Insulin infusion therapy in hypertriglyceridemia induced acute pancreatitis: Retrospective Case series of Seven patients from a Specialist Hospital, UAE
Insulin infusion therapy in hypertriglyceridemia induced acute pancreatitis: Retrospective Case series of Seven patients from a Specialist Hospital, UAE
Diptendu Sengupta *1, Padmarajan Thankappan 2, Naveen. G. Naik 3
*Correspondence to: Diptendu Sengupta.
Copyright
© 2023 Diptendu Sengupta. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 25 October 2023
Published: 01 November 2023
DOI: https://doi.org/10.5281/zenodo.10074826
Abstract
Background and Objectives:
Triglyceride (TG) lowering therapy is imperative in hypertriglyceridemia induced acute pancreatitis (HTG-AP). Intravenous insulin with or without heparin, Plasmapheresis, CRRT and purified apo C? infusion are available regimens. However, there are no definite guidelines on first-line therapy. Plasmapheresis, CRRT and purified apo C? infusion may not be available at all centres managing patients with pancreatitis. We searched for keywords Hypertrigia, acute pancreatitis and Insulin infusion in PubMed, Medline, and Google Scholar databases. The search included articles published from January 1970 to October 2022 with no langulyceridemage restrictions. The search yielded 407 citations in English; 356 of the articles were excluded as they were not relevant; 29 articles were excluded since they were duplicates, leaving 22 articles. Full-text articles of the 22 citations were obtained and reviewed. Only two prior cases reported in literature were found wherein insulin infusion alone was used in the management of HTG-AP. This paper is a retrospective case series of 7 patients who presented to a specialist hospital in UAE with hypertriglyceridemic pancreatitis and their successful management with Insulin infusion therapy.
Keywords: Hypertriglyceridemia, acute pancreatitis, Insulin infusion.
Insulin infusion therapy in hypertriglyceridemia induced acute pancreatitis: Retrospective Case series of Seven patients from a Specialist Hospital, UAE
Introduction
Most common cause of acute pancreatitis (AP) in UAE is gall stones. The next common cause is Idiopathic. Other causes are hypertriglyceridemia, trauma, congenital anomalies, and medications. The incidence and mortality of hypertriglyceridemic (HTG)-AP are increasing on a yearly basis owing to diet and sedentary lifestyle of urban population [1]. Hypertriglyceridemic pancreatitis is notable for its severity and complications [2]. The management of hypertriglyceridemic pancreatitis entails decreasing the serum triglyceride level to less than 5.6 mmol/l as early as possible, apart from the basic care given to pancreatitis patients. Plasmapheresis purified apo C? infusion and hemofiltration (CRRT) are proven effective therapies but are not easily accessible [3]. Few case reports and one randomized controlled trial have reported that Insulin and heparin can enhance lipoprotein lipase activity and are cheaper alternatives for treatment [4,5,6]. Nevertheless, insulin therapy for hypertriglyceridemic pancreatitis is not widely practiced [8]. For hospitals with no access to plasmapheresis, CRRT and purified apo C? infusion management with intravenous insulin is a cost effective, safe and easily available option. There have been no previous publications from UAE on this modality of treatment.
Materials and Methods
Case records of patients who had been admitted to our hospital with a diagnosis of HTG-AP during duration between October 2021 and April 2023 were reviewed. These patients were treated with supportive measures and intravenous continuous infusion of regular human insulin.
Inclusion Criteria
AP was diagnosed when the patients presented with at least two of the following criteria:
- Acute pancreatic type abdominal pain.
- Serum lipase and/or amylase levels increased to three times the upper normal limit.
- Suitable imaging results (abdominal ultrasound and contrast-enhanced abdominal CT scan). HTG-AP was diagnosed if AP patients presented with a blood triglyceride level >11.3 mmol/L and other causes were excluded.
