Comparison of the Effectiveness and Reliability of Oxygen Delivery and EtCO2 Monitoring in 3 EtCO2 Nasal Sampling Cannulas
Comparison of the Effectiveness and Reliability of Oxygen Delivery and EtCO2 Monitoring in 3 EtCO2 Nasal Sampling Cannulas
Dr. Jennifer Riggs, PhD, RRT* 1
*Correspondence to: Dr. Jennifer Riggs, PhD, RRT.
Copyright
© 2023 Dr. Jennifer Riggs. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 29 September 2023
Published: 16 October 2023
Comparison of the Effectiveness and Reliability of Oxygen Delivery and EtCO2 Monitoring in 3 EtCO2 Nasal Sampling Cannulas
Introduction
Monitoring patents' end-tidal CO2 (EtCO2) in various settings throughout the care continuum is the standard of care. While pulse oximetry monitors a patient’s oxygenation status, capnography monitors EtCO2 throughout the breathing cycle. Capnography is an effective method to diagnose early respiratory depression and other airway disorders, leading to a reduction in serious complications. Deitch and associates showed capnography displayed evidence of respiratory depression to hypoxia 60 seconds (range 5 to 240 seconds) before pulse oximetry. (1)
There are a multitude of indications for capnography that include both pre-hospital and various locafions within the hospital. While this list is not exhaustive, indications include:
- Monitoring ventilation / respiratory status in ICU, PACU, ER, OR, Endoscopy, and pre-hospital environments
- Confirmation of endotracheal tube placement
- Monitoring patients during pain management, or moderate to deep sedation
- Monitoring the effectiveness of chest compression and return of spontaneous circulation (ROCS)
Importance of Capnography
More than 50 medical societies worldwide have established guidelines and standards for using capnography to monitor the ventilation status of patients undergoing general anesthesia, sedation, or analgesia, and as a method to verify endotracheal tube placement.
Capnography use combined with pulse oximetry was introduced by the American Society of Anesthesiologists (ASA) in the mid-1980s, based on a review of adverse events that indicated capnography together with pulse oximetry could have prevented 93% of anesthesia mishaps that contributed to anesthetic morbidity and mortality. According to the ASA Standards of Basic Anesthetic Monitoring, "During moderate or deep sedation the adequacy of ventilation shall be evaluated by continual observation of qualitative clinical signs and monitoring for the presence of exhaled carbon dioxide unless precluded or invalidated by the nature of the patient, procedure or equipment" (2)
The AAGBI (Association of Anesthetists of Great Britain and Ireland) (Association of Anesthetists of Great Britain and Ireland)) 2021 Guidelines state, “General anesthesia requires minimum monitoring of ECG, SpO2, NIBP, and capnography, which should be checked for correct function and begun before induction of anesthesia and continue throughout anesthesia, transfer to the post-anesthesia care unit (PACU) and recovery."(3) Continuous EtCO2 can be used to monitor patents recovering from surgery to detect hypoventilation. One study showed continuous EtCO2 was 6 times more effective than pulse oximetry at detecting respiratory depression (4). The sensitivity of capnometry to detect respiratory events is superior to that of clinical examination findings or pulse oximetry. During the transfer between the operating room and PACU, PEtCO2, monitoring allows early detection of hypoventilation and residual sedation, especially by respiratory rate measurements. The use of capnography in the PACU by trained nurses led to the recognition of earlier airway obstruct on and the reduction of these complications. (5) The most common respiratory adverse events detected by capnography included hypocapnia, apnea, tachypnea, bradypnea, and hypoxemia. These data indicate that respiratory adverse events are frequent in the PACU and that the addition of capnography to pulse oximetry monitoring, including ut1lization of integrated pulmonary index (IPI), gives potentially clinically useful information on the respiratory status. (6)
