophthalmol. 2003; 121:785–92
16. Ballard DJ, Melton LJ, Dwyer MS, et al. Risk factors for diabetic retinopathy: a population-based study in Rochester, Minnesota. Diabetes Care. 1986; 9:334–42
17. Chaturvedi N, Sjoelie AK, Porta M, et al. Markers of insulin resistance are strong risk factors for retinopathy incidence in type 1 diabetes. Diabetes Care. 2001; 24:284–9
18. Henricsson M, Nyström L, Blohmé G, et al. The incidence of retinopathy 10 years after diagnosis in young adult people with diabetes: results from the nationwide population-based Diabetes Incidence Study in Sweden (DISS) Diabetes Care. 2003; 26:349–54
19. Klein R, Klein BE, Moss SE, et al. The Wisconsin epidemiologic study of diabetic retinopathy. III. Prevalence and risk of diabetic retinopathy when age at diagnosis is 30 or more years. Arch Ophthalmol. 1984; 102:527–32
20. Schoenfeld ER, Leske MC, Wu SY. Recent epidemiologic studies on nutrition and cataract in India, Italy and the United States. J Am Coll Nutr. 1993; 12:521–6
21. Van Leiden HA, Dekker JM, Moll AC, Nijpels G, Heine RJ, Bouter LM, Stehouwer CD, Polak BC Diabetes Care. 2002 Aug; 25(8):1320-5.
22. Gasser P, Stümpfig D, Schötzau A, Ackermann-Liebrich U, Flammer J J Glaucoma. 1999 Feb; 8(1):8-11.
23. Leske MC, Connell AM, Wu SY, et al. Risk factors for open-angle glaucoma. The Barbados Eye Study. Arch Ophthalmol. 1995; 113:918–24
24. Zang EA, Wynder EL. The association between body mass index and the relative frequencies of diseases in a sample of hospitalized patients. Nutr Cancer. 1994; 21:247–61.
25. Hyung-Deok Jang, Do Hoon Kim, Kyungdo Han, Suk Gyu Ha, Yang Hyun Kim, Jae Woo Kim, show all Pages 1008-1017 | Received 07 Mar 2014, Accepted 05 Oct 2014, Published online: 07 Nov 2014 https://doi.org/10.3109/02713683.2014.975367 CrossMark
26. Mori K, Ando F, Nomura H, Sato Y, Shimokata H. Relationship between intraocular pressure and obesity in japan. Int J Epidemiol. 2000;29(4):661-6.
27. Nyamdorj R, Qiao Q, Soderberg S, Pitakaniemi J , Zimmet P, Shaw J . Alberti G, Nan H, Uusitalo U, Pauvaday V, Chitson P,Tuomilehto J .Comparison of body mass index with waist circumference , waist to hip ratio and waist-to-stature ratio as a predictor of hypertension incidence in Mauritius .J Hypertens . 2008; 26:866-70
28. Adetola Oluwadamilola Feyijimi, Bernice Oluwakemi Adegbehingbe, Adenike O. Adeoye, Chidi Ihemedu, http://www.nigerianjournalofophthalmology.com, October 17, 2022, IP: 156.155.160.169]
29. Louisraj S, Philip Aloysius Thomas, Christadass Arul Nelson Jesudasan DOI: 10.4103/tjosr.tjosr_2018
30. Di Zhao, Myung Hun Kim, Roberto Pastor-Barriuso, Yoosoo Chang, Seungho Ryu , Yiyi Zhang, Sanjay Rampal, Hocheol Shin, Joon Mo Kim, David S. Friedman, Eliseo Guallar, Juhee Cho Published: January 5, 2016 https://doi.org/10.1371/journal.pone.0146057
31. George GO and Ajayi OB, J Clin Exp Ophthalmol 2015, 6:4 DOI: 10.4172/2155-9570.1000461.
32. Huma Zainab, Zamir Iqbal, Mohammad Afzal Naz, Ayyaz Hussain Awan, Mazhar Ishaq Relationship Between Intraocular Pressure and Body Mass Index Pak Armed Forces Med J 2014; 64 (3):391-4
33. Mehak Mufti, Hammad Nasti, Tajali Shora Relationship between intraocular pressure and body mass index, National Journal of Physiology, Pharmacy and Pharmacology (2019)
34. Ja Kyun Lee, MD, Jong Soo Lee, MD, PhD, and Yoon Kyung Kim The Relationship Between Intraocular Pressure and Health Parameters J Korean Ophthalmol Soc. 2009 Jan;50(1):105-112. Korean. Published online Jan 20, 2009. https://doi.org/10.3341/jkos.2009.50.1.105
35. Z. Onaran, O. Konuk, S. O. Oktar, C. Yucel, and M. Unal, “Intraocular pressure lowering effect of orbital decompression is related to increased venous outflow in Graves orbitopathy,” Current eye Research, vol. 39, no. 7, pp. 666–672, 2014.