The Shifting Sands of a Great Imitator: Diagnostic Considerations of Disease Activity in Cardiac Sarcoidosis
The Shifting Sands of a Great Imitator: Diagnostic Considerations of Disease Activity in Cardiac Sarcoidosis
Niall Leahy, MBBAOBCH, MRCPI;1Naeif Almagal, MBBS;1,2,3* James Mannion MB BAO BCH, MRCPI;1 JohnW. McEvoy, MBBCh, MHS1,4
1. Division of Cardiology, Department of Medicine, Saolta University Healthcare Group, University Hospital Galway, Galway, Ireland.
2. Prince Mohammed bin Abdulaziz Medical City, Ministry of Health, Saudi Arabia.
3. School of Medicine, University of Galway, Galway, Ireland.
4. National Institute for Prevention and Cardiovascular Health, School of Medicine, National University of Ireland Galway, Galway, Ireland.
*Corresponding Authors: Dr.Naeif Almagal; e-mail: nmf1988g@hotmail.com.
Copyright
© 2023 Dr. Naeif Almagal. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 30 September 2023
Published: 10 October 2023
Abstract
Background – Cardiac sarcoidosis is frequently clinically asymptomatic, possibly leading to underestimation of its prevalence. The manifestations of cardiac sarcoidosis can exhibit significant variability, encompassing arrhythmias and heart failure.
Case Summary – A 77-year-old male presented for elective spinal decompression surgery. Intraoperatively, he experienced episodes of monomorphic ventricular tachycardia. Comprehensive imaging revealed a left ventricular wall aneurysm, with cardiac MRI features suggestive of an ischemic origin. However, coronary angiography showed no significant coronary artery stenosis. Subsequent FDG-PET-CT depicted egg-shell calcified adenopathy in the hilum and mediastinum, characteristic of prior sarcoidosis, with no FDG-avid uptake in the heart or lungs. Thus, the findings indicated previous sarcoidosis but no current disease activity, eliminating the need for immunosuppressant up-titration. The patient received an implantable cardioverter defibrillator device before discharge.
Discussion – Clinicians should recognize that cardiac sarcoidosis can be diagnosed without relying on endomyocardial biopsy confirmation. Non-invasive cardiac sarcoidosis diagnosis relies on identifying characteristic imaging features, which can also gauge current disease activity. This knowledge holds significant therapeutic implications, as exemplified in this case study.
Keywords:
cardiac sarcoidosis, ventricular arrhythmias, non-invasive imaging, myocardial ischemia, guidelines
The Shifting Sands of a Great Imitator: Diagnostic Considerations of Disease Activity in Cardiac Sarcoidosis
Learning Points:
- Underrecognition of Cardiac Sarcoidosis: The case underscores the challenge of recognizing cardiac sarcoidosis in clinical practice. It serves as a reminder that this condition is often underestimated, despite its potential for serious consequences.
- Advanced Diagnostic Criteria: We discuss the importance of updated diagnostic criteria that incorporate modern imaging modalities. These criteria no longer necessitate invasive tissue biopsies for diagnosis. This represents a significant advancement in the field, making it easier to identify and manage cardiac sarcoidosis promptly.
- Role of Advanced Imaging: The case highlights the crucial role of advanced imaging techniques, such as cardiac MRI and FDG-PET scans, in assessing cardiac sarcoidosis. These tools not only aid in diagnosis but also provide valuable information about the disease's activity level within the myocardium.
- Therapeutic Implications: Understanding the activity level of cardiac sarcoidosis is essential because it has direct therapeutic implications. The case emphasizes that the disease's activity status can guide treatment decisions, particularly concerning the use of immunosuppressant agents. Active disease often warrants more aggressive treatment, while inactive disease may require a different management approach.
- Multidisciplinary Approach: Complex cases like this one highlight the importance of a multidisciplinary approach. Involvement of various medical specialists, including cardiologists, anesthesiologists, radiologists, and cardiothoracic surgeons, was critical in achieving an accurate diagnosis and planning appropriate interventions.
In summary, the case provides valuable insights into the challenges of recognizing and diagnosing cardiac sarcoidosis. It also emphasizes the significance of advanced imaging in both diagnosis and disease activity assessment, which, in turn, influences treatment decisions. A collaborative, multidisciplinary approach is essential for optimal patient management in such complex cases.
