A Cross-Sectional Study of Secondary Students’ Knowledge and Attitudes towards Eating Disorders
A Cross-Sectional Study of Secondary Students’ Knowledge and Attitudes towards Eating Disorders
Erietta - Christina Arnaoutaki[1], Stelios Bousi1, Ioannis Michopoulos1, Vasiliki Efstathiou1, Ioanna Giannopoulou1
1. Second Department of Psychiatry, Medical School, National and Kapodistrian University of Athens, Attikon University General Hospital, Athens, Greece.
*Correspondence to: Erietta - Christina Arnaoutaki, Second Department of Psychiatry, Medical School, National and Kapodistrian University of Athens, Attikon University General Hospital, Athens, Greece.
Copyright
© 2023 Erietta - Christina Arnaoutaki. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 31 August 2023
Published: 15 September 2023
DOI:https://doi.org/10.5281/zenodo.10101336
Abstract
Background: Due to their substantial health repercussions, eating disorders (EDs), such as anorexia nervosa (AN), bulimia nervosa (BN) and binge eating disorder (BED), pose a significant public health issue. The purpose of our study was to evaluate both adolescents’ understanding of EDs and their attitudes towards peers with an ED, as well as to evaluate their preferred means of help-seeking in case of eating habit concerns.
Methods: Upper secondary students, aged from 15 to 18 years old, in four school settings in Athens were given a vignette presenting an adolescent of unknown gender with symptoms consistent with either an eating disorder (AN, BN, or BED), depression, or Type 1 diabetes (T1D), randomly, during May and June 2021. A questionnaire including a modified version of Illness Perception Questionnaire (IPQ) was given along with the vignette, to assess their knowledge and attitudes towards the presented individual’s disorder. Further questions were employed to evaluate adolescents’ beliefs about peers with an ED and the means they would choose to seek help in case they had an ED or eating habit concerns.
Results: Out of 104 participating adolescents (41,3% males), fifty-nine adolescents were given vignettes reporting ED symptoms (18 AN, 23 BN and 18 BED symptoms) and were able to identify them (66,7% AN, 43,5% BN, 61,1% BED) almost twice as frequently as those who had to identify depression symptoms (30,1%) and three times more frequently than those had to identify T1D (21,1%) symptoms in their vignette. Among the ED vignettes, the described individual was most frequently (57,6%) perceived as a female. Adolescents resulted to neutral toward common stigmatizing beliefs regarding peers with EDs. In case of being concerned about their eating habits, most students would prefer to talk to their parents (49,5%). Only 10% would choose to contact a health professional (psychologist or psychiatrist / child-psychiatrist), while preferred means to access health services resulted to telephone helpline (65,3%). The primary factors preventing them from seeking help would be emotions such as shame (20,2%) and fear of being judged (19,5%).
Conclusions: More adolescents seem to have become familiar with eating disorders and stigmatizing beliefs regarding peers with an ED tend to regress recently, compared with previous data. Yet, more progress is needed to totally eliminate social stigma. Means such as national telephone helplines should be taken into consideration to advise adolescents concerned about their eating habits.
Key words: adolescents, teenagers, secondary students, eating disorders, anorexia, bulimia, binge eating, mental health literacy, knowledge, attitudes, stigma
A Cross-Sectional Study of Secondary Students’ Knowledge and Attitudes towards Eating Disorders
Introduction
Eating disorders (EDs), such as Anorexia Nervosa (AN), Bulimia Nervosa (BN), and Binge eating disorder (BED), comprise a major public health issue due to their severe effects on physical and mental health (Mitchel &Crow, 2006). According to epidemiological research, incidence of EDs peaks among adolescents and young adults, accounting for 40% of total cases in 14 to 19 age group. (Smink, van Hoeken, Hoek, 2012; Micali, Hagberg, Petersen, Treasure, 2013).
