A Retrospective Observational Study on The Outcome of IVF Cycles in A Tertiary Care Centre: A Two-Year Database
A Retrospective Observational Study on The Outcome of IVF Cycles in A Tertiary Care Centre: A Two-Year Database
Dr. Mayuri More *1, Dr. Rohan Palshetkar 2, Dr. Manisha Nandi 3, Dr. Nandita Palshetkar 4,Dr. Hrishikesh Pai 5, Dr. Rishma Pai 6, Dr. Arnav Pai 7
1. Assistant Professor, D Y Patil School of Medicine, Navi Mumbai.
2. Associate Professor, D Y Patil School of Medicine, Navi Mumbai.
3. Fellow, Bloom IVF, Mumbai.
4,5. Medical Director, Bloom IVF, Mumbai.
6,7. Consultant, Bloom IVF, Mumbai.
*Correspondence to: Dr. Mayuri More, Assistant Professor, D Y Patil School of Medicine, Navi Mumbai.
Copyright
© 2023 Dr. Mayuri More. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 09 October 2023
Published: 19 October 2023
Abstract
Objective : In vitro fertilization (IVF) cycle success rate and impact on the live birth rate (LBR)
Study Design: Retrospective single-center observational longitudinal study.
Setting: Tertiary care centre (IVF clinic) in India, Navi Mumbai.
Population : Non-donor IVF patients.
Main outcome measures: positive bHCG and LBR in non-donor, non-cancer IVF cycles against type and causes of infertility, the number and quality of oocytes retrieved, D3 and D5 embryo transfers subgroup analysis associated with pregnancy outcomes.
Definitions of clinical outcomes: a positive β-hCG has been defined as a value ≥ 5 mIU/L [1], which indicates implantation. Clinical pregnancy (CP) is defined as the presence of gestational sac (GS) and fetal heart (FH) activity following a positive β-hCG value. Biochemical pregnancy (BP) is defined as the temporary rise in the level of serum β-hCG without G sac inside or outside the uterine cavity [2]. Biochemical pregnancy is defined as a pregnancy that fails to end up with clinical pregnancy. Abortions include miscarriage both in 1st and 2nd trimesters, which is defined as a pregnancy that failed to result in delivery [3], and (ectopic pregnancy) EP is defined as CP that occurs outside the uterine cavity. Live Birth (LB) is defined as the delivery of live babies after 28 weeks of gestation [4,5].
Results: From n=470 IVF cycles, the oocyte retrieved was: 0-10 oocytes in 259 (55.3%); 11-20 oocytes in 120 (25.6%); >20 oocytes in 80 (19.1%). The β-hCG value on day 14 was found to be positive in 49.8% of the study group of patients. FHR was present in 40.6% and pregnancy continued in 161 with live births (n=147).
A Retrospective Observational Study on The Outcome of IVF Cycles in A Tertiary Care Centre: A Two-Year Database
Introduction
In the year of 1978, the world witnessed the birth of Louise Brown, a culmination of decades of ardent scientific research in the field of reproductive medicine. Since then on, abundant breakthroughs in basic science and clinical medicine have paved the way towards an increase in the numbers of infertile couples with the chance of conceiving an healthy baby with the help of IVF cycles. Till date, a number of more than 2 million babies have been born globally through ART. The statistics of the Centers for Disease Control (CDC) has documented that 48 000 babies were born through ART in the United States, and 100 000 IVF cycles were performed in the year of 2003 alone.[6]
The early days of IVF to recent developments
Prior to the year 1978, patients with nonfunctioning fallopian tubes were largely regarded as sterile by their clinicians. At least one tube patent was necessary for the natural fertilisation to occur in vivo. Many patients with damaged fallopian tubes had previously resorted to reparative surgeries, or tuboplasty with the hopes of re-establishing a conduit for the viable gametes to transit. Unfortunately, very often these surgeries failed to give positive results.
Following various critically important and sentinel events, Steptoe and Edwards, along with several other contemporary scientists, were successful in the clinical achievement of pregnancy and their efforts further improved and refined their ongoing pioneering efforts. The initial experiences with unstimulated IVF cycles undertaken by Edwards, Steptoe, and Purdy in the year 1980 yielded an average of 0.7 oocytes per cycle and with an overall clinical pregnancy rate of 6% per cycle. Stimulated cycles with the administration of hMG prior to oocyte retrieval was studied extensively at the Jones Institute in the year 1983. Its widespread usage has paved the way towards dramatic improvement in oocyte yield per cycle and clinical pregnancy rates.