Primary Specialties involved other than Cardiology:
- Radiology
- Anesthesiology
- Orthopedic surgery
- Respiratory Medicine
- General Practice
Introduction:
Sarcoidosis, initially described in 1877, is a multisystem disease with variable prevalence influenced by race and ethnicity (1). While cardiac involvement is clinically evident in around 5% of sarcoidosis cases, autopsy studies suggest a higher prevalence of subclinical cardiac sarcoidosis (3). Consequently, a substantial number of individuals may have asymptomatic cardiac involvement. Data from autopsy studies and non-invasive imaging indicate that cardiac sarcoidosis is present in approximately 20-27% of individuals with systemic sarcoidosis in the United States and can be as high as 58% in Japan (4).
Isolated cardiac sarcoidosis, a condition where sarcoidosis affects the heart exclusively, is estimated to affect 5 to 15% of cardiac sarcoidosis patients. Historically, it may have been under diagnosed due to limitations in previous diagnostic criteria, which required endomyocardial biopsy in the absence of extra cardiac disease. However, new diagnostic guidelines introduced by the Japanese Circulation Society (JCS) in 2016 have provided a pathway for diagnosing isolated cardiac sarcoidosis without the need for endomyocardial biopsy (4,5)
Time line
Day 0: The patient presented for elective spinal decompression surgery.
Day 1: During surgery, a brief episode of unstable monomorphic ventricular tachycardia occurred, which spontaneously resolved. A second brief episode of ventricular tachycardia occurred after the surgery.
Day 2: Additional episodes of stable non-sustained ventricular tachycardia and a short episode of severe sinus bradycardia with ventricular escape beats were observed.
Day 5: A transthoracic echo revealed abnormalities, including an aneurysmal basal posterolateral segment, basal-mid posterior and lateral akinesis, focal basal inferior akinesis, and severe apical infero-septal hypokinesis. The left ventricular ejection fraction was reduced to 35%.
Day 7: Cardiac MRI showed an aneurysm in the basal anterolateral and inferolateral regions, along with myocardial thinning and near transmural sub-endocardial late gadolinium enhancement. Cardiologists considered these findings most suggestive of an ischemic cause.
Day 9: Coronary angiography showed minor disease in the mid left anterior descending artery (10% stenosis) but was otherwise normal.
Day 11: An implantable cardioverter defibrillator (ICD) was inserted after detailed discussions with the patient. Medications including amiodarone, perindopril, and eplerenone were initiated before discharge.
Day 12: The patient was discharged from the hospital with plans for outpatient FDG-PET CT imaging and follow-up in the Cardiology outpatient clinic.
Case Presentation
A 77-year-old male presented for elective spinal decompression surgery due to spinal degenerative disc disease, referred by his general practitioner. His medical history included pulmonary sarcoidosis, hypertension, lymph proliferative disorder, and gastro-oesophageal reflux disease. There were no significant cardiac background or cardiovascular risk factors. Pulmonary sarcoidosis had been diagnosed in the 1990s after a mediastinal lymph node biopsy showed granulomas with central fibrosis. He initially received high-dose corticosteroids, later tapered to prednisolone 5mg daily. He had periodic respiratory evaluations, and his recent review indicated respiratory stability. He had a history of smoking but quit in 1990 and no significant family history of cardiovascular disease.
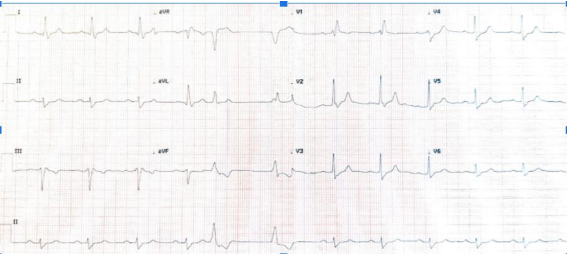
The pre-operative electrocardiogram (ECG)(Figure1) revealed sinus rhythm with a right bundle branch block, left axis deviation, occasional premature ventricular complexes, prolonged PR interval, and QRS duration abnormalities. His only prior echocardiogram in 2011 showed mild left ventricular hypertrophy, septal wall thickening, an ejection fraction of approximately 40%, and mild to moderate mitral regurgitation.
