Flexible Bronchoscopy as a Diagnostic Procedure for a laryngeal or Hypopharyngeal Lesion in Patients High Risk for General Anaesthesia
Flexible Bronchoscopy as a Diagnostic Procedure for a laryngeal or Hypopharyngeal Lesion in Patients High Risk for General Anaesthesia
Dr.Sobha Subramaniam*1, Dr.Amit Kumar Pandey2, Dr.Rabari Rushi3, Dr.Subramaniam Iyer K4
1 Professor and head of pulmonary medicine in Amrita Institute of Medical sciences.
2. Post-doctoral, DM Pulmonary medicine in Amrita Institute of Medical sciences.
3. Senior resident DM Pulmonary medicine in Amrita Institute of Medical sciences.
4. Professor and Head of Head and Neck Surgery in Amrita Institute of Medical sciences, Kochi
*Correspondence to: Dr. Sobha Subramaniam, Professor and head of pulmonary medicine in Amrita Institute of Medical sciences.
Copyright
© 2023 Dr. Sobha Subramaniam. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 04 September 2023
Published: 30 September 2023
Abstract
Background: Biopsy of vocal cord and hypopharyngeal lesion are usually performed by otorhinolaryngologists with rigid laryngoscope under general anesthesia. In patients who are high risk for general anesthesia the procedure can be morbid. In such situations flexible bronchoscopy gives excellent visualization allowing the biopsy to be done under local anesthesia and conscious sedation.
Aims and Objectives: To assess the diagnostic ability and safety of flexible bronchoscopy under local anesthesia for biopsy of laryngeal and hypopharyngeal lesions.
Methods: This is a retrospective study of consecutive patients who underwent flexible bronchoscopy(FB) for hypopharyngeal and laryngeal lesions for a period of 18 months in our hospital. They were referred from Head & Neck surgery department in view of high risk complication probability for GA. The airway was deemed to be adequate for the procedure prior to the referral. The procedure was done with local anesthesia and conscious sedation (intravenous midazolam and fentanyl).
Results: 30 patients underwent the procedure. Out of this, 28 patients were poor candidates for GA due to co morbidities and 2 patients wished to avoid GA.23 had lesions in vocal cords, 4 had lesions in vocal cord and pyriform fossa and 3 had lesions only in the pyriform fossa. Diagnosis achieved in 28 (93.33%) patients. There was no associated complications except for minor bleeding in 5 which could be controlled with local measures.
Conclusions: We report our experience of performing biopsy with FB under conscious sedation as an outpatient procedure in hypopharyneal/laryngeal lesions with very good diagnostic yield and without significant complications.
Flexible Bronchoscopy as a Diagnostic Procedure for a laryngeal or Hypopharyngeal Lesion in Patients High Risk for General Anaesthesia
Introduction
The fifth most prevalent cancer worldwide is head and neck cancer. The prognosis of laryngopharyngeal carcinoma significantly improve with an early diagnosis. Early diagnosis increases the likelihood of survival and maintain laryngeal function. The diagnostic evaluation includes biopsy as well as assessment of extent of lesion. Traditionally, general anesthesia is used to perform the biopsy of laryngopharyngeal lesions. Biopsy of vocal cord and hypopharyngeal lesions is usually performed by otorhinolaryngologists with rigid laryngoscope under general anesthesia.
The general anesthesia has risks and can be potentially lethal in patients with multiple comorbidities. (Recent myocardial infraction,chronic renal failure,advanced COPD)
Other minimally invasive techniques may be helpful in these circumstances. Under local anesthesia and conscious sedation, flexible bronchoscopy (FB) provides excellent visualization of laryngeal and hypopharyngeal structures and allowing biopsy to be taken from the lesions. We report our experience of performing biopsy with FB under conscious sedation as an outpatient procedure in hypopharyneal/laryngeal lesions with very good diagnostic yield and without significant complications.
Methods
This is a retrospective study of consecutive patients who underwent flexible bronchoscopy for hypopharyngeal and laryngeal lesions for a period of 18 months in our hospital. They were referred from department of Head & Neck surgery in view of high risk for GA. The airway was deemed to be adequate for the procedure prior to the referral.
Flexible bronchoscopy was carried out in a procedure room at the outpatient department following the patients' informed consent with local anesthesia and conscious sedation (intravenous midazolam and fentanyl).Topical anaesthetic was applied before the biopsy using a 4% lidocaine spray. It was applied to the pharynx and larynx and there were between five and ten sprays.