Results
Patient Characteristics
All 7 patients were males of South Asian (Bangladesh, India, Nepal and Pakistan) origin between 25 to 45 years working as labourers, with no history of prior alcohol intake. Out of 7 patients studied, 6 did not have a prior history of Diabetes Mellitus. One patient was known diabetic which was uncontrolled due to non-compliance to prescribed treatment.
Clinical Features
Patients presented mostly with severe central abdominal pain, associated with nausea, and vomiting of 1-3 days duration. All patients had tachycardia, diffuse abdominal tenderness, and sluggish bowel sounds.
Laboratory Findings
Plasma triglyceride levels were between 20-90 mmol/l and serum lipase was elevated (2000-9000 U/L). Abdominal contrast CT scan after 72 hours showed diffuse pancreatic swelling with a peri-pancreatic fat stranding and fluid collection in most patients (Table 1).
|
Patients |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
|
Age(yrs) |
25 |
36 |
28 |
33 |
45 |
37 |
43 |
|
RBS(mmol/L) |
19 |
28 |
17.5 |
23 |
31 |
43 |
37 |
|
TLC(Cells/mm3) |
14700 |
12720 |
13500 |
19600 |
11890 |
18100 |
15430 |
|
AST(U/L) |
43 |
57 |
38 |
110 |
82 |
72 |
61 |
|
ALT(U/L) |
56 |
75 |
47 |
135 |
87 |
83 |
77 |
|
SAP(U/L) |
188 |
190 |
212 |
230 |
175 |
201 |
180 |
|
Serum lipase(U/L) |
2550 |
3530 |
4186 |
8376 |
2130 |
5253 |
6547 |
|
HbA1C% |
6.90 |
7.5 |
8.20 |
9.30 |
6.6 |
7.1 |
7.3 |
|
Serum TG(mmol/L) |
54.94 |
24.57 |
24.94 |
48.6 |
34.57 |
52.3 |
82 |
|
CT Severity index |
5 |
3 |
4 |
6 |
3 |
5 |
4 |
|
Modified Marshall Score |
2 |
1 |
1 |
2 |
1 |
2 |
1 |
Table 1. Clinical and laboratory parameters of the patients with hypertriglyceridemia-induced acute pancreatitis
|
Day 1 |
Day 3 |
|
54.94 |
9.6 |
|
24.57 |
6.7 |
|
24.94 |
7.3 |
|
48.60 |
8.5 |
|
34.57 |
8.1 |
|
52.3 |
9.2 |
|
82.0 |
13.4 |
Table 2. Comparison between Triglyceride levels at admission and Post-treatment third-day
Triglyceride (mmol/L)
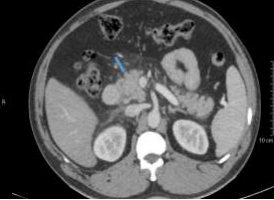
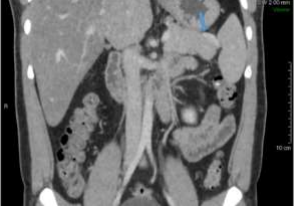
Radiological findings
USG findings revealed mild to moderate fatty infiltration of liver along with bulky pancreas in almost all patients.
CT abdomen with contrast was also done in all patients few of which are highlighted (Fig A,B,C & D)
A. Thin Arrow- Duodenum Thick Arrow- Pancreatic Head
B. Bent Arrow- Free Fluid; Thin Arrow- Duodenum; Thick Arrow –Pancreatic Head
C. Thick Arrow- Pancreatic Head; Thin Arrow-Peripancreatic Fat Stranding / Inflammatory Changes; Posterior Thin Arrow- Retropertoneal Renal Fascial Inflammatory Thickening
D. Thick Arrow- Pancreatic Tail; Thin Arrow- Subtle Peripancreatic Inflamatory Fat Stranding
Treatment and Outcome
With a diagnosis of HTG-AP, all these patients were managed in Intensive care unit. Patients were given Intravenous insulin infusion of regular human insulin at a rate of 0.1 units/kg/hour in normal saline.