During anaesthesia induction, he experienced a brief episode of monomorphic ventricular tachycardia with loss of output, which spontaneously resolved. He received calcium gluconate and intravenous hydrocortisone. Subsequent episodes of ventricular tachycardia occurred, and magnesium was administered. On day 1 post-operatively, the Cardiology team evaluated him; he was hemodynamically stable but hypertensive. Laboratory tests showed elevated troponin T levels. The suspicion of cardiac sarcoidosis arose, and the patient was started on metoprolol.
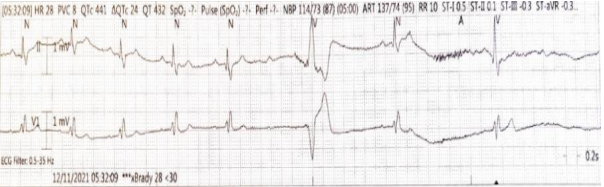
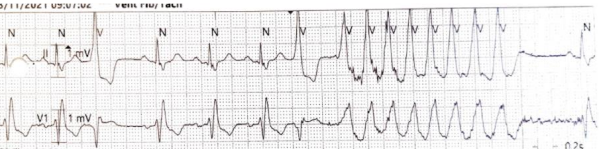
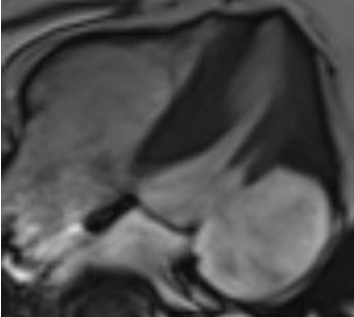
Despite electrolyte optimization, ventricular arrhythmias persisted, and he experienced bradycardia episodes( Figure 2,3). An echocardiogram( Figure 4) revealed cardiac abnormalities, including an aneurysmal basal posterolateral segment, akinesis in various segments, and a reduced ejection fraction. Cardiac MRI (Figure 5) was subsequently performed and showed a wide-necked out pouching from the basal anterolateral and inferolateral left ventricular wall. This was associated with myocardial thinning, severe dyskinesia, and near transmural sub-endocardial late gadolinium enhancement, resembling ischemia more than sarcoidosis.
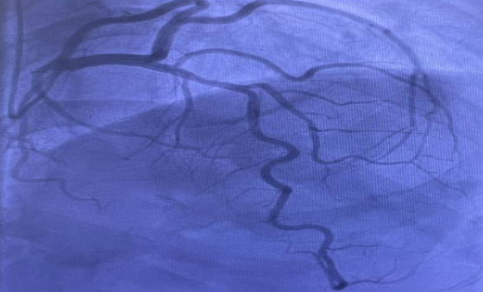
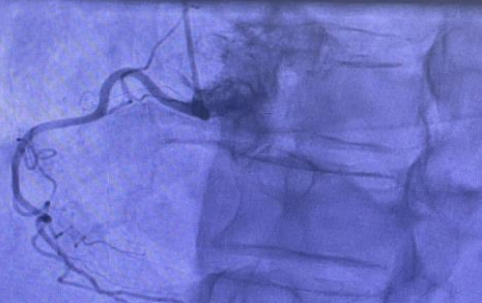
Coronary angiography (Figure 6) confirmed minor disease in one artery but no significant coronary artery disease. Despite this, the cardiac MRI findings were most suggestive of an ischemic aetiology (left circumflex territory myocardial infarction) rather than sarcoidosis.
Following careful consideration, an implantable cardioverter defibrillator (ICD) was inserted, given the patient's non-ischemic cardiomyopathy, ventricular arrhythmias, and bradycardia episodes. The ICD also served as a pacemaker back-up. No complications arose, and the patient was discharged with medications. Follow-up included outpatient whole-body FDG PET imaging, which showed adenopathy in the hilum and mediastinum characteristic of sarcoid. However, there was no FDG-avid uptake in the heart or lungs, indicating prior sarcoidosis without current activity. No immunosuppressant up-titration was required based on these findings.
