Partial Hydatidiform Mole in Ectopic Pregnancy: Report of a Rare Case
Partial Hydatidiform Mole in Ectopic Pregnancy: Report of a Rare Case
Dr. Srijita Chaudhuri 1, Dr. Debojyoti Ghosh 2*, Dr. Indranil Das 3
1,2,3. Department of Pathology, Oncquest Laboratories Ltd, Kolkata, West Bengal, India.
*Correspondence to: Dr. Debojyoti Ghosh, Consultant Histopathologist at Oncquest Laboratories Ltd.
Copyright
© 2023 Dr. Debojyoti Ghosh. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 04 September 2023
Published: 30 September 2023
Abstract
Molar pregnancy in tubal ectopic is extremely rare. The main diagnostic tool is post-operative histopathological diagnosis. Pre-operative diagnosis is difficult as clinically molar pregnancy mimics normal ectopic pregnancy. We report a case of ectopic partial molar pregnancy in the right fallopian tube of a 29year old lady that was sent to us for routine histopathological examination with the clinical diagnosis of tubal ectopic.
Keywords: Molar pregnancy, Histopathological examination, Tubal ectopic.
Partial Hydatidiform Mole in Ectopic Pregnancy: Report of a Rare Case
Introduction
Most of the gestational trophoblastic disease (GTDs) occur in uterus, but ectopic molar pregnancy is very rare. Diagnosis of ectopic molar pregnancy is very difficult as there is no distinguishing features except histopathological diagnosis and DNA ploidy analysis. Combination of molar and ectopic pregnancy is extremely rare finding. We present a case of tubal partial mole that was diagnosed accidentally during routine histopathological examination of salpingectomy specimen.
Case Report:
A 29-year-old non-smoker, non-alcoholic lady went to a nearby gynecology clinic with chief complaints of acute severe lower abdominal pain with recent onset vaginal bleeding. She was 9weeks pregnant. She was non-smoker, non-alcoholic and had no known allergy to food or medicines.
On examination, her blood pressure was 100/60mm of Hg with pulse rate of 90/min. Per abdominal examination showed tenderness over right iliac fossa with no rigidity. On per speculum examination there was blood in vagina.
Pregnancy card test in the clinic was positive. Urgent ultrasound scan revealed an antenatal bulky uterus without any evidence of intrauterine pregnancy. There was a complex right adnexal mass measuring 5x2.5x2cm containing a gestational sac. Pouch of Douglas showed blood. All these findings were consistent with ectopic right tubal pregnancy. Her hemoglobin level was 9.5mg/dl and β HCG level was 20,000Units/ml.
Based on the clinical diagnosis, exploratory laparotomy was done which revealed normal left adnexa and right tubal pregnancy with active bleeding in the tube. Right salpingectomy was done and the formalin fixed specimen was sent to our laboratory for histopathological examination.
Gross examination: The content of tube consisted of grey, brown hemorrhagic material along with a part of patent fallopian tube measuring 4.5x 2.2x 1.3cm. Entire tissue was submitted for histopathological examination.
