Oral Verrucous Carcinoma: Case Report and Literature Review
Oral Verrucous Carcinoma: Case Report and Literature Review
Dr. Hussein Moussawi *
*Correspondence to: Dr. Hussein Moussawi, 4+ Years of experience in providing high-quality patient care who possesses extensive knowledge in dental treatments and techniques, Member of LDA, ITI member, Diploma in oral implantology, Saint joseph university Beirut, American board certified.
Copyright
© 2023 Dr. Hussein Moussawi. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 19 October 2023
Published: 28 October 2023
Abstract
Verrucous carcinoma is a rare, low-grade, well differentiated form of squamous cell carcinoma seen on skin and mucosa. It is a slow-growing and locally aggressive tumor whose standard treatment is surgery. Although it can develop in other anatomical sites, gingiva, buccal mucosa, and alveolar mucosa are the most commonly affected tissues in intraoral tissues. Verrucous carcinoma cells do not exhibit dysplastic characteristics, and mitosis is also nonexistent. Due to the dysplasia that was left close to the verrucous carcinoma following therapy, the recurrence incidence is significant. The differential diagnosis of this
neoplasm is difficult and requires clinic and pathologic data confrontation. Although OVC is illustrated as a benign lesion with minimum aggressive potential over a period of time it can evolve into SCC. Hence most appropriate management of ovc is early diagnosis and surgical excision of the lesion. This case involves a male patient who was diagnosed with verrucous carcinoma.
Key words: Metastasis, oral pathology, squamous cell carcinoma, verrucous carcinoma.
Oral Verrucous Carcinoma: Case Report and Literature Review
Introduction
Head and neck malignant carcinoma is the world's fifth most common cancer with incidence exceeding half a million annually (1).
A common clinical variant of squamous cell carcinoma called verrucous carcinoma manifests as a warty, exophytic overgrowth that is gray or white and slowly enlarging, usually on the gingiva or buccal mucosa, and is most frequently seen in older men. Verrucous carcinoma typically has a locally invasive pattern with few distant metastases and a favorable prognosis. Verrucous carcinoma is difficult to diagnose clinically and histopathologically because of the tumor's slow development and benign histology characteristics. (2)
OVC's complicated etiology is dependent on a number of variables. Strong correlations exist between OVC and oral microbiota, smoking, drinking alcohol, and eating areca nuts. (3)
OVC is linked to unfavorable prostheses, prior wounds and scars, and persistent inflammation. Additionally, it could be brought on by the worsening of premalignant lesions including odontogenic keratocyst, oral lichen planus, oral submucous fibrosis (OSF), and oral verrucous leukoplakia. (4)
The contentious and ambiguous pathogenic role of the human papillomavirus is of interest among other possible causes of OVC (HPV)(5)
Case Report
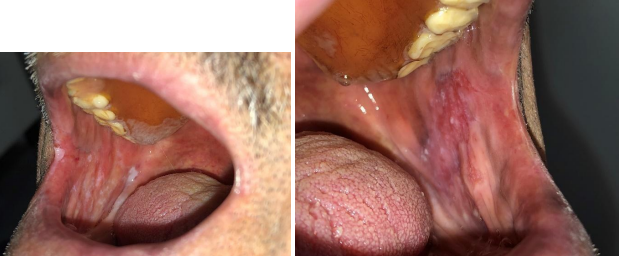
A 80-years-old male patient visited the Department of Oral Medicine and diagnosis with a chief complaint of a growth on the lower right in mental area in the past 6 months. No relevant medical or family history were contributory. The patient complained from a slow growing region (0.7 cm) which was asymptomatic except during eating. Patient is a heavy smoker and is completely edentulous with only an upper complete denture and nothing on the lower jaw in the past 3 years. OVD is significantly decreased. (Fig. 1-2) During oral examination two symmetrical white patches where found on buccal cheek mucosa. (Fig.3-4). Extra oral examination revealed pulpable submandibular lymph nodes (1cm) on both sides. Angular cheilitis is observed on the right side and there was limited in mouth opening.
