To Study the Effect of Oral Vitamin D Supplementation in Dry Eye Patients in a Tertiary Eye Care Center
To Study the Effect of Oral Vitamin D Supplementation in Dry Eye Patients in a Tertiary Eye Care Center
Anurag Kumar Kashyap 1, *Diksha Sareen 2, Deepak Mishra 3, Archana Yadav 4,**OPS Maurya 2, SK Singh 5
- Fellow Sankara Eye Hospital, Kanpur-209217, Uttar Pradesh.
- Prakash Netralaya, Varanasi.
- Associate Professor, Regional Institute of Ophthalmology, Institute of Medical Sciences, Banaras Hindu University, Varanasi- 221005, India.
- Assistant professor, Department of Ophthalmology, Rama Medical College, Mandhana, Kanpur-209217.
- Professor, Department of Endocrinology, Institute of Medical Sciences, Banaras Hindu University, Varanasi- 221005, India.
*Cornea Consultant, **Consultant & Director.
*Correspondence to: Dr Archana Yadav, Assistant Professor, Department of Ophthalmology, Rama Medical College, Mandhana Kanpur, Pincode-209217, Uttar Pradesh.
Copyright
© 2023 Dr Archana Yadav. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 19 October 2023
Published: 01 November 2023
Abstract
Purpose: To establish association between serum vitamin D deficiency and dry eye disease and determine beneficiary effect of vitamin D supplementation in dry eye patients.
Methods: A randomized controlled clinical study was conducted in a hospital-based tertiary eye care center including 497 out-patients between age group 18-58 years. Patients were screened randomly for dry eye. Tear film break-up time (TBUT), schirmer’s test and Ocular surface disease index (OSDI) were used to diagnose dry eye.
Results: Forty patients were diagnosed with dry eye. After vitamin D supplementation in dry eye patients, TBUT and schirmer’s score was found to be significantly higher at 2 weeks (p < 0.001) and at 6 weeks of treatment (p < 0.001). Also, OSDI score was significantly lowered at 6 weeks of treatment (p < 0.001).
Conclusion: Supplementation of oral vitamin D improved tear secretion and reduced tear instability as indicated by development of schirmer's score and tear breakup time. Also, higher OSDI scores and lower TBUT value and schirmer’s scores in vitamin D deficient patients indicates positive correlation between serum vitamin D level and dry eye disease.
Key Words: Dry eye, vitamin D, tear film break-up time, schirmer’s test, ocular surface disease index scores, lacrimal functional unit.
To Study the Effect of Oral Vitamin D Supplementation in Dry Eye Patients in a Tertiary Eye Care Center
Introduction
Dryness of eyes is a multifactorial disease of the eye caused due to abnormalities in the tear film as well as ocular surface, which results in instability of tear film, with possible damage to the ocular surface [1]. A condition when the film is unable to provide required amount of moisture to the eyes is known as dry eye. Dry eye is characterized by redness, discomfort, stinging, itching, pain and tiredness in the eyes which may lead to vision blurring and light sensitivity[2]. Dry eye is more common in women and elderly population [3].
Lacrimal glands, ocular surface (cornea and conjunctiva), eyelids, meibomian glands, and associated nerves form the lacrimal functional unit (LFU). Dysfunction of any of the LFU component leads to dryness in eye which could be because of the changes in the volume, distribution, composition, and tear clearance [4]. Aqueous deficient dry eye is caused when less tear is formed by lacrimal gland while evaporative dry eye is caused due to inflammation of eyelid and meibomian gland dysfunction (MGD) [5,3].
Treatment for dryness in eye includes the use of lubricants, drugs having anti-inflammatory effects, occlusion of puncta and autologous serum6. Lubricating drops help relieve the discomfort in aqueous deficiency, but the inflammatory symptoms are not reduced [7]. A relation between serum vitamin D level and dry eye disease has been studied previously [8,9]. Though studies have established association between serum vitamin D deficiency and dry eye disease but the effect of supplementing vitamin D in dry eye patients lacks evidence.
The objective of our study is to find beneficiary effects of vitamin D supplementation in dry eye patients that may open new horizon in management of dry eye disease.