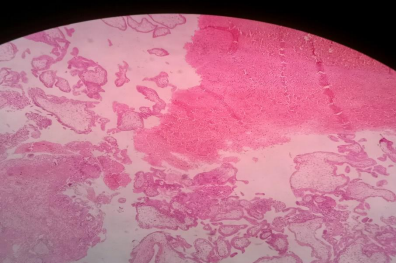
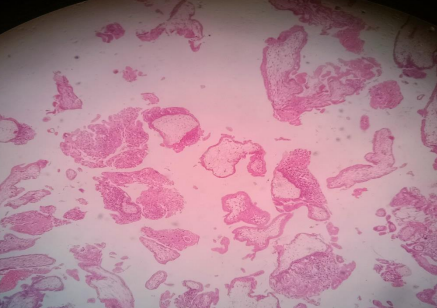
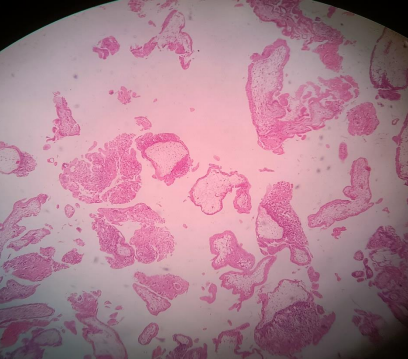
Microscopic examination: Sections showed multiple chorionic villi of variable sizes, predominantly hydropic and admixed with few normal appearing villi. Enlarged villi were irregularly shaped with scalloped borders and secondary trophoblastic pseudo-inclusions were seen. Fetal nucleated RBCs were abundant. Circumferential trophoblastic hyperplasia was noted. Based on the above histological features a diagnosis of partial molar ectopic pregnancy was made. However, patient was advised karyotyping for further confirmation. Follow up with serial B HCG estimation was done which showed a gradual decline.
Figure 1: Chorionic villi of variable sizes
Figure 2: Patent fallopian tube
Figure 3: Scalloping of villi
Figure 4: Circumferential trophoblastic hyperplasia
Discussion:
Ectopic molar pregnancy is an extremely rare condition with an incidence of 1-5/ 2,00000 (1). The diagnosis of this entity predominantly depends on histopathology examination (2).
Hydatidiform mole is characterized by hydropic degeneration of chorionic villi and circumferential proliferation of trophoblastic tissue. Hydatidiform moles arise due to abnormal fertilization. Partial mole is a pathological condition due to fertilization of the ovum by two sperms and paternal to maternal chromosomal ratio becomes 2:1 (3). Clinically ectopic molar pregnancy is indistinguishable from non-molar ectopic pregnancy (4). Histopathological examination of surgically removed salpingectomy specimens can confirm or exclude molar pregnancy. During microscopic examination pathologists should know that degree of extravillous trophoblastic proliferation may appear more florid in ectopic pregnancy (5,6).
Pasic et al. suggested that in unruptured tubal ectopic, salpingotomy is the treatment of choice. (7) However, in our case it was ruptured at the time of diagnosis, so salpingectomy was the only suitable treatment.
Conclusion:
Ectopic molar pregnancy is an extremely rare occurrence. For the correct diagnosis and further management of ectopic molar pregnancy, histopathological examination of the salpingectomy specimen plays an important role.
References
1.Siozos A, Sriemevan A: A case of true tubal hydatidiform mole and literature review. BMJ Case Rep. 2010 2010: bcr0720092123. 10.1136/bcr.07.2009.2123.
2. Zhao T, Hou X, Su C, Wu Q: Tubal hydatidiform mole treated with salpingotomy: a case report. Clin Case Rep. 2019, 7:653-655. 10.1002/ccr3.2037
3.Burton JL, Lidbury EA, Gillespie AM, et al.: Over-diagnosis of hydatidiform mole in early tubal ectopic pregnancy. Histopathology. 2001, 38:409-417. 10.1046/j.1365-2559.2001.01151x
4.Siozos A, Sriemevan A: A case of true tubal hydatidiform mole and literature review . BMJ Case Rep. 2010, 2010:bcr0720092123. 10.1136/bcr.07.2009.2123
5.Gari R, Abdulgader R, Abdulqader O: A live 13 weeks ruptured ectopic pregnancy: a case report . Cureus. 2020, 12:e10993. 10.7759/cureus.10993.
6.Sebire NJ, Makrydimas G, Agnantis NJ, Zagorianakou N, Rees H, Fisher RA: Updated diagnostic criteria for partial and complete hydatidiform mole in early pregnancy. Anti-cancer Res. 2003, 23:1723-1728.
7.Pasic RP, Hammons G, Gardner JS, Hainer M: Laparoscopic treatment of cornual heterotopic pregnancy, J Am Assoc Gynecol Laparosc. 2000, 9:372-375.