Fig.1-2 Mixed red and white warty growth on the buccal aspect
Fig 3-4: Symmetrical white asymptomatic patches
On clinical examination, a sessile warty, pedunculated mixed red and white growth was present on the attached on the buccal side between the lower canine premolar region .The lesion is well-marginated. (Fig.2)
Panoramic x-ray and CBCT were done and there was no bone loss or involvement . With all the above findings a working diagnosis of proliferative verrucous leukoplakia in relation to left retromolar trigone was made and a differential diagnosis of verrucous carcinoma and verrucous hyperplasia were considered.
All haematological investigations were found to be within normal limits. Under local anaesthesia, incisional biopsy was performed which was suggestive of verrucous carcinoma. The specimen was sent for histolopathological evaluation. H&E section revealed hyperplastic parakeratinised stratified squamous epithelium with papillary projections and keratin plugging with cleft formation and wide, elongated rete ridges with pushing margins into underlying connective tissue These features reconfirmed earlier histopathological diagnosis. Hence considering clinical, radiographic and histopathological findings, a final diagnosis of verrucous carcinoma was given. Following treatment, patient is under follow up since last six months and prognosis is good.
Discussion
OVC often occurs in buccal mucosa, tongue, lip, gingiva, alveolar ridge and mouth floor(6)
OVC most commonly affects elderly male with adverse habits of tobacco and alcohol.(7) Association of Human Papilloma Virus infection and verrucous carcinoma has also been proved in various studies.(7-8) Other causative factors include smoking, snuff and alcohol usage, poor dental hygiene, poorly fitted dentures, low socioeconomic level, and tobacco chewing.(9) Leukoplakia was associated with OVC in 48% of the patients studied by Rajendran et al.(10) Most common site in oral cavity is buccal mucosa(61.4%) followed by (11.9%) (11) The contentious and uncertain pathogenic role of the human papillomavirus is of interest among other possible causes of OVC (HPV) (12).
There were one(4%), one(4%), nine(36%), and one(4%) cases in which HPV 6b/11 DNA, HPV 16 DNA, HPV 18 DNA, and HPV 16 DNA plus HPV 18 DNA were found, respectively.(13)
Papillary appearance and exophytic mass are its main clinical symptoms. OVC has a relatively favourable prognosis because of its sluggish growth, which contributes to a long medical history (up to several years), and because of the local aggression that causes rare regional or distant metastases.(14) OVC epithelial cells are well differentiated with weak cell atypia. In optical microscopy, the squamous epithelium of OVC shows highly proliferative, papillary appearance and excess aceratosis. The highly proliferative epithelial pegs show swelling and blunt ends in the shape of liquid droplets. All epithelial pegs are infiltrated to the connective tissue in the same depth, forming pushing borders(15) VC is comparable to many diseases in clinical and pathological conditions and deserves cautious differentiation, such as verrucous hyperplasia, squamous papilloma, and conventional squamous cell carcinoma(16) Abundant keratin production, papillary or verruciform surface and parakeratin plugs between the surface projections are seen with an intense infiltrate of chronic inflammatory cells in the connective tissue which were in accordance to histological features of our case. The histopathologic diagnosis of VC requires an adequate wide margin for incisional biopsy. Individual cells are not very dysplastic, thus the pathologist must carefully evaluate overall histomorphologic configuration of the lesion to arrive at an appropriate diagnosis(17)
There are many treatment modalities for VC are as follows: surgery(18) radiotherapy (19) photodynamic therapy, interferon (18) and chemotherapy (20) out of which surgical excision is the most preferred (21) It has excellent prognosis due to its slow growth and lack of metastasis.
Conclusion
Finally, although OVC is known as a benign lesion with minimum aggressive potential it may further progress to SCC in untreated cases, early diagnosis and surgical excision and long term follow up is required.
References
1. Jemal A, Bray F, Center MM, Ferlay J, Ward E and Forman D: Global cancer statistics. CA Cancer J Clin. 61:69–90. 2011. View Article : Google Scholar : PubMed/NCBI
2. Thomas GJ, Barre? AW. Papillary and verrucous lesions of the oral mucosa. Diagnosis Histopatholology 2009
3. Schutze M, Boeing H, Pischon T, Rehm J, Kehoe T, Gmel G, Olsen A, Tjønneland AM, Dahm CC, Overvad K, et al: Alcohol attributable burden of incidence of cancer in eight European countries based on results from prospective cohort study. BMJ
4. Gupta S, Kumar K, Raviprakash SM and Arunkumar KV: Ackerman's tumor of the oral cavity: A study of four cases with its conglomerate appearance. J Dent Specialities. 3:92–95.2015
5. Herrero R, Castellsagué X, Pawlita M, Lissowska J, Kee F, Balaram P, Rajkumar T, Sridhar H, Rose B, Pintos J, et al; IARC Multicenter Oral Cancer Study Group. Human papillomavirus and oral cancer: The International Agency for Research on Cancer multicenter study. J Natl Cancer Inst. 95:1772–1783. 2003
6. Waskowska J, Koszowski R, Raczkowska-Siostrzonek A and Stemplewska K: Verrucous carcinoma of the tongue-a rare case study. Cent Eur J Med. 7:145–148. 2012.
