Combined Oral Contraceptives Related Myocardial Infarction, a Risk Factor to Bear in Mind.
Combined Oral Contraceptives Related Myocardial Infarction, a Risk Factor to Bear in Mind.
Dr. Geordan Goire Guevara, MD. FACC*1. Dr. Victor Elliot, MBBS, FSCAI2. Dr. Andrene Chung, MBBS. FACC3.
1,2,3. Partner Interventional Centre of Jamaica.
*Correspondence to: Dr. Geordan Goire Guevara, Partner Interventional Centre of Jamaica.
Copyright
© 2023 Dr. Geordan Goire Guevara. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 17 August 2023
Published: 30 September 2023
Abstract
Myocardial infarction, colloquially known as "heart attack," is caused by decreased or complete cessation of blood flow to a portion of the myocardium. Myocardial infarction may be silent, and go undetected, or it could be a catastrophic event leading to hemodynamic deterioration and sudden death. Most myocardial infarctions are due to underlying coronary artery disease and the risk to suffer from this deadly event is linked to the presence of several risk factors like hypertension, diabetes, obesity, dyslipidemia, smoking or stress. Combined oral contraceptives (COCs) have been associated with an increased risk of arterial thrombosis, myocardial infarction or ischemic stroke. However, as these diseases are rare in young women and as many types of combined oral contraception exist, the magnitude of the risk and the effect of different hormonal contents of COC preparations remain unclear.
Key words: Myocardial infarction, sudden death, combined oral contraceptives, ischemic stroke
Combined Oral Contraceptives Related Myocardial Infarction, a Risk Factor to Bear in Mind.
Introduction
Myocardial infarction (MI) is defined pathologically as myocardial cell death due to prolonged ischemia. Diminished cellular glycogen, and relaxed myofibrils and sarcolemmal disruption, are the first ultrastructural changes and are seen as early as 10–15 minutes after the onset of ischemia. 1
It is estimated that over 17 million people die from cardiovascular diseases annually, with over 80% of deaths occurring in low-and middle-income countries. Myocardial infarction most often occurs when an atherosclerotic plaque (a collection of fatty acids, fibrous tissue and leukocytes) ruptures in the wall of a coronary artery. The plaque contents obstruct the artery and deprive the downstream part of the heart muscle of oxygen.2 Combined oral contraceptives (COCs) are the most commonly used reversible form of contraception in developed countries.3
They contain an estrogen and a progestogen that are usually taken together in one pill for the first 21 days of every menstrual cycle, followed by a pill-free week. COCs prevent ovulation, mainly by suppressing the surge in luteinizing hormone (due to the progestogen content).4
Studies in young women have shown an association between combined oral contraception use and an increased risk of myocardial infarction and ischemic stroke. However, as these diseases are rare in young women and as many types of combined oral contraception exist, the magnitude of the risk and the effect of different hormonal contents of combined oral contraceptive preparations remain unclear.5
We present a case of a young female patient with no risk factors for coronary artery disease who suffered from an acute myocardial infarction while taking COCs for a long period of time.
Case presentation
29-year-old female patient with no past medical history who developed acute oppressive-like chest pain suddenly while sleeping during the night, radiating to back with cold sweat and nausea. She initially stayed at home but refers that the pain worsened gradually until it was irresistible early in the morning and that’s why she went to the emergency and accident department of the local hospital for further assessment.
On examination the blood pressure was normal but heart sounds were tachycardic with a heart rate in 110 bpm, the O2 saturation was 97%, no S3-S4 gallop, wheezes or crackles were found. To note she was not found with the classical risk factors for coronary artery disease but she had been taking combined oral contraceptive pill microgynon 30 (levonorgestrel and ethinyl estradiol) for more that 5 years and did not have regular follow-up consultations with the gynecologist.