Today, IVF narrates for millions of live births worldwide and 1 to 3% of all births yearly in the United States and UK.[7] The ongoing increase in the demand for fertility treatments drives us towards further scientific research and development of newer technologies for optimizing IVF success and regimens. [6] In light of the recent advancements, it is important for proper evaluation of the effectiveness and success rate in terms of clinical pregnancy rates and live births per IVF cycle. Our study is a systemic review of a two-year data base focussing on the pregnancy rates in a tertiary care centre.
Objectives: estimation of the success of IVF/ICSI cycles in terms of success with regards to the biological efficiency from oocyte to embryos to a live birth.
Selection Criteria
- IVF/ICSI cycles with the use of homologous gametes
- Non-donor and non-oncology IVF cycles.
Materials and Methods
This is a retrospective longitudinal observational study. IVF and intracytoplasmic sperm injection (ICSI) non-donor and non-oncology IVF cycles performed during a 2-year period from 2020 to 2022.
Information was obtained on the number of fresh oocytes retrieved and embryos obtained, transferred and stored during the treatment period 2020–2022. The data on IVF cycles were stratified with accordance to the number and quality of the oocytes retrieved. Only IVF/ICSI studies with non-donor gametes were analysed. The dataset had the inclusion of the total number of oocytes collected and numbers of embryos (D3/D5 transfers) from 2019 to 2021 and the live birth database analysed thereby offers a feasible and reasonable estimation of the biological efficiency from oocyte to embryos to a LB.
Statistical Analysis
Data were entered into Microsoft Excel and statistical analysis was carried out in SPSS software version 17.0. Age and number of eggs retrieved were converted into categories and reported as percentages. Qualitative variables like type and cause of infertility, D3 and D5 transfer, M1, M2, AMH, pregnancy outcomes, status of beta HCG and live birth were presented as proportions. Bar diagram and pie charts were used for graphical representation of data.
The association between the age categories, type of infertility, cause of infertility, d3 and D5 transfer with the status of beta HCG and live birth was done with the chi squared teat and a p value of less than 0.05 was considered as statistically significant.
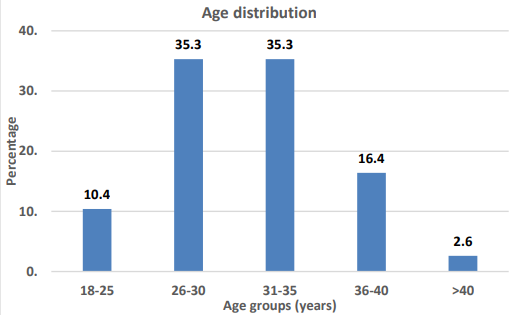
Figure 1: depicts the age distribution with 70.6% of patients within the age group of 26-35 years of age and remaining 10.4% less than 25 years and 2.6% above 40 years of age.
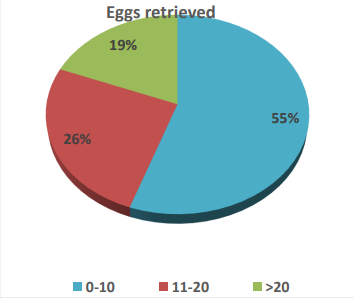
Figure 2: Graphical distribution of number of the number of oocytes retrieved with 55% <=10; 26% : 11-20; and >20 in 19% of the study participants.
Table 3 : Number of M1 and M2 oocytes retrieved.
Table 4: depicts the number of D3 and D5 embryo transfers with 11% (n=50) and 89%(n=420) respectively.
Table 5: depicts the pregnancy outcomes with relation to presence of FHR on ultrasound (40.6%); FHR absent in 8.9%; and ectopic gestation in 0.2% of the participants
Table 9 depicts the correlation of the parameters: age group of the participants, type of infertility, D3 and D5 transfers with beta HCG values. Age group between 26-30 (n=98); 31-35 years (n=74); 36-40 years(n=26); >40 years(n=3); <26 years(n=33) : 59%; 44.6%; 33.8%; 25%; 67.3%with positive β-hCG respectively, (p value 0.001).