For patents having endoscopic procedures, the ASA issued a statement: "Monitoring for exhaled carbon dioxide should be conducted during endoscopic procedures in which sedation is provided with propofol alone or in combination with opioids and/or benzodiazepines, and especially during procedures on the upper gastrointestinal tract. Careful attention to airway management must be provided during complex upper endoscopic procedures and procedures performed in the prone position where ventilatory monitoring, airway maintenance, and resuscitation may be especially difficult" (7)
Regarding sedation in the Emergency Department, there is an update to the guideline from 2018, Clinical Practice Guideline for Emergency Department Procedural Sedation with Propofol: 2018 Update; "Monitoring: Continuous cardiac monitoring, capnography, and pulse oximetry required for deep sedation, with respiratory rate and blood pressure recoded at least every 5 min. Supplemental oxygen is recommended for both adult and pediatric patents undergoing propofol sedation”. (8)
The American Society of Interventional Pain Physicians (ASIPP) Guidelines for Sedation and Fasting Status of Patents Undergoing Interventional Pain Management Procedures (2019) adopted the ASA-published standards for monitoring patents under sedation, regardless of location or setting of the procedure. These standards include blood pressure monitoring, assessment of real-Anne EKG, temperature measurement, pulse oximetry, and continuous quantitative EtCO2. The omission of end-tidal CO2 monitoring can significantly delay the identification of hypoventilation and appropriate airway support, and result in catastrophic complications including anoxic brain injury and even death. Supplemental oxygen by nasal cannula is also recommended, particularly for deep sedation. (9) An observational study detected one or more opioid-induced respiratory depression episodes in 614 (46%) of 1335 patents on the general care floor. The authors concluded that a tool for respiratory depression risk assessment and continuous monitoring with capnography and oximetry of patents identified as high risk for respiratory depression may improve their safety when parenteral opioid analgesia cannot be avoided (10). During hyperventilation, capnography values change instantaneously giving clinicians an immediate warning of the patient's declining respiratory status. An enhanced monitoring program with capnography is an effective intervention to reduce transfers of surgical spine patents to the ICU due to opioid-induced respiratory depression. (11)
Importance of Oxygen (Oz) delivery
When monitoring EtCO2 utilizing a cannula that monitors EtCO2 as well as delivers oxygen, there are several parameters to be considered. Obviously, one is end tidal CO2 and another oxygen saturation (SpO2). Since these patents are typically receiving analgesics or have comorbidities, the ability to deliver adequate oxygen cannot be overstated.
Guidelines regarding monitoring of exhaled CO2, also recommend delivery of supplemental O2 In the study by Kuroe et al, (12) the incidence of respiratory compromise was 5.9 % in elderly patents and 9.0 % in obese patents, with the most frequent cause being hypoxemia. Therefore, it is paramount to utilize a sampling cannula that not only effectively monitors exhaled carbon dioxide, but also adequately delivers oxygen.
 In a previous study by Ebert (13) different nasal cannula designs were tested for oxygen delivery and monitoring of EtCO2. The study evaluated the Hudson Softec Bi FIo #1845, Medline Mac -Safe HCW #4561, Oridion Micro stream Filter Line #006912, and the Salter Labs #4707 at flow rates of 1 LPM, 2 LPM, and
In a previous study by Ebert (13) different nasal cannula designs were tested for oxygen delivery and monitoring of EtCO2. The study evaluated the Hudson Softec Bi FIo #1845, Medline Mac -Safe HCW #4561, Oridion Micro stream Filter Line #006912, and the Salter Labs #4707 at flow rates of 1 LPM, 2 LPM, and
4 LPM. The author concluded that for oxygen delivery, the multi-vented, blow-by facepiece design resulted in lower O2 delivery at higher flow rates. The divided nasal cannula design (Salter Labs) consistently achieved higher pharyngeal O2 percentages. Improved O2, delivery is highly beneficial during moderated sedation or when needing to deliver nigh FiO2 to maintain oxygen saturation.