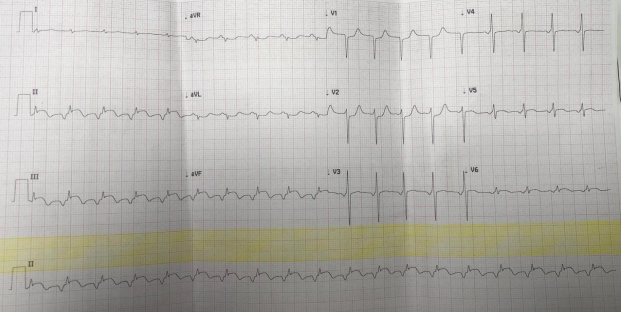
It was carried out an ECG that showed a rapid rhythm, with regular and narrow QRS complexes, but negative P waves in II-III and aVF leads and small biphasic (positive, then negative) P waves in V1 lead, suggestive of a focal atrial tachycardia that based on the morphological analysis of the P wave, that was likely originating at the level of the coronary sinus body. The ECG also showed leftward axis deviation, low QRS voltage in limb leads, long QTc interval (480 ms) according to Fridericia score and > 1mm ST-segment elevation in II, III and aVF leads with subtle ST-segment depression in aVL lead suggesting reciprocal ischemic changes, and also > 1 mm ST-segment depression in V1-V2 leads with subtle ST-segment elevation in V5-V6 leads, all this suggestive on an ongoing acute inferolateral myocardial infarction. Figure 1.
It was also performed cardiac biomarker enzymes such as troponin I qualitative which was positive, CPK in 599 IU/L and CKMB in 58.6 IU/L (both elevated) with the CKMB-CK index in 9.78, which confirmed the presence of myocardial injury and acute myocardial infarction.
The acute coronary syndrome protocol was activated and she was managed with load dose of aspirin and ticagrelor, nitroglycerin was administered sublingually, and amiodarone was administered intravenously which helped revert the focal atrial tachycardia to sinus rhythm. Then the Cath lab was activated and the patient was referred for coronary angiogram and primary percutaneous coronary intervention (PCI).
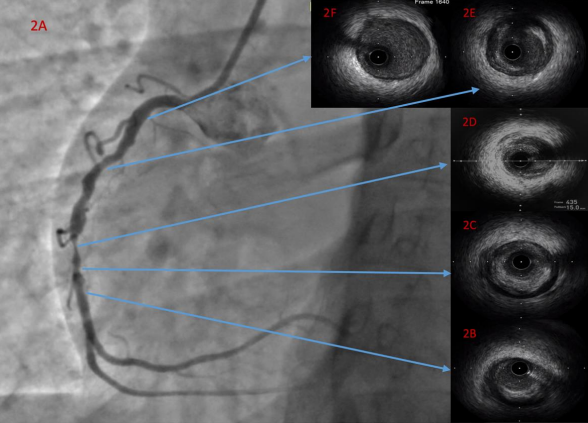
It was carried out a coronary angiogram that showed a no angiographic lesions in the left anterior descending and circumflex arteries, however the right coronary artery showed proximal non-significant irregular plaques, there was a 95% mid segment focal stenosis. Figure 2A. Taking into account that an acute MI is a rare condition in female young patients with no risk factors, and the elevated odds of spontaneous coronary artery dissection as cause of the acute coronary event based on the angiographic images, we decided to perform intravascular ultrasound (IVUS) in the right coronary artery to understand the mechanism of this MI, guide the PCI, assess the final result and manage potential complications of the intervention.
The IVUS pullback assessment showed an extensive concentric plaque burden from distal to proximal segment of the right coronary artery (figures 2B, 2C, 2E and 2F), with a tight stenosis with concentric plaque and dissection at 5 o’clock at the site of the referred 95% stenosis (figure 2D).
