A Prospective Study of Cytomorphological Features of Cervical Lymphadenopathy in HBT Trauma Care Hospital, Jogeshwari, Mumbai
A Prospective Study of Cytomorphological Features of Cervical Lymphadenopathy in HBT Trauma Care Hospital, Jogeshwari, Mumbai
Dr Roshan Shaikh *1, Madhukar M Gavit 2
1,2. Senior Resident in Pathology Department at HBT Trauma Care Hospital, Mumbai.
*Correspondence to: Dr Roshan Shaikh. senior resident in the pathology department at HBT Trauma care hospital, Mumbai.
Copyright
© 2023 Dr Roshan Shaikh. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 11 October 2023
Published: 19 November 2023
Abstract
Cervical lymphadenopathy is one of the commonest presentations in inflammatory and neoplastic disorders. Fine needle aspiration cytology (FNAC) of lymph nodes is a simple, cost effective and minimally invasive out-patient procedure used for diagnosis of various causes of lymphadenopathies. This technique has high sensitivity and specificity which in addition to the establishment of cytological diagnosis, also helps to perform ancillary tests like ZN staining for AFB Bacilli and GeneXpert MTB/RIF Assay. In this study we describe cytomorphological patterns of FNAC of cervical lymph node and its utility in establishing diagnosis.
Material and Methods: In this study 40 patients presenting with lymphadenitis to the cytopathology lab for FNAC of lymph nodes of neck region for a period of one year between September 2022 to September 2023 were included. A detail history and Ultrasonography (USG) findings are noted. The cytomorphological features are compared clinically and on USG.
Statistical analysis and Results: Out of 40 patients, 35 (87 %) were adults (18-59 years) followed by 5 patients (13%) in the Children age group. 25 were females (62.5 %) and 15 were males (37.5%). The cervical group of lymph nodes were most commonly involved 27 (67.5%), submandibular 3(7.5%), submental 4 (10%) and posterior neck 6 (15%). History of contact with TB patient were 6 (15%), clinical suspicion of a tubercular aetiology were included in the analysis. On USG, out of 40 patients, necrosis seen in 13 (32.5%) followed by reactive lymphadenopathy 15 (37.5%) and infective lymphadenopathy seen in 7 (17.5%). Out of 40 patients presenting with lymphadenopathies, there were 28 (70%) cases of tuberculosis lymphadenitis out of which necrotizing granulomatous lymphadenitis were 15 (37.5%), granulomatous lymphadenitis 5 (12.5%), Suppurative lesions 8(20%) and 12 (30%) cases of reactive lymphadenopathy .
Conclusion: FNAC is a simple, cost-effective, outpatient technique with high diagnostic accuracy in cases of tubercular lymphadenopathy. In a developing country like India with a high prevalence rate of tuberculosis, FNAC is the first-line investigation in clinically suspected, diagnosed cases with tubercular lymphadenopathy.
Keywords: Cytomorphological pattern, Fine Needle Aspirate Cytology (FNAC), Cervical lymphadenopathy, Necrosis, Tuberculosis.
A Prospective Study of Cytomorphological Features of Cervical Lymphadenopathy in HBT Trauma Care Hospital, Jogeshwari, Mumbai
Introduction
Lymphadenopathy of cervical, axillary, and inguinal regions is a common clinical presentation in day-to-day clinical practice. There are diverse aetiologies of enlarged lymph nodes, ranging from benign reactive lymphadenopathy (viral or bacterial infections), including tuberculosis (TB) to metastatic carcinomas and lymphomas. Fine needle aspiration cytology (FNAC) without radiological guidance is a quick, effective and relatively inexpensive technique to evaluate visibly accessible superficial masses [1-2]. Although the diagnostic material obtained by FNAC is considered of inferior quality than trucut/core needle biopsy, especially for the diagnosis of lymphomas, however, there are many advantages of FNAC over trucut biopsy. First, it’s an office procedure and there is no specific need for any prior hematological workup. Second, material adequacy can be checked quickly, and repeat FNAC can be done at the same time. Moreover, FNAC has an extremely low complication rate.
The utility of diagnostic cytopathology is rapidly increasing in laboratory diagnostics [3,4]. Apart from rapid turnover time, the obtained material can be used for molecular studies. As cervical, axillary and inguinal lymphadenopathies are commonly encountered clinical problems, in this study, we evaluated the utility of FNAC for assessment of lymphadenopathy.
Material and Methods
A prospective study was conducted in the Department of Cytopathology, HBT Trauma care hospital Jogeshwari Mumbai. The duration of the study was one years from September 2022 to September 2023. A total of 40 cases were included in the study that underwent FNAC. The FNAC procedure was performed in the laboratory procedure room of the Cytopathology department, HBT Trauma care hospital. The FNAC procedure was done without radiological guidance for palpable lymph nodes of cervical region. After palpation, four to five passes were performed with a 22-23 gauge needle along with a plunger for FNAC. The obtained material was spread on four slides that were then stained with hematoxylin and eosin (H & E), Papanicolaou (PAP). If the diagnostic material was not present on the slides, another attempt of FNAC was performed. If the material was still inadequate, the third attempt of FNAC was performed after a gap of one day. The maximum number of FNAC attempts was third.