Adequate hydration was given with Ringer lactate infusion and analgesia with intravenous Tramadol. Bowel rest was given for 12 to 24 hours followed by early enteral nutrition. Random blood sugar was monitored hourly. Electrolytes were monitored every 6 to 12 hours.
No episodes of hypoglycaemia were noted during therapy. Patients had reduction of symptoms within 12 –24 hours of Hospital stay and complete subsidence of symptoms were seen at end of 48 hours. Serum triglyceride levels dropped to less than 10 mmol/l in 2-3 days. No complications or mortality were noted. Mean Hospital stay ranged from 3-5 days. Follow up period ranged from 2-6 months; no long-term complications were noted.
Discussion
Common etiological factors for AP include Alcohol, gallstones, drugs, trauma and Idiopathic. HTG as an etiologic factor has been reported between 1.3% and 6.9% according to some studies [7,8]. However, the incidence of HTG-AP is increasing at a faster rate in the recent years. In a Danish study the incidence of HTG-AP has increased by 2.4 times over past 10 years [9]. Few other studies have shown that the incidence and mortality of HTG-AP are increasing with time which is probably related to change in diet and lifestyle [10]. Clinical manifestations of patients with HTG-AP are similar to pancreatitis due to other causes without any specificity. However, patients with HTG-AP have some atypical clinical characteristics, such as serum TG level (28.75 ± 26.0 mmol/L) that are significantly higher than normal values and associated Type 2DM, Essential hypertension and fatty liver disease (NAFLD) [11].
We found that the mean age of patients with HTG-AP was 33.54 ± 12.20 years. The highest incidence rate of HTG-AP was observed for men in the age group of 30-39 years. A large multi-centre study from China revealed higher incidence of local complications (34.13% vs 15.72%, P < 0.000) and MSAP (28.85% vs 12.95%, P < 0.000) in patients with HTG-AP than in patients without HTG-AP [12]. HTG-AP varies in severity between mild (41%), moderate (26%), and severe (33%) [13]. Some reports have shown a more severe course of AP induced by HTG compared with other causes, whereas other scholars seemed to favour no significant difference in disease severity [14].
Different studies reported that the mortality rate of HTG-AP ranged from 0.48% to 7.9% [10,16], but the mortality rate for severe cases reached as high as 20%-25%[2]. In this study, the frequency of SAP (14.2%), organ failure (27.5%), rate of recurrence (0 %), and mortality (0%) due to HTG-AP was unusually low. In our study the frequency of fatty liver disease, diabetes mellitus, and hypertension were found to be high with values of 90.6%, 100%, and 36.7%, respectively as reported in some other studies [15]. Modified Marshall score is routinely used to predict the severity of disease with a score of 3 or more indicating severe pancreatitis [17].
In our study however all patients had a score between 1 and 2 suggestive of mild to moderate pancreatitis. Rapid decrease of serum TG levels is imperative in the early treatment of HTG-AP and for reducing the severity as well as risk of local and systemic complications [18]. Treatment mainly includes two modalities - blood purification (Plasmapheresis/ CRRT) or insulin with or without heparin. Currently practice guidelines state that TG levels need be reduced to below 6.5 mmol/L as soon as possible which leads to reduction in the risk of clinical events and decrease in health care resource use and costs. [19,20].
However, selecting routine treatment or blood purification for patients with HTG-AP after admission to obtain economic cost effectiveness remains controversial. Routine treatments, such as insulin, heparin, and anti-HTG drugs, are effective in reducing TG and have the advantages of non-invasiveness and low cost [21].
In our study all patients were managed using insulin infusion resulting in rapid decline in TG levels followed by fibrates. None of the patients developed hypoglycemia or hypokalemia, two major complications associated with insulin infusion. All patients were pain free within 48 hours and were discharged within 3-5 days of admission. We avoided using Heparin infusion as it does not provide any additional benefit and can rarely lead to thrombocytopenia and life threatening haemorrhagic complications[22].