Type of infertility: primary (n=188); secondary(n=46): 49.6% and 50.5% with β-hCG positive respectively. P value 0.78
D3 transfers in 205 patients and D5 transfers in 29 patients with positive β-hCG in 48.8% and 58% respectively with a p value of 0.07 for D3 embryo transfers and 0.08 for D5 embryo transfers.
Table 10: Represents the association of live birth with age group of the study participants.
Results
Among the assessed cycles, n=470; 49.8% resulted in positive bHCG; with 147 live births; 43 resulted in 1st and 2nd trimester abortions; and ectopic pregnancy in 1(0.2%). In the analysis, 12 variables were assessed and eight variables were summarised into 4 components using the principle component analysis. Finally, the association of IVF outcome and the 10 variables were evaluated. Age and number of eggs retrieved were converted into categories and reported as percentages. Qualitative variables like type and cause of infertility, D3 and D5 transfer, M1, M2, AMH, pregnancy outcomes, status of beta HcG and live birth were presented as proportions. Bar diagram and pie charts were used for graphical representation of data.
The data collected lists the mean or frequency of the variables for both successful and unsuccessful deliveries. The unadjusted results are shown using the t test and chi-square test for continuous and categorical variables, respectively. The association between the age categories, type of infertility, cause of infertility, D3 and D5 transfer with the status of β-hCG and live birth was done with the chi squared test and a p value of less than 0.05 was considered as statistically significant.
The type of infertility for those who delivered successfully was significantly higher for primary infertility as compared to those with secondary infertility. The number of oocytes retrieved among cases with successful deliveries was higher than those with unsuccessful deliveries. Cases with successful deliveries were significantly of years younger. Male factor (133: 28.4%,), frequency of abortions (1st and 2nd trimester 30 and 13 respectively), and primary type of infertility (n=379, 80.6%). The tables and figures provide additional details of the patients’ characteristics.
Discussion
IVF cycles, in terms of success rates have dramatically improved over the few decades. The LBR per IVF cycle in patients using own eggs has significantly increased by 18%, with a steeper improvement even in the older age groups (above 40 years of age).
In 2019,16,310 babies were born through IVF/ICSI performed in New Zealand and Australia. There were 88,929 IVF cycles in 2019. Not all cycles resulted in embryo transfer, however those which did, has marked significant improvements in pregnancy outcomes. It was recorded significantly higher in younger patients– the live birth rate per embryo transfer was 35.1% for fresh and 34.1% for thaw cycles in patients between 30-34 years, whereas in patients older than 44 years, the LBR per transfer was 1.70% for fresh and 9.20% for thaw cycles. The improvement in the success rates are due to various factors, which includes advancements in laboratory technologies and improvements in the management of patients with infertility, for example lifestyle modifications, newer diagnostic tools, and in some cases surgical treatments prior to ART.[8]
Factors determining the success of IVF cycles
Various factors are known to affect ART outcomes which includes cause of infertility, age of patients and embryo quality. Determination of the influencing primary factors may potentially have an influence on the positive likelihood for the achievement of a successful IVF treatment cycle; this on the greater note, enables clinicians to formulate better decisions based on individual patient characteristics. Couples who failed treatments may experience adverse psychological issues. Therefore, it is essential for the proper assessment of the various factors associated with the outcome of IVF cycles and hence to determine the influencing factors.
Cause of infertility
Cause of infertility is considered to be an important variable which affects IVF outcomes. Nelson and Lawlor in their study had predicted LB and birth weight amongst the infants born from IVF cycles [9]. They concluded that male factor as the cause of infertility was significantly associated with a lower chance of successful pregnancy in patients who underwent IVF without ICSI. The primary factors found in association with failure of treatment was further evaluated by Bhattacharya and colleagues; their results demonstrated that poor fertilisation was more frequent amongst patients with male factor, tubal disease, and endometriosis[10]. Additionally, they observed that non-live births amongst those patients with male factor and tubal disease was significantly higher than those patients with unexplained infertility. It has been demonstrated earlier in several studies that the cause of infertility tends to play a role for determining poor to intermediate outcomes. Elizur and co-workers investigated the primary predictive factors for IVF/ICSI treatment pregnancy outcomes; and observed that the rate of delivery amongst those patients with male factor was higher than the other etiologies. In our study, the cause of infertility was observed as male factor accounted for 28.4%, PCOS in 29%, tubal factor in 18.8%, poor ovarian reserve in 16.6% and unexplained infertility was noted in 7.2% of the study participants.