Study Design and Protocol
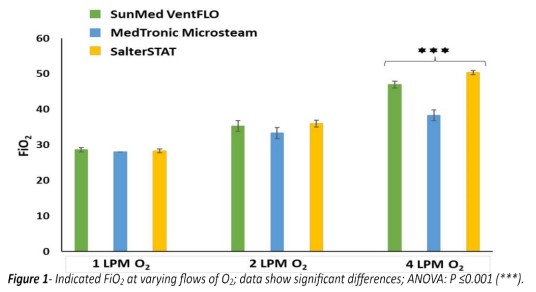
There are many studies evaluating the efficacy of nasal sampling cannulas to monitor EtCO2 Hypoxemia is the most frequent cause of respiratory compromise; therefore, the purpose of this study was to compare the EtCO2 accuracy and oxygen delivery of 3 EtCO2 / O2 nasal sampling cannulas with a single sidestream bedside capnography monitor. Three EtCO2 / O2, nasal cannulas design with a reflective end connector (SunMed VentFlo #5107F-SE, Medtronic Microstream Advance #MVANO and Salter STAT 4MSF3-7-6) were tested at 3 different O2 flowrates, 1LPM, 2LPM, and 4 LPM. In addition, the rise Anne was evaluated as that can impact how well EtCO2 is monitored at higher minute ventilation. study outcomes were (1) FiO2 delivery at a variety of O2 flows, (2) EtCO2 sampling accuracy at a variety of O2 flows, and (3) rise time at a variety of O2 flows.
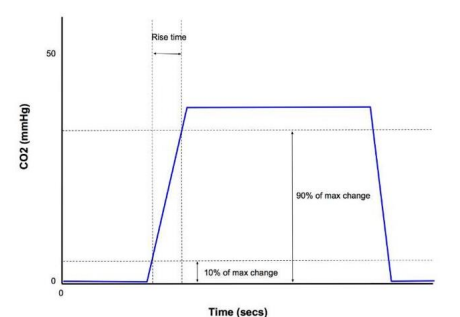
The test procedure used an oxygen source to deliver Ot to the simulated patient and a known baseline EtCO2 level of 38 mmHg. Test samples included 3 cannulas of each design (n=9). Readings were taken after allowing the system to equilibrate for 3 minutes at each flow rate setting, then a full inhalation exhalation waveform to determine the EtCO2 and FiO2 measurements. The waveform was used to determine the rise time, defined as the amount of Anne it takes the measured CO2 to rise from 10% to 90% of the known EtCO2, value. For accurate EtCO2 measurements, the CO2, transducer needs to respond quickly to a change in the level of CO2.
Results
The data obtained were analyzed by using the Excel program. All data were reported as mean + SD. Descriptive data are presented as the median, frequency, and percentage. Statistical analyses were performed using ANOVA.
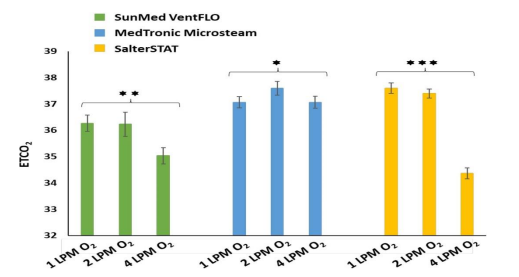
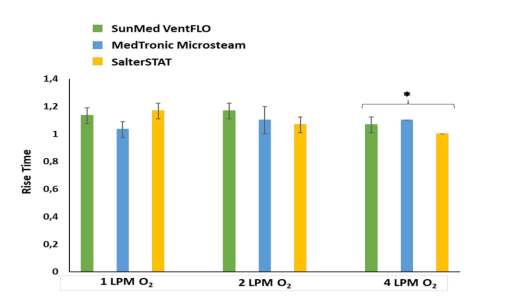
There was no significant difference in the FiO2 delivered at flow rates of 1 LPM and 2LPM. The VentFlo and SalterSTAT had significantly higher FiO2 at 4 LPM (Figure 1 & Table 1). At the flow rates of 1 LPM and 2 LPM, there was no significant change in the EtCO2 value. The Medtronic Advance EtCO2 value was the least affected by increasing the flow rate to 4 LPM. With the increase to 4LPM, the VentFlO EtCO2 mean value dropped from 36.3 to 35.0. The SalterSTAT EtCO2 value dropped from a mean of 37.6 to 34.4 (Figure 2 and Table 2). There was no significant difference in the rise time between the 3 cannulas at the varying flow rates (Figure 3 and Table 3).