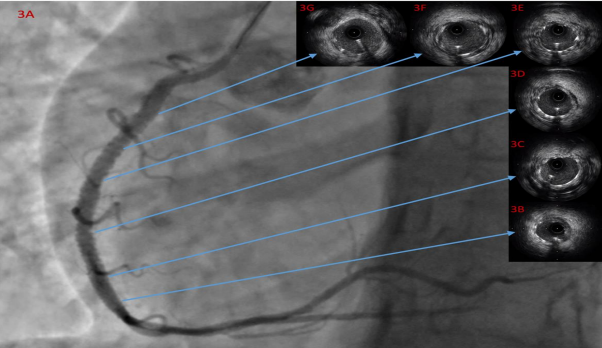
After pre-dilatation with scoring balloon, two drug eluting stents were deployed from the aforementioned and predilated 95% stenotic lesion to proximal right coronary artery and overlapping technique was performed between both stents with a non-compliant balloon. (Figure 3A). Then another IVUS assessment was run and showed excellent apposition with no edge dissection, under-expansion, marked residual stenosis or tissue protrusion. (Figures 3B, 3C, 3D, 3E, 3F and 3G).
The patient was admitted at the coronary care unit and discharged after 5 days with no further ischemic-related clinical symptoms or complications, and she was advised to continue on cardiology follow-up consultation, life-style modification, compliance to medical therapy and visit her gynecology for birth counselling since she cannot longer take COCs or any hormonal formulation for birth control.
Discussion
The recognition that adverse vascular events associated with the use of oral contraceptives are dose related has led over the years to marked decreases in the amount of both estrogen and progestin contained in combination formulations.6
Estrogen has been known to have prothrombotic effects and elevates cardiovascular venous thromboembolism (VTE) risk by increasing prothrombin and decreasing antithrombin III.7
Tanis et al. performed a case-control study of 1,173 women over 6 years and concluded that the use of second-generation oral contraceptives (OCs), containing levonorgestrel, increased the risk of MI by a relative risk of 2.3, while third-generation, containing desogestrel or gestodene, and other progestins such as cyproterone or norgestimate, did not significantly increase the risk.8
Lidegaard et al. stated that women who used oral contraceptives with ethinyl estradiol at a dose of 30 to 40 mg had a risk of arterial thrombosis that was 1.3 to 2.3 times as high as the risk among non-users, and women who used pills with ethinyl estradiol at a dose of 20 mg had a risk that was 0.9 to 1.7 times as high, with only small differences according to progestin type. They estimated that among 10,000 women who use desogestrel with ethinyl estradiol at a dose of 20 mg for 1 year, 2 will have arterial thrombosis and 6.8 women taking the same product will have venous thrombosis. Although venous thrombosis is three to four times as frequent as arterial thrombosis among young women, the latter is associated with higher mortality and more serious consequences for the survivors.9
A recent study reporting that therapy with exogenous hormones is associated with microalbuminuria10, an indicator for early endothelial cell damage and also a predictor of cardiovascular events11, suggests that oral contraceptives cause a disturbance of endothelial cell function.