Figure 1:Pre-operative electrocardiogram (ECG) showing sinus rhythm, with a right bundle branch block, left axis deviation, occasional premature ventricular complexes, a borderline prolonged PR interval of 197ms and a QRS duration of 120ms.
Figure 2:Rhythm strip of the telemetry revealing a short run of severe bradycardia with ventricular escape beats.
Figure 3: Short run of ventricular tachycardia picked up on telemetry whilst the patient was in the coronary care unit.
Figure 4 Transthoracic echo (TTE) showing an aneurysmal basal posterolateral segment.
Figure 5 Cardiac MRI (CMR) showing outpouching from the basal anterolateral and inferolateral left ventricular wallwith associated myocardial thinning, severe dyskinesia and near transmural sub-endocardial late gadolinium enhancement.
Figure 6:Coronary angiogram showed focal minor disease in the mid left anterior descending artery (10% stenosis), but was otherwise entirely normal i.e., there was no significant coronary artery disease.
Discussion
Patients with cardiac sarcoidosis face an increased risk of arrhythmias and sudden cardiac death (6). Predominantly, they experience conduction disorders, such as atrioventricular block, attributed to inflammation and fibrosis affecting the cardiac conduction system. Right bundle branch block may signify initial cardiac sarcoidosis in those previously diagnosed with extra cardiac disease (7). Ventricular tachycardia ranks as the second most common arrhythmia in cardiac sarcoidosis and, when it appears as the initial symptom, carries a notable mortality risk. Atrial arrhythmias, albeit less frequent, have been observed in up to 36% of cases, with atrial fibrillation being the most prevalent among them (6).
Sarcoidosis, often underestimated as an underlying cause, is a recognized contributor to heart failure (8). Granulomatous infiltration of the myocardium leads to fibrosis, resulting in both systolic and diastolic dysfunction. The presence of atrioventricular block and/or ventricular tachycardia in individuals with sarcoidosis signifies a heightened risk of concurrent or future heart failure development (9). Furthermore, these cardiac conduction abnormalities, along with a history of ventricular tachycardia, markedly heighten the risk of sudden cardiac death, which can even serve as the initial and sole manifestation of cardiac sarcoidosis (10).
For patients with established biopsy-proven extra cardiac sarcoidosis, screening for cardiac sarcoidosis typically involves a combination of a cardiac history assessment, electrocardiogram (ECG), and echocardiogram. The presence of abnormalities in any of these aspects warrants further investigation with cardiac imaging modalities like cardiac MRI and/or FDG-PET scans. Indicative findings for potential cardiac sarcoidosis encompass cardiac symptoms such as palpitations, pre-syncope, or syncope, abnormal ECG patterns such as bundle branch blocks, unexplained Q waves in multiple leads, second or third-degree atrioventricular block, and non-sustained ventricular tachycardia. Additionally, abnormal echocardiogram findings, including regional wall motion abnormalities, ventricular wall aneurysms, or a left ventricular ejection fraction below 40%, raise suspicion of cardiac sarcoidosis. Absence of significant findings in these categories suggests a low likelihood of cardiac sarcoidosis (11).
Diagnosing cardiac sarcoidosis is challenging due to its varied and sometimes clinically silent presentation, coupled with imperfect diagnostic modalities (12). Early detection is crucial since heart failure, arrhythmias, and sudden cardiac death risks increase as it progresses (13). Diagnosis hinges on demonstrating cardiac involvement, traditionally requiring endomyocardial biopsy. However, this method's sensitivity is limited (less than 20%) due to the focal nature of cardiac involvement and associated procedural risks, necessitating advanced multimodal imaging for a contemporary diagnosis (14).
The 2016 JCS guidelines introduced a pathway for diagnosing isolated cardiac sarcoidosis without biopsies (12). This approach permits a cardiac sarcoidosis diagnosis via a clinical method in cases where clinical findings strongly suggest cardiac involvement, alongside a positive extra cardiac biopsy confirming sarcoidosis. Notably, a clinical diagnosis can be made even without a positive extra cardiac biopsy if specific criteria are met, including clinical findings suggestive of cardiac involvement, pulmonary or ophthalmic sarcoidosis, and at least two of five characteristic laboratory findings of sarcoidosis. Major and minor criteria further categorize clinical findings strongly suggestive of cardiac involvement (5).