Methods
We have conducted a randomized controlled study from June 2018 to May 2019, involving 497 patients between age group of 18-58 years visiting tertiary eye care center presented with various ophthalmic complaints which may or may not involve dry eye symptoms. Patients were screened randomly for dry eye. The methodology includes patient’s history taking, general examination, visual acuity and refractive error evaluation, and thorough slit lamp examination. Dry eye was established in patients by taking specific tests as tear film break-up time (TBUT), schirmer’s tear secretion test and ocular surface disease index (OSDI).
Forty patients diagnosed with dry eye disease were included. Patients with corneal pathogenesis like corneal ulcer, degenerations, dystrophies, and history of previous intraocular surgery were excluded from the study. Sample size for the present study was calculated statistically and was found to be 20 in both groups [treatment group (group A) & control group (group B)]. All the screened cases were randomly allocated into 2 groups based on random allocation sequence. In addition to conventional dry eye treatment (0.5% carboxymethyl cellulose lubricating eye drops and ointments), treatment group was supplemented with oral vitamin D tablets (60,000 IU once a week for four weeks) while control group was kept only on conventional dry eye treatment. The study was approved by the institutional review board and ethics committee and complied with the tenets of the Declaration of Helsinki. An informed consent was taken in both the groups.
Statistical Analysis
Mean and standard deviation of pre and post-test of two important parameters namely TBUT and OSDI from prior published study12, the sample size was calculated assuming the probability of type I error alpha as 0.05 and power(1-ß) as 0.80. The sample size obtained was 19 and 17 respectively. Therefore, the sample size was considered as 24. Further anticipating 10% loss to follow up during study the required sample size for the present study will be 21(20) in each group. All the screened cases will be randomly allocated into 2 groups based on random allocation sequence. Paired t test was used to evaluate the mean, standard deviation, and p value for different variables. Results are being represented as mean standard deviation. Results corresponding to the value of p < 0.05 were considered as significant.
Results
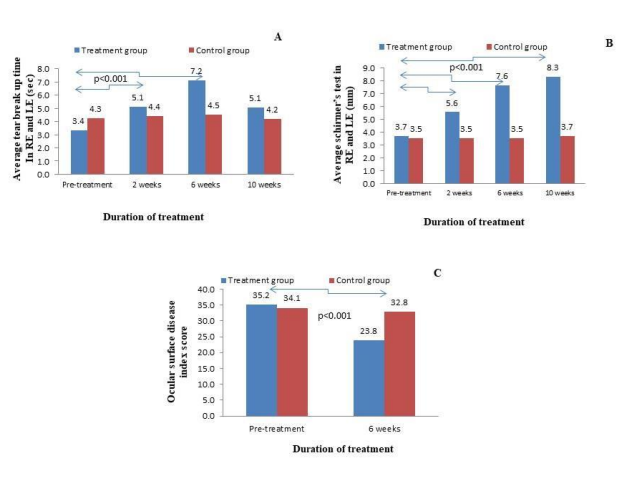
A total of 40 patients were included in the study (Table 1). Of these 20 patients were given oral vitamin D (group A, treatment group) and 20 patients were kept on conventional treatment and not given oral vitamin D (group B, control group). The mean age of the patients was 34.50 ± 13.50 years. There were 18 men and 22 women. Mean serum 25(OH) D level was 20.70 ± 5.91 ng/mL. The effect of vitamin D supplementation on DED patients in group A was assessed (Table 2, Figure. 1 [A-C]). TBUT RE and LE was found to be 3.35 ± 0.93 s and 3.45± 0.88 s at pre-treatment, increased to 5.10 ± 1.44 s and 5.01 ± 1.35 s after 2 weeks and to 7.45 ± 0.98 s and 7.15 ±1.27 s after 6 weeks respectively before returning to the pre-treatment levels after 10 weeks (p < 0.001, 0.001 and 0.001, respectively, paired t-test).