Discussion
Supplemental oxygen is frequently used in procedural sedation and pain management. The ability to deliver oxygen and monitor EtCO2 has been shown to improve patient safety. Corbett evaluated the impact of capnography on the safety of procedural sedation. The primary endpoint was defined as the total incidence of respiratory and cardiac adverse events. Supplementary oxygen was used in 62% (n=864) of the procedures. Respiratory adverse events were defined as oxygen desaturation (75-90%) for < 60 seconds, and severe oxygen desaturation (<75 at any time). After implementing capnography, the incidence of adverse events dropped 43.2% (p≤0.05). 147 adverse events occurred during 666 procedures without capnography compared with 93 adverse events that occurred during 735 procedures with capnography. (15) The SalterSTAT divided cannula delivered significantly higher FiO2 at 4 LPM, which could make a difference in a respiratory-comprised patent. (12)
If the patient has a normal respiratory function, the difference between EtCO2 and PaCO2 (partial pressure of COC) is 2 mmHg to 5 mmHg, and usually, the PaCO2 is greater than the EtCO2 value. However, the PaCO2: EtCO2, gradient increases in situations such as decreased lung perfusion, pulmonary embolism, dead space ventilation, and cardiac arrest. Even if the PaCO2 : EtCO2 gradient is wide, the EtCO2 value can be used as a trending tool to monitor and alert clinicians of changes in the patent's ventilation status.
The SalterSTAT cannula has a divided facepiece, oxygen is delivered to one nare and CO2 is sampled from the other nare. The Medtronic Advance and VentFlo deliver On cloud outside the nares via small holes in the facepiece, while the 2 nasal prongs are used to sample CO2. Similar to Ebert's (13) findings, the "blow-by" design had less impact on the EtCO2 value as O2 flow was increased. In this study, increasing the flow from 1 LPM to 2 LPM did not have a significant impact on the EtCO2 value for all 3 cannulas. When the flow was increased to 4 LPM, the Microstream Advance and VentFlo cannulas had the most stable EtCO2 values (37.60 ± 0.26 to 37.07 ± 0.23 and 36.27 ± 0.31 to 35.0 ± 0.31, respectively). The SalterSTAT EtCO2 value dropped (37.60 ± 0.20 to 34.37 ± 0.21), although this was statistically significant, it is not considered clinically significant.
The CO2, analyzer’s response time, which includes the transit time and the rise Anne, must be sufficiently fast for accuracy. Rise time is defined as the Anne required to change from 10 % to 90 % of the final EtCO2, value (Figure 1) (16) When the respiratory rate is high, faster rise times are recommended for accuracy. The rise time between the 3 cannulas was similar at all flow rate.
Study Limitation
This study has certain limitations. The first of these is that a bench trial does not capture the various clinical conditions that can impact the EtCO2 value and waveform. Multiple factors can affect FiO2, delivery and EtCO2 values, specifically mouth breathing, nasal anatomy, tidal volume, and respiratory rate. These factors, in addition to V/Q mismatches and oxygen flow rate, have a direct impact on EtCO2, values. The second is that only nasal EtCO2, sampling was evaluated. EtCO2 cannula with oral and nasal sampling have different results, especially simulating mouth breathing. Another limitation is that bench study was based on normal simulated breathing. Additional studies simulating different breathing patterns and disease states may have an impact on the results. A limited number of cannulas tested, and data points is another limitation of the study. Additional clinical trials on human subjects are recommended.
All three cannulas designed and studied had an adequate rise time and provided EtCO2 monitoring that would alert clinicians to a decline in ventilation. The key difference in this study is the ability to deliver a higher FiO2, at 4 LPM. Acco ding to Kuroe et al (5), hypoxemia is the most frequent respiratory compromise. In this clinical situation efficiency of O2 delivery could make a difference.
Figure 4. Rise time
References
1. Deitch K, Miner J, Chudnovsky CR, Dominici P, Latta D. Does end-udal CO2 monitoring during emergency department procedural sedation and analgesia witn propofol decrease the incidence of hypoxic events? A randomized, controlled trial. Ann Emerg Med. 2010 Mar;55(3):258-64. doi: 10.1016/j.annemergmed.2009.07.030. Epub 2009 Sep 24. PMID: 19783324.
