Type IV Hypersensitivity Reaction to Surgical Clips – A Case Report
Type IV Hypersensitivity Reaction to Surgical Clips – A Case Report
A. Craveiro*1, M. La Salete Valente1, M. De Jesus Valente1, E. Magalhães1, Rita Lopes2
1.Pulmonology Department, Centro Hospitalar Universitário Cova da Beira, Covilhã, Portugal
2.Department of Cardiothoracic Surgery, Centro Hospitalar Universitário de Coimbra, Portugal
*Correspondence to: A. Cunha-Craveiro, E-mail address: ana-craveiro@live.com.pt
Copyright
© 2023 A. Cunha-Craveiro. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 10 October 2023
Published: 16 November 2023
Abstract
Postoperative Lung Cancer needs to be very accurate and the diferencial diagnosis of tumour recurrence can be very difficult.
Type IV Hypersensitivity reactions to surgical material is a relatively common ocurrence with metals such as niquel, but very rare with Titanium. However that hypothesis should be considered in some contexts.
We report one case where the suspection of tumor recurrence camouflaged the diagnosis of a hypersensitivity reaction.
KEYWORDS: Tumor recorrence; Type IV Hypersensitivity Reaction; Surgical clips; Titanium.
Type IV Hypersensitivity Reaction to Surgical Clips – A Case Report
Introduction
Lung cancer is the leading cause of cancer-related deaths. Along with rapid diagnosis and treatment, it requires careful follow-up (4). However, the monotonous imaging traduction of various conditions can difficult the differential diagnosis, namely of tumour recurrence.
Surgery remains the best option in localized disease and the biocompatibility of surgical materials is a urge concern, with titanium components being the most commonly tolerated (1).
We report a patient with postoperative type IV hypersensitivity reaction to surgical clips used on a pulmonary surgery that mimetized tumour recurrence for a long period.
Case Report
Forty one years old woman, assistant in a nursing home, with the diagnosis of allergic rhinoconjuntivitis and esophageal hernia, previous smoker (CT 7,5 UMA) without other risk inalatory exposures or patological respiratory background that, on June/2015, performed a thoraco-abdomino-pelvic CT-scan for the study of esophageal alteration and in whom was accidentally detected a 3,7cm cavitated lung lesion in the apical segment of the right upper lobe (RUL) and another solid, spiculated and irregular nodule, of 1,1cm, in the same segment but paramediastinal.
Without respiratory symptoms or alterations to the objective examination, she the patient performed a bronchofibroscopy (BF), with bronchoalveolar lavage (BAL) and bronchial aspirate for cytological, micro and mycobacterial and mycological study – which was negative. She did IGRA research and was also negative. For further clarification, one month later, she made a PET/CT – which described metabolic characteristics no suggestive of malignancy, with mild avidity for FDG in the cavitated lesion of RUL (initial SUVmax. of 1,8, with temporal reduction of intensity of SUVmax. latter to 1) and without uptake in the small adjacent nodule.
With normal respiratory functional study, the patient was kept under pulmonology surveillance in consultation with Chest CT-Scan every 6 months. No changes were detected until January 2019, when it was registered a dimensional increase (to 5,2cm) of the cavitated lesion of the RUL, with extension to the mediastinum. The homolateral nodule also increased to 1,7cm. The PET/CT was repeated and again the suspicion was of benignity, with mild glycolytic hypermetabolism in the RUL mass (initial SUVmax 2,2; late SUVmax 2). It was decided to perform Transthoracic Lung Biopsy (TLB) of the lesion on the RUL but it was negative for neoplastic cells (March, 2019).
The clinical case was discussed in a multidisciplinary meeting (MDM) and a surgical approach was proposed. In June of 2019, the patient underwent right upper lobectomy with mediastinal lymphadenectomy, whose anatomopathological (AP) result was compatible with mucinous Adenocarcinoma (ADC) of the Lung, TNM stage: cT2bN0m0 – IIA; pT2N0M0 – IB, with negative molecular (ALK, ROS1, EGFR) and PD-L1 research.
Clinically stable, without weight loss and with PS ECOG of 0, she underwent adjuvant chemotherapy with 4 cycles of oral vinorrelbine and carboplatin, with good tolerance.
In reassessment with Thoracic CT at three months, it was found a right soft tissue mass (2,6 cm) anterolateral to the descending Aorta, right posterolateral in relation to the Esophagus and inferior vena cava (IVC).