7. Oliveira DT, Moraes RV, FiamenguiFilho JF, FantonNeto J,Landman G, Kowalski LP. Oral verrucous carcinoma: a retrospectivestudy in Sao Paulo Region, Brazil. Clin Oral Invest2006;10(3):205–9.
8. Tornes K, Bang G, Stromme KH, Pedersen KN. Oral verrucous carcinoma. Int J Oral Surg 1985;14(6):485–92.
9. Kraus FT, Perezmesa C. Verrucous carcinoma. Clinical and pathologic study of 105 cases involving oral cavity, larynx and genitalia. Cancer 1966;19(1):26–38
10. Rajendran R, Sugathan CK, Augustine J, Vasudevan DM, VijayakumarT. Ackerman’s tumour (verrucous carcinoma) of theoral cavity: a histopathologic study of 426 cases. Singapore Dent J 1989;14(1):48–53
11. Walvekar RR, Chaukar DA, Deshpande MS, Pai PS, Chaturvedi P, KakadeAet al. Verrucous carcinoma of the oral cavity: A clinical and pathological study of 101 cases. Oral Oncol 2009;45:47–51
12. Herrero R, Castellsagué X, Pawlita M, Lissowska J, Kee F, Balaram P, Rajkumar T, Sridhar H, Rose B, Pintos J, et al; IARC Multicenter Oral Cancer Study Group. Human papillomavirus and oral cancer: The International Agency for Research on Cancer multicenter study. J Natl Cancer Inst. 95:1772–1783. 2003. View Article : Google Scholar : PubMed/NCBI
13. Noble-Topham SE, Fliss DM, Hartwick RW, McLachlin CM, Freeman JL, Noyek AM and Andrulis IL: Detection and typing of human papillomavirus in verrucous carcinoma of the oral cavity using the polymerase chain reaction. Arch Otolaryngol Head Neck Surg. 119:1299–1304. 1993
14. Alkan A, Bulut E, Gunhan O and Ozden B: Oral verrucous carcinoma: A study of 12 cases. Eur J Dent. 4:202–207. 2010.PubMed/NCBI
15. Karagozoglu KH, Buter J, Leemans CR, Rietveld DH, van den Vijfeijken S and van der Waal I: Subset of patients with verrucous carcinoma of the oral cavity benefit from treatment with methotrexate. Br J Oral Maxillofac Surg. 50:513–518. 2012
16. 1. Peng Q, Wang Y, Quan H, Li Y, Tang Z. Oral verrucous carcinoma: From multifactorial etiology to diverse treatment regimens (Review). Int J Oncol (2016) 49 (1):59–73. doi: 10.3892/ijo.2016.3501
17. Neville BW, Damm DD, Allen CM, Bouquot JE. Oral and maxillofacial pathology. 2nd ed. Philadelphia: W B Saunders; 2002. pp. 388–397.pp. 422–423.
18. Tippu SR, Rahman F, Pilania D. Verrucous carcinoma: A review of the literature with emphasis on treatment options. Indian J Stomatol. 2012; 3:22–26.
19. Pereez CA, Kraus FT, Evans JC, Powers WE. Anaplastic transformation in verrucous carcinoma of the oral cavity after radiation therapy. Radiology. 1996; 86:108–15
20. Rocco R, Addante, McKenna SJ. Verrucous Carcinoma. Oral Maxillofac Surg Clin North Am. 2006;18:513–19
21. Oliveira DT, Moraes RV, FiamenguiFilho JF, FantonNeto J, Landman G, Kowalski LP. Oral verrucous carcinoma: a retrospectivestudy in Sao Paulo Region, Brazil. Clin Oral Invest. 2006;10:205–09.