Anorexia nervosa (AN) is a condition affecting primarily teenagers and adult young females with a prevalence ranging from 5 to 7% among adolescent females, who are engaged in modeling and dancing, and from 6 to 8% among girls participating in sports, for whom body weight has a significant impact on their performance (Chatzigeorgiou, 2004), while its prevalence in the general population ranges between 0.5 and 1% (Cost, Krantz, Mehler, 2020). The total mortality rate of AN is reported to range from 10 to 20% (Jorm et al., 1997), with the highest rate reported among females aged below 25 years old. (Cost, Krantz, Mehler, 2020). Suicide accounts for about 20% of deaths of affected adolescents, having a 10-fold higher risk of suicide than healthy adolescents (Cost et al., 2020). On the other hand, bulimia nervosa (BN) affects about 10% of adolescents and young adults in total, being more prevalent than AN among that age group (Ponte, 1994) and is 10 times more frequent in females than males (Jorm et al., 1997). Meanwhile, binge eating disorder has an overall estimated prevalence of 1.32% in children and adolescents. BED seems to be as frequent in children and adolescents as anorexia and bulimia nervosa (KJeldbjerg &Clausen, 2021).
The concept of “mental health literacy”, originally used by Jorm et al. (Jorm et al., 1997), refers to someone’s ability to identify that either themselves or others have an eating disorder (Burns& Rapee, 2006). There is often a partial overlap between the meanings of frequently used terms, such as “knowledge”, “attitude” and “belief”. “Knowledge” refers to a broad network of concepts, images and mental capacities featuring human beings. “Beliefs” or “perceptions” are considered a part of knowledge, comprising undisputed personal truths held by every single individual, derived from experiences or imaginations with strong emotional characteristics, proposing that something is right or wrong. (Mc Nicholas et al., 2015). “Attitudes”, on the other hand, originate from the Latin word “aptus”, which means “capable and ready for action”. They comprise a quite permanent combination of “beliefs” and behavioral tendencies towards socially significant groups or objects, providing either positive or negative feelings about a person or an issue (Petrie &Weinman, 1997).
From a review of the literature, we did not find any reports regarding Greek adolescents’ knowledge about EDs or their attitudes towards people with eating disorders and barriers to help-seeking, which comprise crucial data for their early detection and treatment (Burns& Rapee, 2006). The present study comes to remedy this gap by examining Greek adolescents’ knowledge of EDs and views toward peers affected by an ED and to evaluate their preferred help-seeking means when concerned about their eating habits.
Materials and Methods
Our study involved secondary students, aged from 15 to 18 years old attending four different secondary schools in Athens, Greece, between May and June 2021. In Greece, secondary education consists of six classes in total, three middle school classes and three high school classes. Eligible participants for our study, were those enrolled from the third class of middle school to the third class of high school (Table 1). Informed consent forms were priorly obtained by their parents.
In our study, we used five different vignettes, randomly distributed to the students, followed by identical questionnaires, so that each student had to deal with one single vignette (Table 2) (Roehrig, 2009; McNicholas et al., 2015). Each vignette-questionnaire form was labeled with a unique number code to provide anonymity and ensure confidentiality. The forms were filled out in the classroom, in presence of the main study researcher (EC. A.), in approximately 40 minutes.
The vignettes used, were describing a case of an adolescent (unspecified gender) presenting with symptoms of either AN, BN, BED, depression or T1D (5 separate vignette types). A question following the vignette, asked about the disorder described (free response). Many students did not use a diagnostic terminology, but rather described psychological, or social difficulties faced by the individual in the vignette. Coherent approaches provided by the participants, even without using the exact terms, were considered as a correct identification of the disorder.
A modified version of Illness Perception Questionnaire (IPQ) (reliability index: 0,91), based on Leventhal's self-regulatory model, followed then, to assess participants’ attitudes towards the described disorders (Petrie & Weinman, 1997). Each of five vignette types was assessed in the basis of three IPQ subscales (beliefs about the probable timeline of an illness, the degree of personal control an individual has over the illness, and the efficacy of treatment).
Participants were consequently asked to guess the gender of the adolescent in the vignette, in form of multiple choice (boy, girl, or other gender). All participants, independently from the given type of vignette, were asked to report the level of agreement on five statements representing stereotypical/stigmatizing beliefs about people with EDs on a 5-point Likert scale (from strongly disagree to strongly agree). Finally, all participants reported the person they would reach out in case of being concerned about their eating habits (multiple-choice), the means they would prefer to access health services (multiple-choice) and potential factors that would prevent them from seeking help in that case (free response).