In PET/CT one month later, it was possibly to identify several new foci of abnormal FDG uptake, namely in right paramediastinal pleural densification (initial SUVmax of 8.8; late max. of 14.5).
In this context, due to suspicion of disease recurrence/progression, in November of 2019, the patient underwent BF and endobronchial and esophageal endoscopy (EBUS and EUS, respectively). On endoscopic examination, were found extensive inflammatory signs in the right bronchial tree. Ganglion aspiration puncture in positions 8 and 10R were negative for neoplasic origin.
After one month (December of 2019 – 6 month after surgery), it was identified a dense and heterogeneous area in the internal and posterior basal segments of the Right Lower Lobe (RLL), adjacent to the diaphragmatic cisura (of 7,1cm) and with changes of ground glass in the periphery. Associately, a new pulmonary nodule with soft tissue consistency of 2 cm, was found behind the IVC and to the right of the Esophagus.
In few days, the patient started developing clinical symptoms with right pleuritic thoracalgia, dry cough and wheezing. The RLL lesion was approached by BTT and was diagnosticated as Organizing Pneumonia. So, patient started a long scheme of systemic corticosteroids, with progressive clinical improvement and imaging resolution on Chest CT (March of 2020), but maintaining, in successive examinations at 6 and 9 months, the image compatible with a right paraesophageal soft tissue mass (Chest CT on August and November of 2020).
The patient repeated PET/CT (in December of 2020) and presented changes suggestive of malignant etiology – namely with description of hypermetabolic thickening in the right hilar region (4,5 cm), with SUVmax. of 9.
The clinical case was discussed again in MDM and was decided to repeat BF and EBUS. Both exams (performed in January of 2021) were negative for neoplastic cells. It was assumed that the changes were a probable sequelae of surgical intervention and it was decided to maintain active surveillance.
In the following month, the patient reported persistent dry cough and, after another three months, she repeated Thoracic CT-Scan, registering a new dimensional increase in the right upper hilar mass (to 3,1 cm), as well as hilar adenopathy on the right.
After a new MDM, and with the suspicion of locoregional recurrence, the patient performed exeresis of the right parahilar mass, with arterial and bronchial sleeve and lymphadenectomy, in May of 2021. The post-operative recovery was slow, and the patient had hospital discharge under oxygen therapy (1,5L/min, 16h/day) and started a Respiratory Rehabilitation program.
Despite the suspicion of tumour recurrence, the result of PA (June of 2021) of the surgical specimen excluded neoplastic disease at the level of the bronchial resection line, right paratracheal lymph nodes (2R, 4R) and ganglion stations 7 and 8, with identification of extensive histiocytosis and areas with mixed inflammatory infiltration, foamy histiocytes, and calcified secretions.
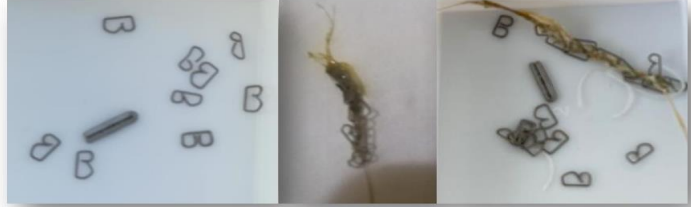
The patient restarted corticotherapy and did also empirical antibiotics. However, in few days, she developed an intense clinical worsening, with incoercible cough, no response to medical therapy and episodes of elimination of surgical clips by mouth (Figure 1).
Figure 1: Surgical clips expelled through the mouth with cough
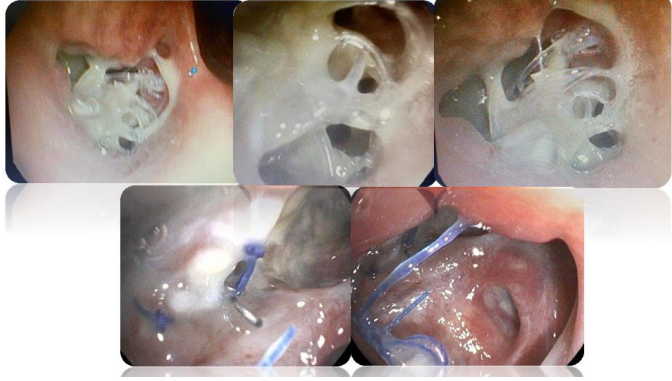
BF was repeated (July of 2021) and, in addition of exuberant endobronchial inflammatory signs, it was observed a heterogeneous mass at the right bronchial tree, with visualization of surgical clips at the entrance of the right main bronchus (Figure 2).