The higher risk of cardiovascular events has been associated with changes in lipid metabolism caused by oral contraceptives through the modification of low-density lipoprotein (LDL) and high-density lipoprotein cholesterol (HDL-C) levels12 and the chronic subclinical inflammation13. In addition, they act like procoagulant agents, favoring a hypercoagulability state, and then raising the risk of thromboembolic diseases. 14
Inflammation is an uninterrupted effect of the atherosclerotic process, which promotes the formation of the lipid stria, and even the movement and rupture of the atherosclerotic plaque. 15, 16 Thus, it is known that the atherosclerotic process is chronic and has a long subclinical phase. 13 High-sensitivity C-reactive protein (hsCRP) is the best biomarker of chronic subclinical inflammation and is associated with the risk of cardiovascular diseases. 17, 18 It has been demonstrated that the use of oral contraceptives may increase hsCRP levels, contributing to a higher cardiovascular risk. 13, 19
Ernst Rietzschel et al. conducted a study that involved 1301 healthy women aged 35 to 55 in Belgium; 81% had taken oral contraceptives for at least one year, with an average of 13 years. About one-fourth of them were still on the pill. The women were at low risk for cardiovascular disease but agreed to undergo vascular echography of the carotid and femoral arteries. Results showed that every decade of use was associated with a 42% increased risk in having bilateral carotid plaque and a 34% increased risk in having bilateral femoral plaque and plaque buildup in any artery is directly associated with an increased risk of coronary artery disease.20
Focal atrial tachycardia (AT) may occur in patients with organic heart disease in response to atrial stretch due to elevated atrial pressure in conditions such as hypertension and cardiomyopathy. In addition to chronic heart disease, AT can also be associated with acute events such as a myocardial infarction, pulmonary decompensation, infection, excessive alcohol ingestion, hypokalemia, hypoxia, stimulants, cocaine ingestion, and theophylline.21
Lesser et al. stated that atrial tachycardia was noted in 32 of 119 patients with acute myocardial infarction, a 27% prevalence. The site of infarction was anterior in 50%, inferior in 38%, and indeterminate in the remainder. Congestive failure or cardiogenic shock was noted in 22%, and pericarditis was present in 19%. The frequency of these complications was similar in a group of patients treated for acute myocardial infarction without atrial tachycardia: congestive heart failure or cardiogenic shock in 20% and pericarditis in 18%. This study suggests that atrial tachycardia is a common arrhythmia in the early stages of acute myocardial infarction. Although it occurs frequently, it generally follows a benign course. In rare instances, atrial tachycardia is more sustained and may result in important hemodynamic impairment.22
This benign and common form of atrial tachycardia shares many features with accelerated idioventricular rhythm, a rhythm attributed to enhanced automaticity.23
Due to this acute coronary event happened in a young female patient with no risk factors for CAD, our initial thought was that it was likely caused by spontaneous coronary artery dissection which is far commoner in this subset of patients, but the IVUS guided procedure helped us clarify the mechanism of this event by demonstrating an early and marked atherosclerotic process in the coronary tree of this patient.
The screening for coronary artery disease risk factor in female patients taking COCs should always be carried out by primary care or gynecologist physicians to avoid potential vascular complications which can limit the quality of life in this essential subset of the population because it is better to prevent than to treat.
Figure 1. ECG performed in the emergency and accident department.
Figure 2A. coronary angiogram RAO 30-degree view showing the angiographic lesions. 2B, 2C, 2D, 2E and 2F show the IVUS assessment.
Figure 3A. coronary angiogram RAO 30-degree view showing the angiographic result after stenting. 3B, 3C, 3D, 3E, 3F and 3G show the IVUS assessment after the percutaneous coronary intervention with excellent result.
References
1.Jennings RB, Ganote CE. Structural changes in myocardium during acute ischemia. Circ Res. 1974;35:156–172.
2.Nabel EG, Braunwald E. A tale of coronary artery disease and myocardial infarction. New England Journal of Medicine 2012;366(1):54?63. [PUBMED: 22216842]
3.United Nations. World Contraceptive Use 2011. http://www.un.org/esa/population/publications/contraceptive2011/contraceptive2011.htm (accessed 08 July 2015). Find Article
4.Speroff L, Darney PH. A Clinical Guide for Contraception. 5th Edition. Wolters Kluwer, 2011.
5.Zakharova MY, Meyer RM, Brandy KR, Datta YH, Joseph MS, Schreiner PJ, et al. Risk factors for heart attack, stroke, and venous thrombosis associated with hormonal contraceptive use. Clinical and Applied Thrombosis/Hemostasis 2011;17(4):323?31. [PUBMED: 20530058] Add to Library
6.Mishell DR, Jr. Oral contraception: past, present, and future perspectives. Int J Fertil 1991;36:(supp1)7-18.