Cardiac MRI with late gadolinium enhancement (LGE) is the preferred modality to diagnose cardiac sarcoidosis, indicating scar tissue presence, with certain LGE patterns suggesting it (15). FDG-PET can identify active inflammation through focal uptake (13).
Differential diagnosis includes myocardial infarction with non-obstructive coronary artery disease (MINOCA). The presence of a left ventricular aneurysm, characteristic of cardiac sarcoidosis, strongly supports this diagnosis. Ventricular aneurysms are rare in MINOCA, and patient profiles differ (20).
Coronary angiography may be considered based on MRI and/or FDG-PET findings (13).
Immunosuppressant, mainly corticosteroids, is the primary treatment for active cardiac sarcoidosis (21). Steroid-sparing agents can be effective alone or with steroids to minimize side effects (5). Biologic agents are an option for steroid-resistant cases (21).
ICD implantation is recommended by the Heart Rhythm Society (HRS) in specific situations (11, 13).
Diagnosing cardiac sarcoidosis is challenging due to its diverse and sometimes asymptomatic clinical presentation. The 2014 HRS Consensus Statement highlights the limitations of existing diagnostic modalities, particularly the low sensitivity of endomyocardial biopsy (less than 20%) due to the focal nature of cardiac involvement and associated risks. However, the 2014 HRS Consensus Statement acknowledges that there was a historical limitation in the diagnostic guidelines, particularly the lack of provisions for diagnosing isolated cardiac sarcoidosis. Subsequent to the publication of the 2016 JCS guidelines, it became possible to diagnose isolated cardiac sarcoidosis without the necessity of endomyocardial biopsy or extra cardiac biopsy. The 2014 HRS Expert Consensus Statement provides valuable insights into the diagnosis and management of arrhythmias associated with cardiac sarcoidosis, emphasizing the challenges in diagnosis, the significance of cardiac conduction abnormalities and arrhythmias, and the role of advanced imaging modalities in achieving a contemporary diagnosis (11).
In summary, while both the 2014 HRS Expert Consensus Statement and the JCS 2016 guideline address the diagnosis and management of cardiac sarcoidosis, the JCS 2016 guideline introduced significant changes, particularly in diagnosing isolated cardiac sarcoidosis without the need for biopsies, incorporating FDG-PET imaging, and providing more detailed treatment and device therapy recommendations. These updates aimed to improve the diagnosis and management of cardiac sarcoidosis, reflecting advances in medical knowledge and technology.
Table 1
|
JCS Criteria for clinical diagnosis in absence of a positive extra-cardiac biopsy |
|
Clinical findings strongly suggestive of cardiac involvement |
|
Clinical findings strongly suggestive of pulmonary or ophthalmic sarcoidosis |
|
At least two of five characteristic laboratory findings of sarcoidosis are present: 1.Bilateral hilar lymphadenopathy 2.High serum angiotensin-converting enzyme (ACE) activity or elevated serum lysozyme levels 3.High serum soluble interleukin-2 receptor (sIL-2R) levels 4.Significant tracer accumulation in 67Ga citrate scintigraphy or 18F-FDG PET 5.A high percentage of lymphocytes with a CD4/CD8 ratio of >3.5 in BAL fluid
|
Table 2
|
Criteria for cardiac involvement |
|
1.Major criteria: |
|
(a) High-grade atrioventricular block (including complete atrioventricular block) or fatal ventricular arrhythmia (e.g., sustained ventricular tachycardia, and ventricular fibrillation). (b) Basal thinning of the ventricular septum or abnormal ventricular wall anatomy (ventricular aneurysm, thinning of the middle or upper ventricular septum, regional ventricular wall thickening). (c) Left ventricular contractile dysfunction (left ventricular ejection fraction less than 50%) or focal ventricular wall a synergy. (d) 67Ga citrate scintigraphy or 18F-FDG PET reveals abnormally high tracer accumulation in the heart. (e) Gadolinium-enhanced MRI reveals delayed contrast enhancement of the myocardium |
|
2. Minor criteria : |
|
a)Abnormal ECG findings: Ventricular arrhythmias (nonsustained ventricular tachycardia, multifocal or frequent premature ventricular contractions), bundle branch block, axis deviation, or abnormal Q waves. b)Perfusion defects on myocardial perfusion scintigraphy (SPECT). c)Endomyocardial biopsy: Monocyte infiltration and moderate or severe myocardial interstitial fibrosis. |
Conclusion:
Cardiac sarcoidosis is likely to be under diagnosed in clinical practice, underscoring the importance of maintaining a high level of suspicion when the clinical context warrants. In this particular case, the suspicion for cardiac sarcoidosis was appropriately raised based on the clinical events that transpired. This case brings attention to the uncommon occurrence of cardiac sarcoidosis with a sub endothelial distribution, a presentation that can mimic ischemic conditions.