Tear secretion by schirmer’s test in RE and LE was found to be 3.70±0.80 mm and 3.75±0.78 mm at pre-treatment, 5.55 ± 0.82 mm and 5.80 ± 0.77 mm after 2 weeks, 7.64 ± 0.81 mm and 7.85 ± 0.74 mm after 6 weeks, and 8.30 ± 0.73 mm and 8.81 ± 0.77 mm respectively after 10 weeks (p < 0.001, 0.001 and 0.001, respectively, paired t-test). OSDI score was 35.2 ± 2.14 at pre-treatment, 23.85 ± 1.66 after 6 weeks (p < 0.001).
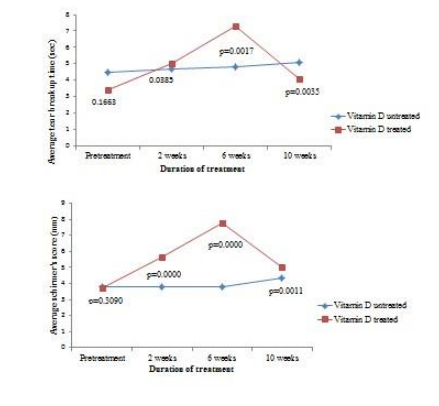
A comparison between the vitamin D treated and untreated group was performed by using t test two tailed paired depicted in Table 3. The average p value obtained for TBUT in vitamin D untreated and treated group was 0.1663 (not significant) at pre-treatment, 0.0385 (significant) at 2 weeks, 0.0017 (significant) at 6 weeks, and 0.0035 (significant) at 10 weeks. Similarly, the average p value obtained for schirmer’s score in vitamin D untreated and treated group was 0.3090 (not significant) at pre-treatment, 0.0000 (significant) at 2 weeks, 0.0000 (significant) at 6 weeks, and 0.0011 (significant) at 10 weeks. Figure 1A and 1B clearly showed that vitamin D supplementation increases TBUT and schirmer’s scores in vitamin D supplemented group than the vitamin D non supplemented group.
In group B, oral vitamin D supplementation was not given, hence no significant changes were observed in the parameters for improvement of dry eye (Table 2). However, conventional treatment was given to all the 40 dry eye patients with insignificant changes in the TBUT, schirmer’s tear secretion test and OSDI score in patients of group B.
Table 1: Demographic data of subjects
Table 2: The effect of vitamin D supplementation on dry eye disorder in treatment and control group
Table 3: Comparison of TBUT and Schirmer’s score between the vitamin D treated and untreated group
Figure 1. Association of vitamin D supplementation on dry eye disorder in control group (without oral vitamin D supplementation) and treatment group (Oral vitamin D supplementation). (A) Average break up time in right eye and left eye in treatment group showed significant increment at 2 weeks and 6 weeks in comparison to control group showing improvement in dryness before returning to pre-treatment level after 8 weeks. (B) Average schirmer’s test in right eye and left eye in treatment group showed significant increment at 2 weeks, 6 weeks in comparison to control group showing improvement in dryness before returning to pre-treatment level after 8 weeks. (C) Ocular surface disease index score significantly decreased after 6 weeks in treatment group in comparison to control group showing improvement in dryness.
Figure 2. Comparison of p value obtained for TBUT and schirmer’s score between the vitamin D treated and vitamin D untreated group at different time interval.
Discussion
Dry eye is an ocular surface disease with characteristic loss of tear film stability, in which hyperosmolarity of tear film, inflamed and damaged ocular surface, and neurological disturbances play an important role in etiology[1].
To the body, vitamin D (particularly, D3) is a crucial nutrient. Vitamin D affects many parts of our body, if a number is to be given to it, it would be somewhere near 2000 individual parts, thus it is one of the highest researched drugs throughout the world. Virtually every cell of our body contains a receptor for vitamin D. Vitamin D deficiency is associated in dry eye has been proposed in several literatures [8,9].
In our study 47.5% of the participants were vitamin D insufficient and 52.5% of the participants were vitamin D deficient. Both the vitamin D insufficient and deficient groups had dry eyes as per schirmer's test and tear breakup time test. We established a negative correlation between serum 25(OH) levels and OSDI scores. Our findings go well with the study performed by P. Yildrim et al.[13], in which he established a link between vitamin D deficiency and dysfunctions in tear and dryness and negative correlation between vitamin D levels and OSDI scores.