Biopsies were obtained using a flexible video bronchoscope with a 2.8 mm diameter working channel (BF 1TH 190,Olympus Medical) and a 1.8 mm diameter flexible biopsy forceps. Images were displayed and recorded using a video processor .During biopsy, the flexible bronchoscope was inserted transnasally / transorally in patients in a supine position.
After visualization of the laryngopharyngeal lesion, a biopsy forceps was passed through the working channel. The lesion was approached with an open jaw biopsy forceps, pushed deep into the lesion, and closed. The biopsy forceps was pulled back swiftly, while feeling for resistance when removing the tissue from the suspected lesion. Four deep biopsies were taken from each suspected lesion. All biopsies were performed by two physicians, a senior pulmonologist and senior residents under direct supervision. Information was gathered about the patient's characteristics, including age, sex, anticoagulant use, biopsy site, and complications.
Result
Thirty patients underwent the procedure .Patient characteristics are shown in table 1. The study population consisted of males only(100%) mean age of 66.8 years. The most common biopsy site was the vocal cords in twenty three patients (76.67%),four (13.33%) patients had lesions in both vocal cord and pyriform fossa and 3 (10%) had lesions only in the pyriform fossa. Histology results were squamous cell carcinoma in 63.33% and severe dysplasia and carcinoma in situ in 30%.Diagnosis achieved in 28 (93.33%) patients. There was no major complications following the procedure .there was minor bleeding in 5 patients which could be controlled with local measures.
Discussion
Vocal cord or pyriform fossa biopsies are typically performed using rigid laryngoscope under GA. Complication of GA include myocardial infarction, arrhythmia ,cardiac arrest, heart failure, atelectasis, aspiration, and bronchospasm. Rigid laryngoscopy can cause injury to the upper airway structures including vocal cords. In such a circumstance, Fiber optic bronchoscopy is a safer options for diagnosis. When safety is a primary concern, FB has substantial advantages over rigid laryngoscopy in high-risk situations. FB is well tolerated and performed as an outpatient procedure under local anaesthetic and conscious sedation. Complications are also not major (Eg. Minor bleeding after biopsy) when compare to rigid laryngoscope.
The cases with substantial comorbidities were first identified by a laryngologist and after risk assessment referred for a FB biopsy. The airway was deemed to be adequate for the procedure prior to the referral. The planned Vocal Cord biopsies in our investigation were referred by laryngeal experts because of expected technical challenges brought on by comorbidities and the requirement for patient cooperation. But bronchoscopy has some constraints. For the obtaining sufficient tissue without injuring the VC, a skilled operator is needed to sample the lesions using a bronchoscope. This study uses retrospective design which had inherent drawbacks. In addition there was a chance of selection bias, as
patient's ability to comply during bronchoscopy under topical anesthesia was also assessed by the doctor. Since this is a subjective measurement, it may vary between doctors.
In our study we found that fibre optic bronchoscopy requires cautious patient selection. For patients who are at high risk for GA and are therefore not candidates for rigid laryngoscopy, it serves as a substitute procedure with a good results. It is a time saving procedure and it involves less cost.
To prevent complications of GA , we suggest that skilled bronchoscopist should try to collect biopsies of hypopharyngeal and laryngeal lesions first, saving rigid laryngoscopy under general anaesthesia for when the biopsies are unsatisfactory. In our study only one patient out of 30 required rigid laryngooscopy for diagnosis as a second procedure. This confirms usefulness of the FB in vocal cord and hypopharyngeal lesion as a first procedure.
|
Characteristics |
Flexible Bronchoscopy Biopsy |
Percentage % |
|
Study Population |
30 |
100% |
|
Sex ( Number of Males) |
30 |
100% |
|
Age (range) |
66.8(51-88) |
|
|
Site of Biopsy |
|
|
|
Vocal cord |
23 |
76.67 |
|
Pyriform fossa |
3 |
10 |
|
Vocal cord + Pyriform Fossa |
4 |
13.33 |
|
Definitive Histology |
|
|
|
Hyperplasia |
2 |
6.67 |
|
Mild/Moderate Dysplasia |
4 |
13.33 |
|
Carcinoma in situ |
5 |
16.67 |
|
Squamous cell carcinoma (no) |
19 |
63.33 |
Table 1
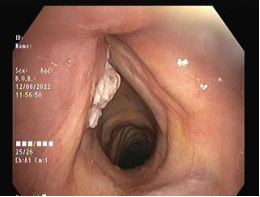
Figures 1,2,3,4
Conclusion
We report our experience of performing FB with under conscious sedation as an outpatient procedure of hypopharyngeal/laryngeal lesion with a very good diagnostic yield and without any significant complications. It can be considered as a routine method for procurement of biopsy material in these lesions particularly in high risk patients who are poor candidates for general anesthesia.