Statistical analysis and Results
Out of 40 patients, 35 (87 %) were adults (18-59 years) followed by 5 patients (13%) in the Children age group. 25 were females (62.5 %) and 15 were males (37.5%). The cervical group of lymph nodes were most commonly involved 27 (67.5%), submandibular 3(7.5%), submental 4 (10%) and posterior neck 6 (15% ), as shown below in table 1.
|
Sr. No |
Site |
No. Of cases |
Percentage |
|
1 |
Cervical |
27 |
67.5% |
|
2 |
Submental |
04 |
10% |
|
3 |
Submandibular |
03 |
7.5% |
|
4 |
Posterior neck |
06 |
15% |
|
|
Total |
40 |
100% |
Table 1. Distribution of cases according to Site;
History of contact with TB patient were 6 (15%), clinical suspicion of a tubercular aetiology were included in the analysis. On USG, necrosis seen in 13 (32.5%) and reactive lymphadenopathy 15 (37.5%), infective lymphadenopathy 7 (17.5%) , as shown in below table 2.
|
Sr. No |
USG Findings |
No of Cases |
Percentage |
|
1 |
Reactive lymphadenopathy |
15 |
37.5% |
|
2 |
Necrosis |
13 |
32.5% |
|
3 |
Infective aetiology |
07 |
17.55 |
|
4 |
Abscess |
03 |
7.5% |
|
5 |
Benign cystic lesions |
01 |
2.5% |
|
6 |
Neoplastic aetiology |
01 |
2.5% |
|
|
Total |
40 |
100% |
Table 2. Distribution of cases according to USG findings;
Out of 40 patients presenting with lymphadenopathies, there were 28 (70%) cases of tuberculous lymphadenitis out of which necrotizing granulomatous lymphadenitis 15 (37.5%), granulomatous lymphadenitis 5 (12.5%), Suppurative lesions 8(20%) and 12 (30%) cases of reactive lymphadenopathy, as shown in below table 3.
|
Sr. No |
Cytomorphological patterns |
No of Cases |
Percentage |
|
1 |
Necrotizing granulomatous lymphadenitis |
15 |
37.5% |
|
2 |
Granulomatous lymphadenitis |
05 |
12.5% |
|
3 |
Suppurative lesions |
08 |
20% |
|
4 |
Reactive lymphadenopathy. |
12 |
30% |
|
|
Total |
40 |
100% |
Table 3. Distribution of cases according Cytomorphological patterns;
Discussion
In this study, we found that FNAC is a highly diagnostic technique in the evaluation of superficial lymphadenopathy of cervical region. We also noted that tuberculous lymphadenitis was the most common reason for lymphadenopathy. Furthermore, in the younger age group, reactive lymphadenopathy was more common.
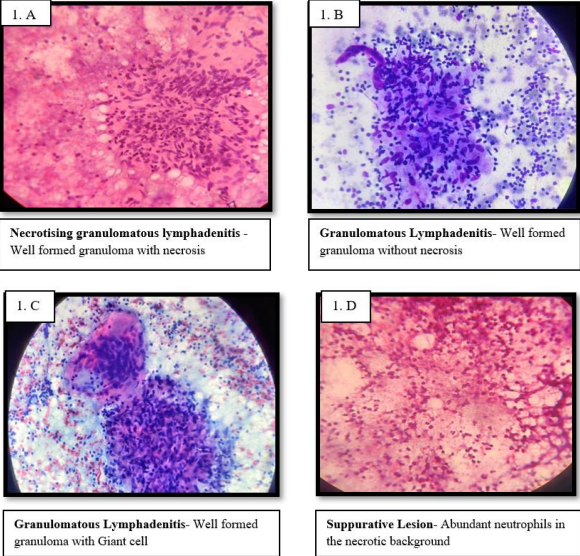
In our study, we observed that the categorization of the cause of lymphadenopathy into necrotizing granulomatous lymphadenitis, granulomatous lymphadenitis, Suppurative lesions and reactive lymphadenopathy could be reliably done by FNAC, (Figure 1& 2). A high sensitivity (71.4%) and specificity (91.5%) of FNAC was reported in previous studies for the evaluation of lymphadenopathy [5]. For patients with a known history of tuberculosis and tuberculosis contact in whom a subsequent enlargement of lymph node occurs, a cytological diagnosis of tuberculosis helps in avoiding unwanted surgical biopsy for confirming tuberculosis.
