The Benifit Ofphrenic Nerve Pacemaker in the Individulas with Cervical Spine Injury.
The Benifit Ofphrenic Nerve Pacemaker in the Individulas with Cervical Spine Injury.
Nawar Alasaad*1, Tariq Al Ayed
*Correspondence to: Dr. Nawar Alasaad , Dr sulaiman al habib medical group, Saudi Arabia.
Copyright
© 2023: Dr Nawar Alasaad. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 12 October 2023
Published: 25 October 2023
Abstract
OBJECTIVE: patient with severe cervical spine injury, quadriplegia , dependent mechanical ventilation, right diaphragm paralysis , the patient tracheoostomid after 1 month of mechanical ventilation. This patient candidate to diaphragmatic pacemaker for possible weaning of ventilator.
SETTING: a case report about the benefit of diaphragmatic pacing in patient with spine injury in DR SULAIMAN AL HABIB MEDICAL GROUP CENTER , RIYADH SAUDI ARABIA.
METHOD: one patient with quadriplegia following high cervical traumatic spinal cord injury and ventilator–dependent chronic respiratory failure were implanted with a laparoscopic diaphragmatic pacemaker after preoperative assessments of his phrenic nerve function and diaphragm contractility through transcutaneous nerve stimulation.
INTERVENTION: patient supine position, under general anaesthesia ,the main trocar open technique through the infer umbilical area, other trocars under direct vision, division of the falciform ligament, the both sides of diaphragm were stimulated, insertion of 2 pacemakers in each side, tested both functioning well, connection of the wires after taken out and tunnelled.
RESULTS: The patient has shown satisfactory improvement after the procedure and we could gradually wean him of ventilator. The patient is off mechanical ventilation now. Furthermore, we blocked the tracheostomy then we could remove it successfully, and the patient is tolerating well and managing his upper airway without complications, he can speak too.
CONCLUSION: PNP in appropriate setting, clearly gives a benefits to these patients depended on mechanical ventilation.As discussed, principal among these are the avoidance of the machinery of mechanical ventilation and the associated facility of transport in and out of the home as well as to and from bed. Speech and olfactory sensation are improved.psychologically the patient was improved because was out of ventilator noise and can move out side.
Keywords: phrenic nerve , pacemaker, quadriplegia.ventilation.
The Benifit Ofphrenic Nerve Pacemaker in the Individulas with Cervical Spine Injury.
Introduction
In this report we present a patient had severe spinal cord injury with quadriplegia and chronic ventilator dependent , right phrenic nerve paralysis, he underwent to tracheostomy but still depend on mechanical ventilation , after implantation of diaphragm pacemaker through laparotomy we could disconnect him out of ventilator persistently then we could remove the tracheostomy.
The diaphragm is innervated by cervical nerves C3 to C5, but a patient may be able to mobilize the diaphragm with only partial innervation of the diaphragm(1).Testing diaphragm function may be accomplished with the “sniff test” of diaphragm eleva-tion under fluoroscopy. Further, electrodiagnostic testing of phrenic nerve function also may be used to show a response in diaphragm function(1).Diaphragm pacing has been shown to be an effective way of weaning and maintaining patients off of mechanical ventilation, thus lowering the care burden, and liberating the patient to be more mobile, and lessening the potential for morbidity(1).
Case Presentation:
An 11 years old sustained road traffic accident lead to cervical spine injury C5-C7 and quadriplegia.. The spine CT scan showed C 6-7 fractures with severe cord injury. The patient had maintained his upper airway and respiratory functions until 2 days before admission when he developed paradoxical breathing with respiratory distress. Therefore, he was intubated and connected to mechanical ventilation .The patient traneferred to our hospital from the referral hospital intubated.
After fixation, we tried to wean the patient of mechanical ventilation but we failed. A suspicion of diaphragmatic paralysis was raised, and a fluoroscopy study confirmed presence of right diaphragm paralysis compromising the normal breathing. A tracheostomy was done successfully 4 shily cuffed actually we tried to wean the ventilatory support after tracheostomy but we failed , so a laparoscopic diaphragmatic pacemaker was implanted.