AGE
Woman’s age is considered to be yet another significant factor with regards to the achievement of a successful clinical pregnancy. Till date, it has been debated that with the increase of age, the IVF outcomes tends to become worse. Amongst the infertile cases, the Society for ART (SART) has recently stated that 47% of embryo transfers amongst patients less than 35 years had resulted in successful deliveries. The proportion was 38% for women at 35-37 years, 28% for ages 38 to 40 years, 16% for 41 to 42 years and 6% for women older than 42 years. Nazemian and colleagues investigated age of the patient and its impact on IVF cycle outcomes[11]. They observed that for women younger than 25 years have lower fertilization rates and a decreased frequency of good quality embryos. In their clinical study, pregnancy and implantation rates, were found to be similar to those patients who were 30 to 35 years of age. In another research, Yan and colleagues. [12] investigated the various mechanisms by which maternal age tends to have an affect on the outcomes of IVF cycles. Women older than 40 years tend to have a disadvantaged IVF outcome with an increased rate of miscarriages. In our study 70.6% of patients were within the age group of 26-35 years,10.4% less than 26 years and 2.6% of the study participants were above 40 years of age. We observed a cumulative higher rate of clinical pregnancy rates in terms of live birth rate in the younger age group of patients i.e. less than 40 years.
The Judgment based on Oocyte Maturity
The success and outcome of IVF pregnancies depends on many factors, which includes the quality of the gametes, endometrial receptivity and immunological factors. Amongst them, the key factors which affects infertile patients are the steady decline in the number and quality of retrieved oocytes. With Accordance to the evaluation of the oocytes in terms of developmental and morphological characteristics , the oocytes are divided into 3 classes, mature oocytes (MII stage): disappearance of the endogenous oocyte cytoplasm and the 1st polar body is visualised in the perivitelline space; intermediate mature oocytes (MI phase): the endogenous oocyte cytoplasm disappears but the perivitelline space is not visualised initially in the polar body; immature oocyte (GV stage): germinal follicles are seen in the cytoplasm.[13] Based on the maturity criteria, the number of mature oocytes obtained in our study was M1 stage: 1-10; 11-20 and >20 in 31.6% ;39.7% and 28.7% respectively, M2 stage: 1-10; 11-20; >20 was observed on analysis in percentages of 71.1%, 20.9% and 8% respectively.
Rate of mature oocytes retrieved=the total number of retrieved mature oocytes/the total number of oocytes retrieved (%)
Serum AMH and its role in determining the success of IVF cycles:
The level of serum AMH has a positive correlation with the number of antral follicles (AFC). Various clinical studies have demonstrated that serum AMH level not only reflects upon the number of AFCs but also determines the quality of the retrieved oocytes [14,15]. Generally speaking, it is commonly believed that serum AMH is maintained and remains stable throughout the menstrual cycle of a woman [16]. Hence, AMH can be considered as one of the best indicators for the evaluation of the ovarian reserve of a woman. The role of serum AMH in ART has been one of the best research hotspots in terms of determining the outcomes of IVF cycles. COH plays a key part of ART and AMH plays an important role determining the success or failure of the treatment protocols. Various clinical studies have demonstrated that women with lower values of AMH have a higher tendency towards cycle cancellation and lower number of good quality oocyte retrieval owing to poor ovarian response[17]. Some studies have also commented on the correlation of serum AMH levels with the number of high quality oocytes retrieved, fertilization rate per cycle, the number of available embryos and clinical pregnancy rates [18]. However, the compound relationship between serum AMH and the number of eggs retrieved in infertile patients at different age groups is yet to be studied effectively[10].
Herein, in our study, we analysed the AMH levels and the number of retrieved eggs obtained by controlled ovarian hyperstimulation in patients of different age groups and investigated the factors affecting IVF-ETs. AMH levels were classified into low (<1.5), medium (1.6-3.5) and high (>3.5). 41.9% of our study participants had a serum AMH value of >3.5 (high responders);1.6-3.5 (medium responders) in 37.7%and 20.4% had serum AMH level <1.5(low responders).