The analysis was conducted using IBM SPSS Statistics for Windows, Version 22.0. Armonk, NY. The Kolmogorov-Smirnov criteria was used to test the distributions' normality. The dependability of the derived factors was evaluated using Cronbach alpha internal consistency index. Quantitative differences between the two groups were compared using the parametric Student's t-test. The parametric analysis of variance (ANOVA) test was developed to compare quantitative variables between more than two groups. The Bonferroni adjustment, whose significance threshold is 0.05/k (k = number of comparisons), was employed to compensate for type I error brought on by multiple comparisons. Two qualitative variables were compared to one another using the t-test. The statistical significance was set at 0.05, and the significance levels are two-sided.
Table1:Secondary school class attended by enrolled students
Results
Knowledge of EDs
104 students (43 boys and 61 girls), (mean age 15,6 +/- 1,1 years old) participated in our study. Eighteen students (17,3%) were given the vignette describing AN symptoms, twenty-three (22,1%) dealt with the one with symptoms of BN and eighteen were given the one with symptoms of BED. Twenty-six students (25%) were given the vignette presenting symptoms of depression The rest of nineteen students (18,3%) were given the vignette describing T1D. ED symptoms (AN, BN, BED) were identified almost twice as often as those of depression and almost three times as often as those of T1D (Table 2). Statistical analysis showed that there was a statistically significant difference in the percentage of correctly identifying the individual's disorder in each vignette [χ² (4) = 11.410, p = .022, N = 104].
Table 2 Randomly distributed vignettes describing symptoms of five separate disorders to secondary school students and percentages of participants who correctly identified the disorder described in their given vignette
AN= Anorexia Nervosa, BN= Bulimia Nervosa, BED= Binge Eating Disorder, T1D= Type 1 Diabetes
Perceptions and attitudes towards EDs
The Cronbach's alpha internal consistency indices in the present sample were 0.76 for the subscale assessing the timeline of the illness, 0.75 for the subscale assessing the degree of personal control an individual has over the illness and 0.71 for the subscale assessing the efficacy of treatment.
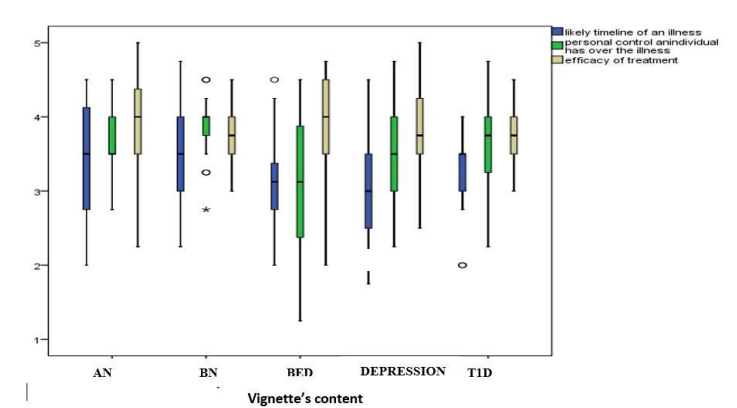
The median values of the subscales according to the content of the vignette are shown in Figure 1. The score regarding the timeline is slightly higher for AN and BN, implying that they are perceived as more chronic conditions, while for the subscale regarding the degree of personal control over the illness, BED has the lowest value. Higher scores for the subscale on treatment effectiveness were observed in BED vignettes without a statistically significant difference. All the above-mentioned observations did not result statistically significant.
Figure 1 Median values of disease perception subscales (timeline – control over the illness – treatment efficacy) for the five vignette disorders according to the IPQ-R answers of the participants
Perceived gender of the vignette’s teenager
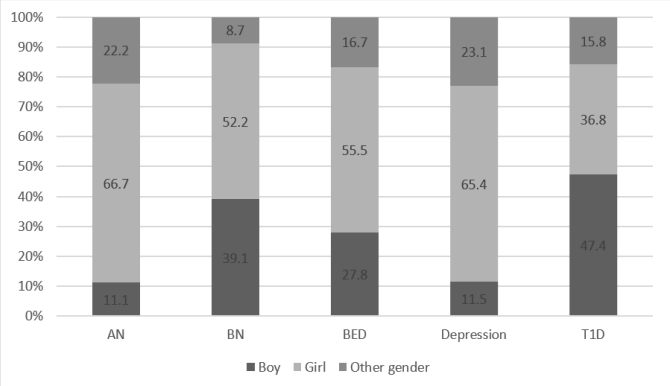
Regarding adolescents’ perception of the vignette individual’s gender, for ED vignettes, most students perceived the individual as a girl Figure 2. There was no statistically significant difference between participants' responses about the gender of the vignette’s individual, x2(7) = 10.832, p =.211, n = 96.