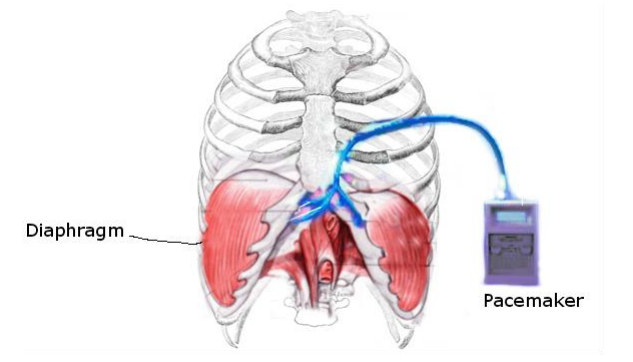
Figure 1
Discussion:
In 1777, Cavallo was the first to suggest electricity as a means for artificial respiration(2).
In 1818 Andrew Ure claimed that life could be restored in cases of suffocation, hanging, and drowning by stimulating the phrenic nerve (3).
In 1873 Hufeland was the first person to suggest that electrical stimulation of the phrenic nerve can lead to artificial respiration and can treat asphyxia. There was a long pause in work of phrenic nerve pacing despite the earlier success, which is mainly attributed to the advent of positive pressure ventilation(4). In 1940s Sarnoff et al. from Harvard University suggested that the absence of rhythmic diaphragmatic contractions can alter minute ventilation and henceforth result in an increase in carbon dioxide and a decrease in oxygen concentration. He described the new means of artificial respiration in which one or both phrenic nerves are stimulated by electrical current. He applied the current via a Grass stimulator set to deliver 40 impulses per second, with each impulse having a duration of two seconds. “The current was fed through a rotating potentiometer which describes an arc, the length of which can be set by an adjustable lever. The voltage can be regulated, and a gradual increase in voltage results in a smooth diaphragmatic contraction, which produces respiration. He also was able to perform 52 hours of phrenic nerve stimulation as an only means of artificial respiration in a five-year old patient with cerebral aneurysm leading to respiratory paralysis (5). William Glenn . from Yale University, along with his colleague, was the first to create the first practical application of phrenic nerve pacing. Their first clinical application of radiofrequency stimulation was done in 1964; it was a short-term application in the immediate postoperative period (6). Glenn and colleague mentioned phrenic nerve pacing in their paper in 1966 (7), though their seminal work on this topic was published in JAMA in 1968 on the use of radio-frequency electrophrenic respiration, a long-term application to a patient with primary hypoventilation syndrome (7). In collaboration with Dr. Glenn and Roger E. Avery, Glenn’s prototype was brought into commercial distribution by Avery Laboratories, Inc. in the early 1970s (8).
In 1987, Duchenne was the first to discover that direct stimulation of the phrenic nerve can lead to the contraction of diaphragm and imitate normal respiration (9); however, discussion about electrically stimulating the diaphragm and heart dates back almost two hundred years.
Flageole et al. (10) in 1995 described their experience with inserting phrenic nerve pacemakers in three children. In 2006 Hunt et al. (11) published their experience from Children Memorial Hospital in Chicago, Illinois, USA, of phrenic nerve pacemaker implantation among 34 infants and children since 1976. In 2002 Shaul et al. (12) described the thoracoscopic technique for phrenic nerve pacemaker implantation among nine children from 1997-2000. So far approximately 330 diaphragmatic pacemakers have been implanted among infants and children, and a total of approximately 2,000 diaphragmatic pacemakers have been implanted in over 20 countries. For approximately two decades, Dr. Onders and colleague from Cleveland clinic initiated the implantation of the diaphragmatic pacer. Over 150 spinal cord injury patients, including Christopher Reeves have been treated with NeuRx DPS TM (DPS: Diaphragmatic Pacing System) system in the USA(13). Onders et al. (14.15) reported the data of 88 patients’ experiences on the use of NeuRx DPS.