7.Ouyang P, Michos ED, Karas RH. Hormone replacement therapy andthe cardiovascular system: lessons learned and unanswered questions.J Am Coll Cardiol 2006;47:1741–53.
8.Tanis BC VM, Kemmeren JM, Cats VM, et al. Oral contraceptivesand the risk of myocardial infarction. N Engl J Med 2001;345:1787–93.
9.1. Lidegaard Ø, Løkkegaard E, Jensen A, Skovlund C, Keiding N. Thrombotic Stroke and Myocardial Infarction with Hormonal Contraception. New England Journal of Medicine. 2012;366(24):2257-2266.
10.MONSTER TB, JANSSEN WM, DE JONG PE, DE JONG-VAN DEN BERG LT: Oral contraceptive use and hormone replacement therapy are associated with microalbuminuria. Arch. Intern. Med. (2001) 161:2000-2005.
11.GERSTEIN HC, MANN JF, YI Q et al.: Albuminuria and risk of cardiovascular events, death, and heart failure in diabetic and nondiabetic individuals. JAMA (2001) 286:421-426.
12.Fazio G, Ferrara F, Alessandro GBC, Ferro F, Novo G, Novo S. Protrhombotic effects of contraceptives. Current Pharmaceutical Design. 2010; 16(1): 3490-6.
13.Petto J, Pereira LS, Santos ACN, Giesta BA, Melo TA, Ladeia AMT. Inflamação subclínica em mulheres que utilizam contraceptivo oral. Revista Brasileira de Cardiologia. 2013; 26(6): 465-71.
14.Ferreira ACP, Montes MBA, Franceschini AS, Toloi MRT. Efeitos do contraceptivo oral contendo 20 µg de etinilestradiol e 150 µg de desogestrel sobre os sistemas de coagulação e fibrinólise. Rev Bras Hematol Hemoter. 2010; 22(2): 77-87.
15.Pearson TA, Mensah GA, Alexander RW, et al; Centers for Disease Control and Prevention; American Heart Association. Markers of inflammation and cardiovascular disease: application to clinical and public health practice: a statement for healthcare professionals from the Centers for Disease Control and Prevention and the American Heart Association. Circulation. 2003; 107(3): 499-511.
16.Liao JK. Beyond lipid lowering: the role of statins in vascular protection. Int J Cardiol. 2002; 86(1): 5-18.
17.Pepys MB, Hirschfield GM. C-reactive protein: a critical update. J Clin Invest. 2003; 111(1): 1805-12.
18.Harrison M, O'Gorman DJ, McCaffrey N, et al. Influence of acute exercise with and without carbohydrate replacement on postprandial lipid metabolism. J Appl Physiol. 2009; 106(3): 943-9.
19.Sorensen CJ, Pedersen OB, Petersen MS, et al. Combined oral contraception and obesity are strong predictors of low-grade inflammation in healthy individuals: results from the Danish Blood Donor Study (DBDS). PLoS One. 2014; 9(2): 1-8.
20.3. Rietzschel E, De Buyzere M, De Baquer D, Bekaert S, Segers P, Cassiman P et al. Abstract 3614: Anticonceptive Drug Use And Increased Carotid and Femoral Plaque Prevalence: Population Data From Asklepios. Circulation. 2007;116(suppl_16).
21.Akhtar, M. Supraventricular tachycardias. Electrophysiologic mechanisms, diagnosis and pharmacologic therapy. In: Tachycardias: Mechanisms, Diagnosis, Treatment, Josephson, ME, Wellens, H (Eds), Lea & Febiger, Philadelphia 1984. p.137.
22.Lesser L. Atrial Tachycardia in Acute Myocardial Infarction. Annals of Internal Medicine. 1977;86(5):582.
23.Gallagher JJ, Damato An, Lau Sh: Electrophysiologic studies during accelerated idioventricular rhythms. Circulation 44:671-677, 1971