Figure 2 Perception of the vignette individual’s gender for each depicted disorder
Agreement level with common stigmatizing beliefs
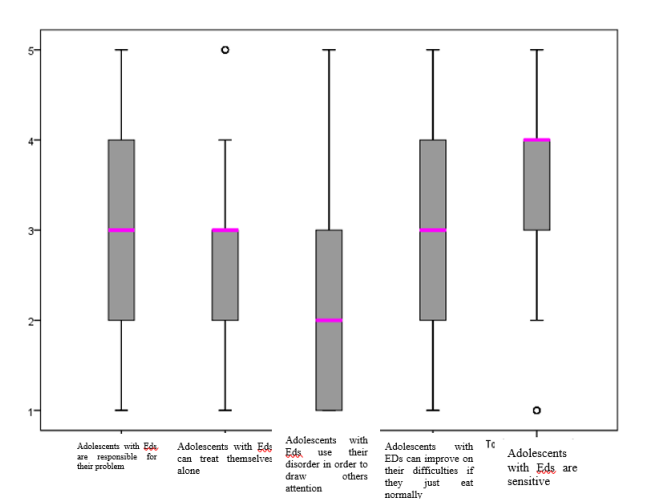
The agreement level on five stereotypical beliefs regarding adolescents having an ED are shown on Figure 3. The median of thee out of the five items range around the midpoint of the scale ("Neither agree nor disagree"). About 50% of the adolescents disagreed with the item "People with EDs use their disorder to get attention from others”, while about 50% agreed with the item "People with EDs are fragile".
Figure 3 Boxplot showing level of agreement with five common beliefs about adolescents with EDs reported on a 5-point Likert score system Median values people with an eating disorder
Help-seeking
Out of 99 students who answered the question ‘Who would you talk to if you were worried about your eating habits’, half of them (49.5%, n=49) would share their concerns with their parents, about a third (32.3%, n=32) with their ‘best friend’ and only a small percentage with a psychologist (7.1%, n=7), a child psychiatrist (3%, n=3) or a teacher (1%, n=1). These results are presented in Table 3.
Table 3 Reported answers on the question regarding the person that adolescents would ask for help in case of an eating disorder
Out of 95 students who responded to the question “How would you prefer to access health services?”, 65.3% (n=62) mentioned the telephone helpline, 26.9% (n=28) the internet / social media, while only 5.3% (n=5) reported that would attempt a meeting with a mental health professional in person (Table 4).
Table 4 Preferred means of help-seeking
Barriers to help-seeking
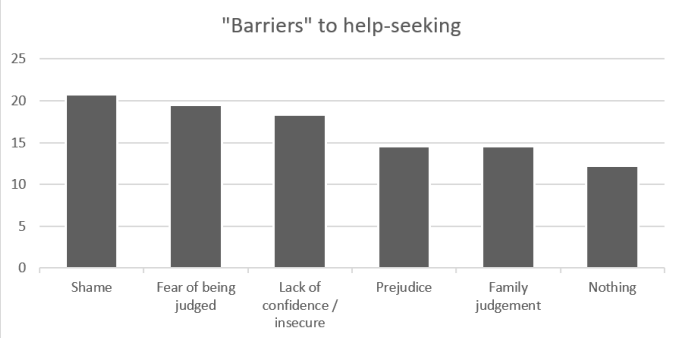
Out of 82 students who responded to the question about what would prevent them from seeking help if they had any concern about their eating habits or an ED, 17 (20.2%) reported shame, 16 (19,5%) fear of being judged, 15 (18,3%) reported lacking self-confidence, 12 (14,6%) prejudice and 12 (14,6%) family judgement. Only ten students (12,2%) reported that nothing would prevent them from seeking help (Figure 3), without statistically significant differences between male and female students.