Vipperla et al [13] reported that the risk of recurrent AP attacks was 32%, often in patients with poorly controlled diabetes, alcoholism, and TG levels. Our study showed that there was no recurrence during a 3 month follow-up period. One drawback of this case series however is the absence of control group.
Conclusion
This case series supports the previous observations that, intensive insulin therapy is extremely effective in rapid lowering of TG levels. In addition it seems Intravenous Insulin is an effective, safe, readily available, and cheaper triglyceride-lowering therapy for HTG-AP compared to plasmapheresis, CRRT or purified apo C? infusion albeit more RCT’s and control groups are required to ascertain this conclusion. HTG-AP may be a presenting feature in previously undiagnosed patients of type 2 diabetes mellitus and associated metabolic syndrome was another interesting observation providing scope for further research and meta-analysis.
Reference
1. Xiao AY, Tan MLY, Wu LM, et al. Global incidence and mortality of pancreatic diseases: a systematic review, meta-analysis, and meta-regression of population-based cohort studies. Lancet Gastroenterol Hepatol. 2016;1(1):45–55. doi: 10.1016/S2468-1253(16)30004-8.
2. Li X, Ke L, Dong J, Ye B, Meng L, Mao W, Yang Q, Li W, Li J. Significantly different clinical features between hypertriglyceridemia and biliary acute pancreatitis: a retrospective study of 730 patients from a tertiary center. BMC Gastroenterol 2018; 18: 89 [PMID: 29914404 DOI: 10.1186/s12876-018-0821-z]
3. Tsuang W, Navaneethan U, Ruiz L, Palascak JB, Gelrud A. Hypertriglyceridemic pancreatitis: presentation and management. Am J Gastroenterol 2009; 104: 984-991 [PMID: 19293788 DOI: 10.1038/ajg.2009.27]
4. He WH, Yu M, Zhu Y, et al. Emergent triglyceride-lowering therapy with early high volume hemofiltration against low-molecular-weight heparin combined with insulin in hypertriglyceridemic pancreatitis a prospective randomized controlled trial. J Clin Gastroenterol. 2016;50(9):772–778. doi: 10.1097/MCG.0000000000000552.
5. Jain P, Rai RR, Udawat H, Nijhawan S, Mathur A. Insulin and heparin in the treatment of hypertriglyceridemia-induced pancreatitis [2] World J Gastroenterol.2007;13(18):2642–2643. doi: 10.3748/wjg.v13.i18.2642.
6. Alagözlü H, Cindoruk M, Karakan T, Ünal S. Heparin and insulin in the treatment of hypertriglyceridemia-induced severe acute pancreatitis. Dig Dis Sci. 2006;51(5):931–933. doi: 10.1007/s10620-005-9006-z.