Correlation of Serum β-hCG levels with pregnancy outcomes: blastocyst transfer compared to cleavage embryo transfer
Serum β-hCG levels are estimated on a fixed day post-embryo transfer and one β-hCG level may fit all. However, Zhang and colleagues. observed that serum β-hCG levels in pregnancies resulting from day 5 transfers were lower than day 3 transfers, which further suggested that a delay in embryo transfer can impair embryo development and implantation4. Theocharis and co-workers19 reported similar trends but with no statistical significance in their study, which claimed that serum β-hCG levels were highly predictive in terms of pregnancy outcomes after D5 transfer compared to D3 (cleavage embryo transfers). Although, Wang et al. 5 also demonstrated a strong predictive role of serum β-hCG on a fixed day post embryo transfer, their study did not report the overall average serum β-hCG levels in the study subgroups.20 In our study D3 and D5 embryo transfers had a positive β-hCG noted as 48.8% and 58% respectively. Our results seemed relatively homogeneous without considering blastocysts.
Association of live birth rates with various parameters in IVF cycles: prediction of pregnancy outcomes
The cumulative pregnancy rates and outcome analysis are proven to be useful methods for advising couples of the probability of IVF success. All 5209 IVF/ICSI cycles in 2391 patients at The University Hospital, London, Ontario, Canada, over a span of 10 years were studied. The cumulative clinical pregnancy rates were calculated using Life Table analysis. The Cox proportional hazards model (CPH) was applied to analyse the influence of various covariates. Egg retrieval and embryo transfer were observed in 84 and 67% of the initiated IVF cycles, respectively. There were 644 intra-uterine, 24 ectopic pregnancies, and 68 spontaneous abortions (10.6%)21,22. In our study the analysis demonstrated the number of patients with 1st trimester abortion (n=30); 2nd trimester abortion(n=13); pregnancy continued in 161 participants; live birth(n=147) and ectopic pregnancy (n=1).
Strength and limitations
To the best of our expertise, this study is one of the largest non-donor aggregate number of IVF treatment cycles demonstrating the association between the number and quality of oocytes retrieved, with pregnancy outcomes in terms of positive bHCG, biochemical pregnancies, abortions, stillbirths and LBRs, thus reflecting the efficiency of IVF practices. The dataset was independently obtained and analysed thus overcoming selection biases at various levels after ensuring a significant degree of applicability of the study results for future reference. The 2 years post oocyte retrieval follow-up offers a logical and reasonable timeline for FET to occur. Whilst it is highly desirable to have a prospective clinical RCTs, the size of the database in this study is unlikely to form a match for an aggregated dataset analysis.
Conclusion
Globally, each individual IVF cycle has a success rate of about 30-50% in patients between 30-37 years of age. In general, the more eggs collected per cycle, the higher the likelihood of success. Success is defined as having a live birth. This study indicated that successful delivery after ART is strongly dependent on various characteristics of the patients, which included total number of embryos, number of injected oocytes, cause of infertility, age of women, and outcomes of IVF cycles in terms of clinical pregnancy rates. Further clinical trials based on individualised treatment protocols are to be highlighted in the future to pave the way towards advancements in IVF/ICSI cycles that can promise better outcomes and successful pregnancies in the near future.
Reference
1. Papageorgiou TC, Leondires MP, Miller BT, Chang AS, Armstrong AB, Scott LA, et al. Human chorionic gonadotropin levels after blastocyst transfer are highly predictive of pregnancy outcome1. Fertil Steril. 2001 Nov 1;76(5):981–7.
3. Lu M man, Wen Y xing, Liu Y liang, Ding C hui, Zhou C quan, Xu Y wen. Trophectoderm biopsy reduces the level of serum β-human chorionic gonadotropin in early pregnancy. Fertil Steril. 2020 Oct 1;114(4):801–8.
4. Zhang X, Barnes R, Confino E, Milad M, Puscheck E, Kazer RR. Delay of embryo transfer to day 5 results in decreased initial serum β-human chorionic gonadotropin levels. Fertil Steril. 2003 Dec 1;80(6):1359–63.
5. Wang Z, Gao Y, Zhang D, Li Y, Luo L, Xu Y. Predictive value of serum β-human chorionic gonadotropin for early pregnancy outcomes. Arch Gynecol Obstet. 2020 Jan 1;301(1):295–302.