2. https:www.asah.orstandards-and-sidelinesstandards-for-basic-anesthetic-monitoring Klein AA, et al. Recommendations or standards o monitoring during anesthesia and recovery 2021: Guideline from the Association of Anesthetists. Anesthesia. 2021 Sep;76(9):1212-1223. doi: 10.1111/anae.15501. Epub 2021 May 20. PMID: 34013531.
3. Rackley CR. Monitoring Dur”ng Mechanical Venfilafion. Respir Care. 2020 Jun;65(6):832-846. doi: 10.4187/respcare.07812. PMID: 32457174.
4. Potvin J, Etchebarne I, Soubiron L, Biais M, Roullet S, Nouette-Gaulain K. Effects of capnometry monitoring during recovery in the post-anesthesia care unit: a randomized controlled trial in adults (CAPNOSSPI). J Clin Monit Comput. 2022 Apr;36(2):379 385. doi: 10.1007/s10877 021 00661 9. Epub 2021 Feb 7. PM ID: 33550546.
5. Chung F, Wong J, Mestek ML, Niebel KH, Lichtenthal P. CharacterizaVon of respiratory compromise and the potenflal clinical ufllity of capnography in the post-anesthesia care unit: a blinded observafional trial. J Clin Monit Comput. 2020 Jun;34(3):541 551. doi: 10.1007/s10877 019 00333 9. Epub 2019 Jun 7. PMID: 31175500; PMCID: PMC7205778.
7. https://nunem.com/wp-content/uploads/2O21/06/7-Procedural Sedation.pdf
8. Kaye AD, Jones MR, Viswanath 0, Candido KD, Boswell MV, Soin A, Senapafl M, Harned ME, Simopoulos TT, Diwan S, Albers SL, Datta S, Falco FJ, Manchikanti L. ASIPP Guidelines for Sedation and Fasting Status of Patients Undergoing Interventional Pain Management Procedures. Pain Physician. 2019 May;22(3):201-207. PMID: 31151329.
9. Khanna AK, et al. Prediction of Opioid-I nduced Respiratory Depression on Inpatient Wards Using Cont nuous Capnography and Oximetry: An International Prospective, Observational Trial. Anesth Analg. 2020 Oct;131(4):1012-1024. doi: 10.1213/ANE.0000000000004788. PMID: 32925318; PMCID: PMC7467153.
10. Kozub E, Uttermark A, Skoog R, Dickey W. Prevent ng Postoperative Opioid Induced Respiratory Depression Through Implementation of an Enhanced Monitoring Program. J Healtnc Qual. 2022 Jan-Feb 01;44(1):e7-e14. doi: 10.1097/JHQ.0000000000000322. PMID: 34469926.
11. Kuroe Y, Mihara Y, Okahara S, Ishii K, Kanazawa T, Morimatsu H. An integrated pulmonary index can predict respiratory compromise in high-risk patients in the post-anesthesia care unit: a prospective, observational study. BMC Anesthesia. 2021 Apr 21;21(1):123. doi: 10.1186/s12871-O21-01338-1. PMID: 33882856; PMCID: PMC8059175.
13. https://www.bianaesthesia.org/arflcIe/S0007-0912(17)49247-6/fuI!text
14. Corbett G, et al. Se vice Evaluation of the Impact of Capnography on tne Safety of Procedural Sedaflon. Front Med (Lausanne). 2022 May 6;9:867536. doi: 10.3389/fmed.2022.867536. Erratum in: Front Med (Lausanne). 2022 Aug 05;9:999862. PMID: 35602494; PMCID: PMC9122489.
15. Brunner JX, Westenskow DR. How the rise t1me of ca bon dioxide analyzers influences the accuracy of carbon dioxide measurements. Br J Anaesth. 1988 Nov;61(5):628-38. doi: 10.1093/bja/61.5.628. PMID: 3144999.
16. Piper, D. (2023). End Tidal CO2 and FiO2 Measurements of Three EtCO2 and 02 Del”very Split Cannulas.