Outcome data in adults In an appropriately selected individual, the diaphragmatic pacemaker provides an opportunity for liberation from mechanical ventilation, either completely or partially. Moreover, by providing an opportunity for the normal negative pressure ventilation, and henceforth eliminating the adverse effects of positive pressure ventilation. Glenn et al. (16) reported their initial experience with phrenic nerve stimulation of 37 patients with quadriplegia in 1975. Full-time pacing was achieved in 13 patients, and in other ten patients ventilation was provided by pacing at least 50% of the time. In the remaining 14 patients in the series, ventilator support for 50% of the day could not be achieved. Eight of those patients died mainly from the complications of positive pressure ventilation. The main cause of failure to support ventilation was due to injury and subsequent damage to one or both phrenic nerves either from the initial trauma or operative manipulation. Malfunction of the pacemaker due to shorting of electronic components and antenna connector breakage also contributed to failure to pace or ineffective pacing. Another work by Glenn and colleague (17), reviewed the records of 477 patients who had undergone diaphragm pacemaker implantation for chronic hypoventilation. The data were from 1966 to 1988. Out of 477 patients, 165 patients were from multicenter study patients, 203 were from non-center study patients, and 109 patients were from non-study patients. Cervical cord injury and brain stem injury patients made the majority of patients . 47.27% of patients had success, whereas 34.54% of patients had significant support, and approximately 16% of patients had failure or minimal support. In another paper by Glenn et al. (18), they reported the long-term follow-up of pacing of the conditioned diaphragm in twelve quadriplegic patients. All twelve patients were successfully conditioned and they all were able to achieve full ventilation. In 1998 GarridoGarcia et al. (19)described a series of 22 patients who underwent placement of diaphragmatic pacemaker for the treatment of chronic respiratory failure. Thirteen of them had quadriplegia, five were status post-surgical treatment of intracranial lesion, and four patients had central alveolar hypoventilation syndrome. In their series, 81.8% of patients achieved permanent diaphragmatic paced breathing, whereas in 18.2% of patients it was done during sleep. On the long-term follow-up only two of the twenty-two patients were considered as failure. Garrido=Garcia et al. felt diaphragmatic pacemakers promote complete stable ventilation and improve the quality of life for patients. In 2002, Elefteriades and colleagues (20) reviewed the data on twelve patients who underwent implantation procedures between 1981 and 1987. They reported that 50% continued to pace full time with a mean duration of 14.8 years. Two (16%) patients died, one (8%) patient paced part-time, and three (25%) patients stopped pacing. Recently, Khong et al. (21) published an Australian series of 19 patients. Of those, 14 required phrenic nerve pacing due to quadriplegia, one had central hypoventilation syndrome, one had encephalitis, and the information on the remaining three was not known. Currently, 11 of the pacers are known to be actively implanted to date with a mean duration of 13 years. Outcome data in children from the information available, the first breathing pacemaker occurred on August 23, 1974 at St. Mary’s Hospital (Mayo Clinic) in Rochestor, Minnesota, (22) in a fifteen-year-old quadriplegic patient who is still being paced to date. In 1983 Brouilette et al. reported the case series of nine infants and children who underwent phrenic nerve pacing; five of those were less than one year of age. Seven of those were still alive at the time of publication. From August 1974 to June 2006, 324 diaphragmatic pacemakers have been implanted in children under the age of 18. Congenital central alveolar hypoventilation syndrome and quadriplegia account for approximately 75% of cases. gives the breakdown of the indication and average implant days among the pediatric population (22). Approximately 71% of the patients still have active working pacemakers, whereas 18% of the patients are deceased,
Phrenic nerve pacing in three infants with congenital central hypoventilation syndrome. The electrodes were implanted in the lower thoracic portion of each phrenic nerve. In all patients. bilateral simultaneous pacing was required to maintain an adequate arterial PO2, tidal volume, and minute ventilation during quiet sleep. Case 1 died of problems primarily related to the severe cor pulmonale that had been present before pacemaker insertion; at autopsy, the pacemaker system was intact and there were no significant phrenic nerve abnormalities. Case 2 later developed failure of awake ventilatory control and died because of extensive phrenic nerve damage incurred by 19 days of continuous pacing. Case 3 has received quiet sleep pacemaker support since September 1977 and has been able to maintain normal quiet sleep ventilation in this manner. Phrenic nerve pacing can be successful in infants as long as continuous pacing is not required (23).
A retrospective review was conducted of 14 consecutive patients with combined lesions of the cervical spinal cord and phrenic nerves, and with complete ventilator dependence, who were treated with simultaneous microsurgical nerve transfer and implantation of diaphragmatic pacemakers. Parameters of interest included time to recovery of diaphragm electromyographic activity, average time pacing without the ventilator, and percent reduction in ventilator dependence. Results Recovery of diaphragm electromyographic activity was demonstrated in 13 of 14 (93%) patients. Eight of these 13 (62%) patients achieved sustainable periods (>1 h/d) of ventilator weaning (mean = 10 h/d [n = 8]). Two patients recovered voluntary control of diaphragmatic activity and regained the capacity for spontaneous respiration. The one patient who did not exhibit diaphragmatic reinnervation remains within 12 months of initial treatment. (24).