7. Fortson MR, Freedman SN, Webster PD 3rd. Clinical assessment of hyperlipidemic pancreatitis. Am J Gastroenterol 1995; 90: 2134-2139 [PMID: 8540502]
8. Gullo L, Migliori M, Oláh A, Farkas G, Levy P, Arvanitakis C, Lankisch P, Beger H. Acute pancreatitis in five European countries: etiology and mortality. Pancreas 2002; 24: 223-227 [PMID: 11893928 DOI: 10.1097/00006676-200204000-00003]
9. Olesen SS, Harakow A, Krogh K, Drewes AM, Handberg A, Christensen PA. Hypertriglyceridemia is often under recognized as an aetiologic risk factor for acute pancreatitis: A population-based cohort study. Pancreatology 2021; 21: 334-341 [PMID: 33608229 DOI: 10.1016/j.pan.2021.02.005]
10. Khatua B, El-Kurdi B, Singh VP. Obesity and pancreatitis. Curr Opin Gastroenterol 2017; 33: 374-382 [PMID: 28719397 DOI: 10.1097/MOG.0000000000000386]
11. Carr RA, Rejowski BJ, Cote GA, Pitt HA, Zyromski NJ. Systematic review of hypertriglyceridemia-induced acute pancreatitis: A more virulent etiology? Pancreatology 2016; 16: 469-476 [PMID: 27012480 DOI: 10.1016/j.pan.2016.02.011]
12. Yin G, Cang X, Yu G, Hu G, Ni J, Xiong J, Hu Y, Xing M, Chen C, Huang Y, Tang M, Zhao Y, Cheng G, Wan R, Wang S, Wang X. Different Clinical Presentations of Hyperlipidemic Acute Pancreatitis: A Retrospective Study. Pancreas 2015; 44: 1105-1110 [PMID: 26348469 DOI: 10.1097/MPA.0000000000000403]
13. Vipperla K, Somerville C, Furlan A, Koutroumpakis E, Saul M, Chennat J, Rabinovitz M, Whitcomb DC, Slivka A, Papachristou GI, Yadav D. Clinical Profile and Natural Course in a Large Cohort of Patients With Hypertriglyceridemia and Pancreatitis. J Clin Gastroenterol 2017; 51: 77-85 [PMID: 27322530 DOI: 10.1097/MCG.0000000000000579]
14. Scherer J, Singh VP, Pitchumoni CS, Yadav D. Issues in hypertriglyceridemic pancreatitis: an update. J Clin Gastroenterol 2014; 48: 195-203 [PMID: 24172179 DOI: 10.1097/01.mcg.0000436438.60145.5a]
15. Jin M, Bai X, Chen X, Zhang H, Lu B, Li Y, Lai Y, Qian J, Yang H. A 16-year trend of etiology in acute pancreatitis: The increasing proportion of hypertriglyceridemia-associated acute pancreatitis and its adverse effect on prognosis. J Clin Lipidol 2019; 13: 947-953.e1 [PMID: 31735687 DOI: 10.1016/j.jacl.2019.09.005]
16. Murphy MJ, Sheng X, MacDonald TM, Wei L. Hypertriglyceridemia and acute pancreatitis. JAMA Intern Med. 2013 Jan 28;173(2):162-4. doi: 10.1001/2013.jamainternmed.477. PMID: 23183821.
17. Revised Marshall Score: A New Approach to Stratifying the Severity of Acute Pancreatitis; Dig Dis Sci doi: 10.1007/s10620-019-05719-y. Epub 2019 Jul 8
18. Anderson F, Thomson SR, Clarke DL, et al. Dyslipidaemic pancreatitis clinical assessment and analysis of disease severity and outcomes. Pancreatology 2009; 9: 252–257. [PubMed] [Google Scholar]
19. Berberich AJ, Ziada A, Zou GY, Hegele RA. Conservative management in hypertriglyceridemia-associated pancreatitis. J Intern Med 2019; 286: 644-650 [PMID: 31077464 DOI: 10.1111/joim.12925]
20. Galán Carrillo I, Demelo-Rodriguez P, Rodríguez Ferrero ML, Anaya F. Double filtration plasmapheresis in the treatment of pancreatitis due to severe hypertriglyceridemia. J Clin Lipidol 2015; 9: 698-702 [PMID: 26350817 DOI: 10.1016/j.jacl.2015.07.004]
21. Christian JB, Arondekar B, Buysman EK, Johnson SL, Seeger JD, Jacobson TA. Clinical and economic benefits observed when follow-up triglyceride levels are less than 500 mg/dL in patients with severe hypertriglyceridemia. J Clin Lipidol 2012; 6: 450- 461 [PMID: 23009781 DOI: 10.1016/j.jacl.2012.08.007]
22. Mark A. Crowther, Theodore E. Warkentin; Bleeding risk and the management of bleeding complications in patients undergoing anticoagulant therapy: focus on new anticoagulant agents; Blood (2008) 111 (10): 4871–487 https://doi.org/10.1182/blood-2007-10-120543.