6. Wang J, Sauer MV. In vitro fertilization (IVF): a review of 3 decades of clinical innovation and technological advancement. Ther Clin Risk Manag. 2006 Dec;2(4):355–64.
7. Chandra A, Copen CE, Stephen EH. Infertility service use in the United States: data from the National Survey of Family Growth, 1982-2010. Natl Health Stat Rep. 2014 Jan 22;(73):1–21.
9. Nelson SM, Lawlor DA. Predicting Live Birth, Preterm Delivery, and Low Birth Weight in Infants Born from In Vitro Fertilisation: A Prospective Study of 144,018 Treatment Cycles. PLOS Med. 2011;8(1):1–11.
10. Amini P, Ramezanali F, Parchehbaf-Kashani M, Maroufizadeh S, Omani-Samani R, Ghaheri A. Factors Associated with In Vitro Fertilization Live Birth Outcome: A Comparison of Different Classification Methods. Int J Fertil Steril. 2021;15(2):128–34.
11. Nazemian Z, Esfandiari N, Javed M, Casper RF. The effect of age on in vitro fertilization outcome: is too young possible? J Assist Reprod Genet. 2011 Feb;28(2):101–6.
12. Yan J, Wu K, Tang R, Ding L, Chen ZJ. Effect of maternal age on the outcomes of in vitro fertilization and embryo transfer (IVF-ET). Sci China Life Sci. 2012 Aug;55(8):694–8.
13. Sun XY, Lan YZ, Liu S, Long XP, Mao XG, Liu L. Relationship Between Anti-Müllerian Hormone and In Vitro Fertilization-Embryo Transfer in Clinical Pregnancy. Front Endocrinol [Internet]. 2020 [cited 2023 Aug 18];11. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7746804/
14. Iliodromiti S, Kelsey TW, Wu O, Anderson RA, Nelson SM. The predictive accuracy of anti-Müllerian hormone for live birth after assisted conception: a systematic review and meta-analysis of the literature. Hum Reprod Update. 2014;20(4):560–70.
15. Pilsgaard F, Grynnerup AGA, Løssl K, Bungum L, Pinborg A. The use of anti-Müllerian hormone for controlled ovarian stimulation in assisted reproductive technology, fertility assessment and -counseling. Acta Obstet Gynecol Scand. 2018 Sep;97(9):1105–13.
16. Younis JS, Iskander R, Fauser BCJM, Izhaki I. Does an association exist between menstrual cycle length within the normal range and ovarian reserve biomarkers during the reproductive years? A systematic review and meta-analysis. Hum Reprod Update. 2020 Nov 1;26(6):904–28.
17. Rotterdam ESHRE/ASRM-Sponsored PCOS consensus workshop group. Revised 2003 consensus on diagnostic criteria and long-term health risks related to polycystic ovary syndrome (PCOS). Hum Reprod Oxf Engl. 2004 Jan;19(1):41–7.
18. Badawy A, Wageah A, El Gharib M, Osman EE. Prediction and Diagnosis of Poor Ovarian Response: The Dilemma. J Reprod Infertil. 2011;12(4):241–8.
19. Serum hCG-β levels of postovulatory day 12 and 14 with the sequential application of hCG-β fold change significantly increased predictability of pregnancy outcome after IVF-ET cycle | SpringerLink [Internet]. [cited 2023 Aug 18]. Available from: https://link.springer.com/article/10.1007/s10815-016-0744-y
20. Zhang Y, Li Z, Ren B, Wu W, Liu Y, Wang X, et al. Diagnostic value of a single β-hCG test in predicting reproductive outcomes in women undergoing cleavage embryo transfer: a retrospective analysis from a single center. Reprod Health. 2022 Jun 22;19(1):145.
21. Alsalili M, Yuzpe A, Tummon I, Parker J, Martin J, Daniel S, et al. Pregnancy: Cumulative pregnancy rates and pregnancy outcome after in-vitro fertilization: >5000 cycles at one centre. Hum Reprod. 1995 Feb 1;10(2):470–4.
22. Werbrouck E, Spiessens C, Meuleman C, D’Hooghe T. No difference in cycle pregnancy rate and in cumulative live-birth rate between women with surgically treated minimal to mild endometriosis and women with unexplained infertility after controlled ovarian hyperstimulation and intrauterine insemination. Fertil Steril. 2006 Sep;86(3):566–71.