Moreover, our case emphasizes the pivotal role of cardiac MRI in identifying myocardial scar, as indicated by late gadolinium enhancement (LGE). This diagnostic capability is further enhanced by the complementary use of CT-PET imaging, which aids in detecting evidence of active sarcoidosis within the myocardium. Identifying active sarcoidosis through CT-PET is of paramount importance as it has significant implications for determining the appropriate treatment regimen, particularly the use of immunosuppressive agents.
The presence of monomorphic ventricular tachycardia and the absence of cardiac FDG uptake on PET-CT collectively suggest that scar tissue was the focal point of the arrhythmia in this case. Furthermore, this case underscores the critical role of a robust multidisciplinary approach in managing complex cases such as this, optimizing patient care and outcomes. Additionally, it highlights how advances in non-invasive imaging have greatly contributed to enhancing clinical practice.
References
1. ATS/ERS/WASOG statement on sarcoidosis.
2.Birnie DH. Cardiac Sarcoidosis. Semin Respir Crit Care Med. 2020 Oct 1;41(5):626–40.
3. Mehta D, Lubitz SA, Frankel Z, Wisnivesky JP, Einstein AJ, Goldman M, et al. Cardiac involvement in patients with sarcoidosis: Diagnostic and prognostic value of outpatient testing. Chest. 2008;133(6):1426–35.
4. Okada DR, Bravo PE, Vita T, Agarwal V, Osborne MT, Taqueti VR, et al. Isolated cardiac sarcoidosis: A focused review of an under-recognized entity. Vol. 25, Journal of Nuclear Cardiology. Springer New York LLC; 2018. p. 1136–46.
5. Terasaki F, Azuma A, Anzai T, Ishizaka N, Ishida Y, Isobe M, et al. JCS 2016 guideline on diagnosis and treatment of cardiac sarcoidosis ? digest version ?. Vol. 83, Circulation Journal. Japanese Circulation Society; 2019. p. 2329–88.
6. Okada DR, Smith J, Derakhshan A, Gowani Z, Misra S, Berger RD, et al. Ventricular arrhythmias in cardiac sarcoidosis. Circulation [Internet]. 2018 Sep 18 [cited 2022 Jan 17];138(12):1253–64. Available from: https://www.ahajournals.org/doi/abs/10.1161/CIRCULATIONAHA.118.034687
7. Ashraf I, Peck MM, Maram R, Mohamed A, Crespo DO, Kaur G, et al. Association of Arrhythmias in Cardiac Amyloidosis and Cardiac Sarcoidosis. Cureus [Internet]. 2020 Aug 18 [cited 2022 Jan 17];12(8). Available from: /pmc/articles/PMC7497218/
8. Birnie DH, Kandolin R, Nery PB, Kupari M. Cardiac manifestations of sarcoidosis: diagnosis and management. Eur Heart J [Internet]. 2017 [cited 2022 Jan 17];38(35):2663–70. Available from: https://pubmed.ncbi.nlm.nih.gov/27469375/
9.Rosenthal DG, Fang CD, Groh CA, Nah G, Vittinghoff E, Dewland TA, et al. Heart failure, atrioventricular block, and ventricular tachycardia in sarcoidosis. J Am Heart Assoc [Internet]. 2021 [cited 2022 Jan 17];10(5):1–16. Available from: https://www.ahajo
10. Challenges in Cardiac and Pulmonary Sarcoidosis | Elsevier Enhanced Reader [Internet]. [cited 2022 Jan 17]. Available from: https://reader.elsevier.com/reader/sd/pii/S073510972036410X?token=FCB9898413CBBBF3C3FC4141B3A2B20E60EC6450E9A325F329822BCF3683F8CF7FDB0BB083E113E5E0D16016EFBF4834&originRegion=eu-west-1&originCreation=20220117184554
11. Birnie DH, Sauer WH, Bogun F, Cooper JM, Culver DA, Duvernoy CS, et al. HRS expert consensus statement on the diagnosis and management of arrhythmias associated with cardiac sarcoidosis. Heart Rhythm. 2014;11(7):1304–23.