Figure 2: BF images of right bronchial tree in which are seen surgical clips and a mass in the entrance of the main right bronchus
In the following days, the clinical worsening was accentuated, with fatigue for small efforts, frequent productive cough and episodic hemoptoic sputum. The case was again discussed in MDM and was equacionated the hypothesis of type IV hypersensitivity reaction to the surgical material. After revision of its constitution (titanium, nickel, palladium), skin sensitivity tests were performed (July of 2021), which at 96h of reading were positive for all the metals involved – including titanium.
Because of the potential risks involved, thoracic surgeons decided to do not re-operate the patient. So, after another MDM, the corticosteroid therapy was increased, and the patient started showing progressive clinical improvement.
At the time this report was written, the patient was clinically stable, already without corticotherapy and in pulmonology consultation follow-up.
Discussion:
The case is reported for its exuberance, rarity and diagnostic complexity. Type IV hypersensitivity reactions such as the ones described, mimetizing recurrence of neoplastic processes, are very infrequent. Titanium is usually well tolerated, but in cases of persistent inflammation this diagnosis must be considered.
The inert character, strong resistance and biocompatibility to produce a protective oxide layer of Titanium make it a superior commodity(1). Titanium is currently used as biologic implant material across surgical specialties, especially in metal-sensitive individuals (2). Titanium alloys have been used for dental implants, endoprostheses, pacemakers, stents, eyeglass frames...(6).
Metal allergies are becoming more recognized within the surgical field. Allergic responses to metals such as nickel or cobalt are widely recognized(3), but allergy to Titanium is a rare occurence(1, 5) .. Titanium allergy diagnosis is typically based on medical history, clinical findings, and the results from patch testing (7). However, positive patch test reactions to Titanium materials are extremely rare(2) and a metal allergy to Titanium can occur even when the results of skin patch tests are negative(5).
Following the diagnosis of an allergic response to Titanium, the approach varies depending on the patient profile – including immunosuppressants, removal of Titanium hardware, stabilizing the affected site(1)…
This case highlights that, although Type IV hypersensitivity reaction secondary to Titanium that mimics cancer recurrence is a rare diagnosis of exclusion, in cases of persistent unexplained inflammation with a past medical history of metal surgical clips or implants, this diagnosis must be considered.
Detailed history and clinical evaluation are essential and can potentially expedite the diagnostic pathway saving unnecessary procedures.
Patient consent
Written informed consent was obtained from the patient for publication of his clinical details and images.
Funding
No funding source.
Conflicts of Interests
The authors have no conflicts of interest to declare.
References
(1)Razzante M. et al (2019). Type IV Cell-Mediated Hypersensitivity Reaction Caused by Titanium Implant Following Double Calcaneal Osteotomy and First Metatarsal- Cuneiform Arthrodesis: A Case Report and Review of the Literature. The Journal of Foot and Ancle Surgery, Case Reports and series – volume 58, issue 5, P974-979
(2)Megan M. Wood and Erin M. Warshaw. (2015). Hypersensitivity Reactions to Titanium: Diagnosis and Management. Dermatitis. Feb 2015.7-25. http://doi.org/10.1097/DER.0000000000000091.
(3) S. Jain M. et al. (2021). Delayed Titanium Hypersensitivity and Retained Foreign Body Causing Late Abdominal Complications. Hindawi – Case Reports in Surgery. ID 5515401, https://doi.org/10.1155/2021/5515401
(4)Alduais Y, Zhang H, Fan F, Chen J, Chen B. (2023). Non-small cell lung cancer (NSCLC): A review of risk factors, diagnosis, and treatment. Medicine 102:8(e32899). http://dx.doi.org/10.1097/MD.0000000000032899
(5)Sakamoto K, Ando K & Noma D. (2014). Metal Allergy to Titanium Bars After the Nuss Procedure for Pectus Excavatum. Case Report. Ann Thorac Surg, 98:708–10
(6)Vijayaraghavan V, V. Sabane A & Tejas K. (2012). Hypersensitivity to Titanium: A Less Explored Area of the Research. J Indian Prosthodont Soc, 12(4):201–207
(7) Fage S., Muris J., Jakobsen S & Thyssen J. (2016). Titanium: a review on exposure, release, penetration, allergy, epidemiology, and clinical reactivity. Contact Dermatitis, 74, 323– 345