References
[1] DiMarco AF. Phrenic nerve stimulation in patients with spinal cord injury. Respir
Physiolo Neurobiol 2009;169:200-9.
[2] Hufeland CW. De use vis electricae in asphyxia experimentis illustrato. Inaugraldissert. Gottingae 1873
[3] Spartacus Educational. www.spartacus.school.co.uk/IRue.htm. Accessed on 7/17/2010.
[4] Glenn WW, Judson JP. Radio-frequency electrophrenic respiration. Long-term application to a patient with primary hypoventilation. Journal of the Am Med Ass 1968; 203 (12): 1033-1037.
[5] Sarnoff SJ, hardenbergh E, Whittenberger JL. Electrophrenic Respiration. Science 1948; 108: 482.
[6] Glenn WW, Holcomb BE, Bernard J, Gee L, Rath R. Central hypoventilation; Long term ventilator assistance by radiofrequency electrophrenic respiration. Ann of Surg 1970; 172 94): 755-773).
[7] Glenn WW, Anagnostopoulos CE. Electronic pacemakers of the heart, gastrointestinal tract, phrenic nerve, bladder, and carotid sinus: Current status. Surgery, 1996; 60 (2): 480-494.
[8]Breathing Pacemaker. www.averylabs.com/breathing-pacemakers/introduction.html. Accessed on 7/4/2010.
[9] Duchene GB. De L’electrisation localisee et de son application a la pathologie et a le therapeutique par courants induits et par courants galvaniques interrompus et continues per le dr. Duchenne. Paris, Bailliere 1872
[10] Flageole H, Adolph VR, Davis M, Laberge JM, Nguyen LT, Guttman FM. Diaphragmatic pacing in children with congenital central alveolar syndrome. Surgery 1995; 118 (1): 25-28.
[11] Hunt CE, Brouillette RT, Weese-Mayer DE, Morrow A, Ilbawi MN. Diaphragm pacing in infants and children. PACE 2006; 11 (11); 2135-2141.
[12] Shaul DB, Danielson PD, McComb JG, Keens TG. Thoracoscopic placement of phrenic nerve electrodes for diaphragm pacing in children. J Ped Surg 2002; 37 (7): 974-978
[13] The NeuRx DPS. www.synapsebiomedical.com/products/neurx.shtml. Accessed on 7/12/2010.
[14] Onders RP, Elmo M, Khansarinia S, Bowman B, Yee J, et al. Complete worldwide operative experience in laparoscopic diaphragm pacing: results and differences in spinal cord injured patients and amyotrophic lateral sclerosis patients. Surg Endosc 2009; 23 (7): 1433-1440.
[15] Onders RP, Carlin AM, Elmo M, Sivashankaran SB, Schilz R. Amyotrophic lateral sclerosis: the Midwestern surgical experience with the diaphragm pacing stimulation system shows that general anesthesia can be safely performed. Am J Surg 2009; 197 (3): 386-390.
[16] Glenn WL, Holcomb BE, Shaw RK, Hogan JF. Long term ventilator support by diaphragm pacing in quadriplegia. Ann Surg 1976; 183 (5): 566-576.
[17] Glenn WL, Brouillette RT, Dentz B, Fodstad H, Hunt CE, Keens TG, Marsh HM, et al. Fundamental considerations in pacing of the diaphragm for chronic ventilator insufficiency: A multi-center study. PACE 1988; 11: 2121-2128.
[18] Elefteriades JA, Quin JA, Hogan JF, Holcomb WG, Letsou GV, Chlosta WF, Glenn WW. Long-term followup of pacing of the conditioned diaphragm in quadriplegia. PACE 2002; 25 (6): 897-906.
[19] Garrido-Garcia H, Alvarez JM, Escribano PM, Ganuza JR, Banda FL et al. Treatment of chronic ventilator failure using a diaphragmatic pacemaker. Spinal Cord 1998; 36: 310-314.
[20] Elefteriades J, Quin J. Diaphragm Pacing. Ann Thorac Surg 2002; 73: 691-692
[21] Khong P, Lazzaro A, Mobbs R. Phrenic nerve stimulation: The Australian experience. J of Clin Neuroscience 2010; 17: 205-208.
[22] Avery Biomedical Laboratory Company records. Avery Biomedical Devices Inc.
[23] Am Rev Respir Dis. 1978 Jul;118(1):23-8.
[24] J Reconstr Microsurg. 2015 Jun;31(5):391-5. doi: 10.1055/s-0035-1549159. Epub 2015 Apr 13.