Our result clearly shows that vitamin D deficiency decreases the TBUT and schirmer’s test values and may be associated with severity of dry-eye symptoms. Also, we noted supplementation of oral vitamin D improved tear secretion and reduced tear instability as indicated by development of schirmer's score and tear breakup time. This observation is well defended by the study performed by Watts et al[10]., and Hwang et al.[11], in which they investigated the role of vitamin D in dry eye disease patients.
Present study indicates a significant improvement in schirmer's score, tear breakup time and OSDI score in vitamin D supplemented group (group A) while there was an insignificant improvement in vitamin D non-supplemented group (group B). The possible explanation for insignificant improvements in group B patients was their treatment with conventional drugs. The obtained p value for the average TBUT and average schirmer’s score in the vitamin D treated group is significant than the vitamin D untreated group (Figure 2). Hence, we can say that vitamin D supplementation promotes tear secretion with improved symptoms of dry eye syndrome, which could be due to the enhancement of the tear film parameters and reduction of ocular surface inflammation.
Conclusion
In summary, a protective role is played by vitamin D in the development of dry eye. Supplementation of vitamin D improved dry eye symptoms, including ocular discomfort, soreness, redness, ocular fatigue, sensitivity to light and blurred sight. Vitamin D supplementation also reduced severity of dry eye disease and subjective symptoms including OSDI score. Hence, we can conclude that vitamin D supplementation is a beneficial and effective treatment in dry eye patients.
References
1. Craig JP, Nicholas KK, Akpek EK, Caffery B, Dua HS, Joo CK et al. TFOS DEWS II Definition and Classification report. Ocul Surf. 2017;15:276-83.
2. Vitamin D and Dry Eye, www.vitamindsupplement.com.
3. Lemp MA. Report of National Eye Institute/Industry Workshop on Clinical Trials in Dry Eye. CLAO J. 1995;21:221-32.
4. Michael AL, Gary NF. International Dry Eye Workshop Subcommittee. The definition and classification of dry eye disease: a report of the definition and classification subcommittee of the International Dry Eye Workshop (DEWS-2007). Ocul Surf. 2007;5:75-92.
5. Anat G, Hannah G, Bozorgmehr P, William F, Hermes F. Effect of a Mediterranean dietary pattern and Vitamin D levels on dry eye syndrome. Cornea. 2014;33(5):437-41.
6. Zheng X, Paiva CS, Li DQ, Farley WJ, Pflugfelder SC. Desiccating stress promotion of Th17 differentiation by ocular surface tissues through a dendritic cell-mediated pathway. Invest Ophthalmol Vis Sci. 2010;51:3083-91.
7. Mencucci R. Boccalini C, Caputo R, Favuzza E. Effect of a hyaluronic acid and carboxymethylcellulose ophthalmic solution on ocular comfort and tear-film instability after cataract surgery. J Cataract Refract Surg. 2015;41:1699-704.
8. Lin H. & Yiu SC. Dry eye disease: A review of diagnostic approaches and treatments. Saudi J Ophthalmol. 2014;28:173-181.
9. Galor A, Gardner H, Pouyeh B, Feuer W, Florez H. Effect of a Mediterranean dietary pattern and vitamin D levels on Dry Eye syndrome. Cornea. 2014;33:437-41.
10. Watts P, Sahai A, Kumar PR, Shamshad MA, Trivedi GK, Tyagi L. A prospective study to assess the role of vitamin D individually and in combination with cyclosporine in the treatment of dry eye in patients with deficient serum 25(OH)D levels. Indian J Ophthalmol 2020;68:1020-6
11. Hwang JS, Lee YP, Shin YJ. Vitamin D enhances the efficacy of topical artificial tears in patients with dry eye disease. Cornea 2019;38:304 10.
12. Bae SH, Shin YJ, Kim HK, Hyon JY, Wee WR, Park SG. Vitamin D supplementation for patients with dry eye syndrome refractory to conventional treatment. Scientific Reports. 2016;6:1-8.
13. Yildirim P, Garip Y, Karci AA, Guler T. Dry eye in vitamin D de?ciency: more than an incidental association. Int J Rheumatic Dis 2016;19(1):49-54.