In our study we found that one case on USG has features of neoplastic aetiology but on FNAC it has features of reactive lymphadenitis. Similarly 15 cases on USG have features of reactive lymphadenitis out of which 12 cases cytomorphologically proved reactive lymphadenitis and remaining 3 cases have features of Tuberculosis on FNAC.
Tuberculous lymphadenitis was the most common cytological diagnosis on FNAC in our study. Cytologically, tuberculous lymphadenitis is characterized by caseation necrosis, epithelioid granulomas, and Langhans type giant cells (Figure 1.A, 1.B, 1.C)
A study evaluated 550 consecutive cases of TB diagnosed on FNAC. They noted that caseous necrosis with degenerated inflammatory cells in the background was the most common cytological pattern. They also found that cervical lymph nodes were the most common site and maximum incidence was in the third decade [6]. We also noted a higher frequency of TB in cervical lymph nodes with the most common occurrence in the 16-35 years age group. Another cytomorphological study investigating lymphadenopathy reported TB to be the most common cause of lymphadenopathy (44.02%), followed by reactive lymphadenitis (42.64%) and metastatic lesions (9.4%) [7].
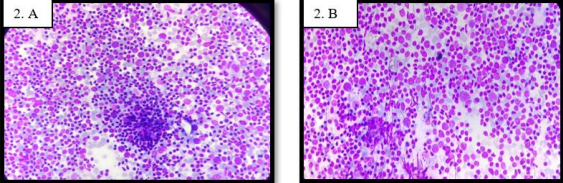
Cytological analysis of reactive lymph node reveals lymphoid cells with variable maturation intermixed with immunoblasts, and tingible body macrophages (Figure 2.A & 2.B).
Reactive lymphadenopathy was the second most common cause of lymphadenopathy in our study and was more frequently noted in the younger age group. These findings are consistent with other studies [8].
There were some limitations to our study. First, the biopsy and histopathological sections was not performed in all these cases to determine the sensitivity, specificity, and diagnostic accuracy of FNAC.
Conclusion
FNAC is an important tool for evaluating lymphadenopathy, as it is a simple, cost-effective, outpatient technique with high diagnostic accuracy in cases of tubercular lymphadenopathy. In a developing country like India with a high prevalence rate of tuberculosis, FNAC is the first-line investigation in clinically suspected, diagnosed cases with tubercular lymphadenopathy. Categorization of the cause of lymphadenopathy into necrotizing granulomatous lymphadenitis, granulomatous lymphadenitis, Suppurative lesions and reactive lymphadenopathy can be reliably done by FNAC, avoiding the need for truct/excisional biopsy. Furthermore, age, gender, and site of lymphadenopathy also provide useful information in predicting the cause of lymphadenopathy, as reactive lymphadenitis was more common in the younger age group, tuberculous lymphadenitis in middle age. Similarly, tuberculous lymphadenitis was more commonly noted in cervical lymph nodes.
References
1. Naz S, Hashmi AA, Khurshid A, Faridi N, Edhi MM, Kamal A, Khan M: Diagnostic role of fine needle aspiration cytology (FNAC) in the evaluation of salivary gland swelling: an institutional experience. BMC Res Notes. 2015, 8:101. 10.1186/s13104-015-1048-5
2. Asim M, Mudassir G, Hashmi AA, et al.: Diagnostic accuracy of fine needle aspiration biopsy in pediatric small round cell tumors. BMC Res Notes. 2018, 11:573. 10.1186/s13104-018-3678-x
3. Naveed H, Abid M, Hashmi AA, Edhi MM, Sheikh AK, Mudassir G, Khan A: Diagnostic accuracy of touch imprint cytology for head and neck malignancies: a useful intra-operative tool in resource limited countries. BMC Clin Pathol. 2017, 17:25. 10.1186/s12907-017-0063-y
4. Naz S, Hashmi AA, Ali R, Faridi N, Hussian SD, Edhi MM, Khan M: Role of peritoneal washing cytology in ovarian malignancies: correlation with histopathological parameters. World J Surg Oncol. 2015, 13:315. 10.1186/s12957-015-0732-1
5. Faro RO, Mohammed AZ, Atanda AT: Diagnostic utility of fine needle aspiration cytology in the evaluation of peripheral lymphadenopathy. West Afr J Med. 2018, 35:162-167.
6. Chand P, Dogra R, Chauhan N, Gupta R, Khare P: Cytopathological pattern of tubercular lymphadenopathy 2020 Hashmi et al. Cureus 12(12): e11990. DOI 10.7759/cureus.11990 8 of 9 on FNAC: analysis of 550 consecutive cases. J Clin Diagn Res. 2014, 8:16-19. 10.7860/JCDR/2014/9956.4910
7. Malhotra AS, Lahori M, Nigam A, Khajuria A: Profile of lymphadenopathy: an institutional based cytomorphological study. Int J Appl Basic Med Res. 2017, 7:100-103. 10.4103/2229-516X.205812