12. Sharma A, Okada DR, Yacoub H, Chrispin J, Bokhari S. Diagnosis of cardiac sarcoidosis: an era of paradigm shift. 2020 [cited 2022 Jan 18];34:87–93. Available from: https://doi.org/10.1007/s12149-019-01431-z
13. Markatis E, Afthinos A, Antonakis E, Papanikolaou IC. Cardiac sarcoidosis: diagnosis and management. Rev Cardiovasc Med. 2020;21(3):321–38.
14. Kawai H, Sarai M, Kato Y, Naruse H, Watanabe A, Matsuyama T, et al. Diagnosis of isolated cardiac sarcoidosis based on new guidelines. ESC Heart Fail. 2020 Oct 1;7(5):2662–71.
15. Blankstein R, Waller AH. Evaluation of Known or Suspected Cardiac Sarcoidosis. Circ Cardiovasc Imaging [Internet]. 2016 Mar 1 [cited 2022 Dec 19];9(3). Available from: https://www.ahajournals.org/doi/abs/10.1161/CIRCIMAGING.113.000867
16. Okasha O, Kazmirczak F, Chen KHA, Farzaneh-Far A, Shenoy C. Myocardial Involvement in Patients With Histologically Diagnosed Cardiac Sarcoidosis: A Systematic Review and Meta-Analysis of Gross Pathological Images From Autopsy or Cardiac Transplantation Cases. J Am Heart Assoc [Internet]. 2019 May 21 [cited 2023 Mar 19];8(10). Available from: https://pubmed.ncbi.nlm.nih.gov/31070111/
17. Sekhri V, Sanal S, DeLorenzo LJ, Aronow WS, Maguire GP. Cardiac sarcoidosis: a comprehensive review. Arch Med Sci [Internet]. 2011 Aug [cited 2023 Mar 19];7(4):546–54. Available from: https://pubmed.ncbi.nlm.nih.gov/22291785/
18. Pedrotti P, Ammirati E, Bonacina E, Roghi A. Ventricular aneurysms in cardiac sarcoidosis: From physiopathology to surgical treatment through a clinical case presenting with ventricular arrhythmias. Int J Cardiol [Internet]. 2015 May 1 [cited 2023 Mar 19];186:294–6. Available from: https://pubmed.ncbi.nlm.nih.gov/25828139/
19. Bil J, Buller P, Gil RJ, Gromadzi?ski L, Onichimowski D, Jalali R, et al. Acute Complications in Patients with Myocardial Infarction with Non-Obstructive Coronary Arteries: A Systematic Review with Special Focus on Mechanical Complications. Rev Cardiovasc Med [Internet]. 2022 Dec 2 [cited 2023 Mar 19];23(12):393. Available from: https://www.imrpress.com/journal/RCM/23/12/10.31083/j.rcm2312393/htm
20. Gudenkauf B, Hays AG, Tamis-Holland J, Trost J, Ambinder DI, Wu KC, et al. Role of Multimodality Imaging in the Assessment of Myocardial Infarction With Nonobstructive Coronary Arteries: Beyond Conventional Coronary Angiography. J Am Heart Assoc [Internet]. 2022 Jan 4 [cited 2023 Mar 19];11(1). Available from: https://pubmed.ncbi.nlm.nih.gov/34970915/
21. Gilotra N, Okada D, Sharma A, Chrispin J. Management of cardiac sarcoidosis in 2020. Arrhythm Electrophysiol Rev. 2021;9(4):182–8.