Figure 4 Responses regarding factors that would prevent adolescents from help-seeking if they had concerns about their eating habits
Discussion
AN and BN symptoms were identified twice as often as those of depression and almost three times as often as those of T1D in our study. This finding comprises a contradiction of the available literature, which claims that there is a very low level of knowledge among adolescents regarding EDs. In a sample of 420 adolescents aged 14-18 years in Italy, only 22.8% seemed to correctly identify AN and BN (Napolitano, Bencivenga, Pompili, Angelillo, 2019). It is worthy to point out that although study participants seemed to understand the vignette’s presented disorder when referring to EDs, they found it difficult to give a specific term, due to lack of medical knowledge and, thus, they tended to approach them descriptively. Regarding adolescents’ attitudes towards young people with EDs, these were identified as neutral, a finding that also contradicts the limited available data in the literature, which show intensely stigmatizing attitudes among adolescents with EDs (Roehrig& McLean, 2009).
Students appeared to prefer to reach out their parents and friends to share their eating habits concerns, to seek for help, in contrast to existing literature that highlights a preference for contacting firstly a psychologist or mental health professional (McNicholas, O’Connor, McNamara, O’Hara, 2015). Furthermore, our findings show that adolescents prefer to contact a health professional via a telephone helpline, while a smaller proportion of participants would opt for an in-person contact. A finding consistent with existing literature, which agrees with the difficulty of seeking in-person professional help due to stigma and prejudice from the social environment (Ali et al., 2016; Hackler, Vogel, Wade, 2010).
Societal stigma serves as a "barrier" to both recognition of the issue and the need for seeking assistance or treatment to deal with the ED (Ali et al., 2016; Hackler, Vogel, Wade, 2010). Other obstacles of help-seeking include failing to perceive how serious these conditions could be, financial obstacles like treatment costs, lack of support from relatives, and absence of motivation to change their habits (Booth et al., 2004). Thus, stigma could increase both the duration and the severity of EDs and could have a deliberating impact on young individuals suffering from an ED, who are usually reluctant to seek help, driven by the fear of prejudice and criticism of peers surrounding them.
Almost two third of the students identified the described person with AN symptoms as a girl, while at least half of the students gave the same answer for BN and BED vignettes. These rates show that adolescents consistently associated the vignette's target-face with a female, indicating their perception that EDs are mostly associated with women, which is in fact true according to literature (Hadjigeorgiou, 2004). Earlier evidence suggests that drive for thinness and body dissatisfaction showed lower heritability in males. A possible explanation for this difference was offered in a study of French and German cohorts whereby inherited variations in an estrogen receptor gene (ESR1) significantly increased risk of restrictive eating and subsequently development of AN restrictive subtype (AN-R)(Versini et al., 2010).
Conclusions
EDs have been the focus of research interest in recent years due to their severe physical and psychological effects, and because of their potentially high morbidity and mortality rates. In this setting, it is becoming a necessity to treat them appropriately and promote the mental health accessibility, especially for adolescents who get mostly affected. It is also important to highlight the constant need to raise awareness among teenager groups, so that prejudices and stigmatizing belief rates towards people with EDs, get reduced even further in the future. These attitudes act as the main barrier for those who experience an ED to seek for treatment and get specialized help. The creation of telephone helplines for EDs would be an important tool for facilitating adolescents' direct access to a health specialist, which according to our survey resulted to be the preferred means of seeking professional help.
Limitations
Regarding the limitations of the study, it is important to note that the selection of participants was done using the convenience/availability sampling method, as the sample was drawn from schools to which the researcher had access, and thus, may not be enough representative of the total secondary students’ population and consequently reducing the external validity of the study. However, the present study is the first one to be conducted on a sample of Greek adolescents regarding their knowledge and attitudes towards EDs, which are a highly important issue and comes to fill this crucial gap through the use of the vignette technique. Its findings could be a valuable source for further research and high quality studies on this topic combining quantitative and qualitative methodology.
Declaration of Competing Interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding None
References
1. Ali, K., Farrer, L., Fassnacht, D.B., Gulliver, A., Bauer, S., Griffiths, K.M. (2016). Perceived barriers and facilitators towards help-seeking for eating disorders: A systematic review. International Journal of Eating Disorders, 16;50(1):9–21. Doi:10.1002/eat.22598.
2.Booth, M.L., Bernard, D., Quine, S., Kang, M.S., Usherwood, T., Alperstein, G. (2004). Access to health care among Australian adolescents young people’s perspectives and their sociodemographic distribution. The Journal of Adolescent Health: Official Publication of the Society for Adolescent Medicine, 1;34(1):97–103. Doi: 10.1016/j.jadohealth.2003.06.011.
3.Burns, J.R., Rapee, R.M. (2006). Adolescent mental health literacy: Young people’s knowledge of depression and help seeking. Journal of Adolescence,29(2):225–39.
Doi: 10.1016/j.adolescence.2005.05.004.
4.Cost,J., Krantz, M.J., Mehler, P.S. (2020). Medical complications of anorexia nervosa. Cleveland Clinic Journal of Medicine, 87(6):361–6. Doi: https://doi.org/10.3949/ccjm.87a.19084.
5.Hadjigeorgiou, Ch. (2004). Psychogenic Anorexia Psychogenic Bulimia. Review of the latest scientific data. Pediatric Update, 8:12-8.
6.Hackler, A.H., Vogel, D.L., Wade, N.G. (2010). Attitudes Toward Seeking Professional Help for an Eating Disorder: The Role of Stigma and Anticipated Outcomes. Journal of Counseling & Development, 88(4):424–31.
7.Hogg, M.A., Vaughan, G.M., Vasilikos, E. Arvanite?s, A., Chantze?A. (2010). Social Psychology. Athens: Gutenberg.
8.Jorm, A.F., Korten, A.E., Jacomb, P.A., Christensen, H., Rodgers, B., Pollitt, P. (1997). Public beliefs about causes and risk factors for depression and schizophrenia. Social Psychiatry and Psychiatric Epidemiology [Internet], 32(3):143–8.
9.Kjeldbjerg, M.L., Clausen, L.(2021). Prevalence of binge-eating disorder among children and adolescents: a systematic review and meta-analysis. European Child and Adolescent Psychiatry. Doi:10.1007/s00787-021-01850-2.
10.McNicholas, F., O’Connor, C., McNamara, N., O’Hara, L. (2015). Eating disorder services for young people in Ireland: perspectives of service providers, service users and the general adolescent population. Irish Journal of Psychological Medicine, 21;35(4):301–9. Doi:10.1017/ipm.2015.66.
11.Micali, N., Hagberg, K.W., Petersen, I., Treasure, J.L. (2013). The incidence of eating disorders in the UK in 2000–2009: findings from the General Practice Research Database. BMJ Open, 3(5): e002646.
12.Mitchell, J.E., Crow, S. (2006). Medical complications of anorexia nervosa and bulimia nervosa. CurrentOpinioninPsychiatry,19(4):438–43. https://doi.org/10.1097/01.yco.0000228768.79097.3e.
13.Napolitano, F., Bencivenga, F., Pompili, E., Angelillo, I.F. (2019). Assessment of Knowledge, Attitudes, and Behaviors toward Eating Disorders among Adolescents in Italy. International Journal of Environmental Research and Public Health, 24;16(8):1448.
DOI: 10.3390/ijerph16081448.
14.Petrie, K.J., Weinman, J. (1997). Perceptions of health & illness : current research and applications. Amsterdam: Harwood Academic Publishers.
15.Ponte, J.P. (1994). Mathematics teachers’ professional knowledge. In: Proceedings of the XVIII International Conference for the Psychology of Mathematics Education (PME). Lisbon, Portugal, p. 195–210.
16.Roehrig, J.P., McLean, C.P. (2009). A comparison of stigma toward eating disorders versus depression. International Journal of Eating Disorders, 8;43(7):671–4.
17.Simos, G. (1996). Investigation of psychogenic disorders in food intake and the possibilities of prevention [Doctoral dissertation]. [Aristotle University of Thessaloniki].
18.Smink, F.R.E., van Hoeken, D., Hoek, H.W. (2012). Epidemiology of Eating Disorders: Incidence, Prevalence and Mortality Rates. Current Psychiatry Reports, 14(4):406–14. https://doi.org/10.1007/s11920-012-0282-y.
19.Suarez-Albor, C.L., Galletta, M., Gómez-Bustamante E.M. (2022). Factors associated with eating disorders in adolescents: a systematic review. Acta Biomedica Atenei Parmensis [Internet], 1;93(3): e2022253–3. Doi:10.23750/abm.v93i3.13140.
20.Versini, A., Ramoz, N., Le Strat, Y., Scherag, S., Ehrlich, S., Boni, C. (2010). Estrogen receptor 1 gene (ESR1) is associated with restrictive anorexia nervosa. Neuropsychopharmacology, 35(8):1818–25. Doi : 10.1038/npp.2010.49